- Always exclude other causes of the Febrile child
- Peak age prevalence is 6-18 months
- Exposure to cigarette smoke from household contacts is a known modifiable risk factor
Classification
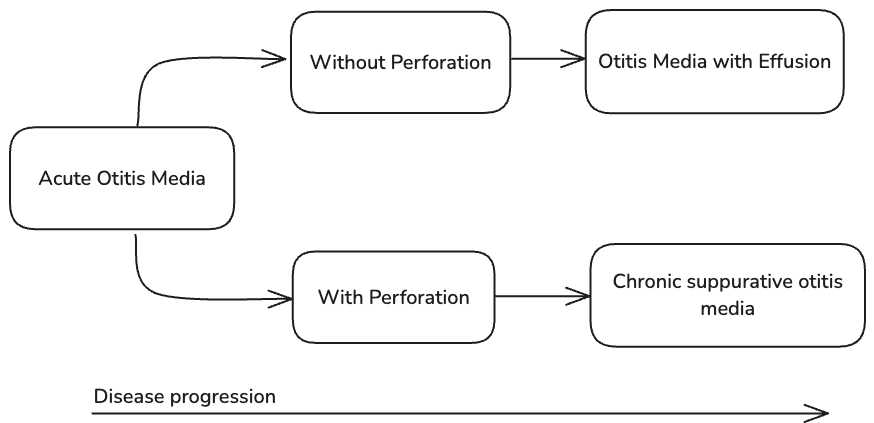
- Otitis media ⇒ inflammation or infection in the middle ear space
- Otitis media with effusion or serous otitis ⇒ middle ear effusion without infection; there are two types: persistent and episodic
- Episodic otitis media with effusion ⇒ middle ear effusion present for <3 months without inflammation
- Persistent (chronic) otitis media with effusion (glue ear) ⇒ middle ear effusion present for >3 month without inflammation
- Acute otitis media ⇒ Infection of fluid in the middle ear i.e. OME + infection
- Formally defined as middle ear effusion + ≥1 of the following:
- Bulging tympanic membrane
- Red tympanic membrane
- Recent discharge of pus
- Fever
- Ear pain
- Irritability
- Can be categorised into with and without perforation
- AOM with perforation (AOMwiP) ⇒ discharge of pus through a perforation in the tympanic membrane within the last 2 weeks
- Perforation is typically quite small initially when it first ruptures
- Note the size of the hole
- AOM with perforation (AOMwiP) ⇒ discharge of pus through a perforation in the tympanic membrane within the last 2 weeks
- Recurrent acute otitis media ⇒ ≥3 episodes of AOM within 6 months or ≥4 episodes in 12 months
- Formally defined as middle ear effusion + ≥1 of the following:
- Chronic suppurative otitis media (sometimes chronic mucosal otitis media) ⇒ perforated eardrum and discharge >6 weeks1
- Can think of it as on the worser spectrum of AOMwiP. Adequate management of AOMwiP will reduce progression to CSOM
- Should by definition have no features of fever or otalgia (if present consider other diagnoses: Otitis Externa, Acute Mastoiditis or intracranial involvement)
Aetiology
- Often preceded by a viral URTI
- Explain to parents that the Eustachian tube in children is shorter and more horizontal so infection happens from bacterial pathogens in the nasopharynx going to the ear through the Eustachian tube
- Bacterial pathogens:
- Steptococcus pneumoniae
- Haemophilus influenzae (less common due to vaccination)
- Moraxella catarrhalis
- If purulent consider can be caused by:
- Staphylococcus aureus or Pseudomonas aeruginosa
Risk Factors
- Risk factors for recurrent bacterial otitis media:
- Group child care
- Allergic rhinitis
- Adenoid disease
- Various structural abnormalities e.g. cleft palate, those associated with Down syndrome
- Exposure to smoke (e.g. cigarette, wood fires)
- Socioeconomic disadvantage (e.g. crowded housing)
- Ensure the child is up to date with Streptococcus pneumoniae vaccination (completed by 12 months)
Epidemiology
- Common: 90% of children have ≥1 episode and two thirds have ≥1 episode by 6 years old
- Peak incidence is between 6 and 24 months
Presentation
- Acute onset of fever and ear pain often preceded by URTI symptoms
- Includes: irritability, restless sleep and crying
- Purulent drainage from the ear may be present with AOM with tympanic membrane perforation or otitis externa
- See assessment of otalgia
Examination Findings
Transclude of Otalgia#^otoscopy-table
Management
Acute Otitis Media Management
- Symptomatic management
- See Paediatric Pain Management
- For severe acute ear pain consider
- Short term use of topical analgesia (e.g. 2% lignocaine or 1-2 drops of benzocaine + phenazone (Auralgen) applied to an intact tympanic membrane)
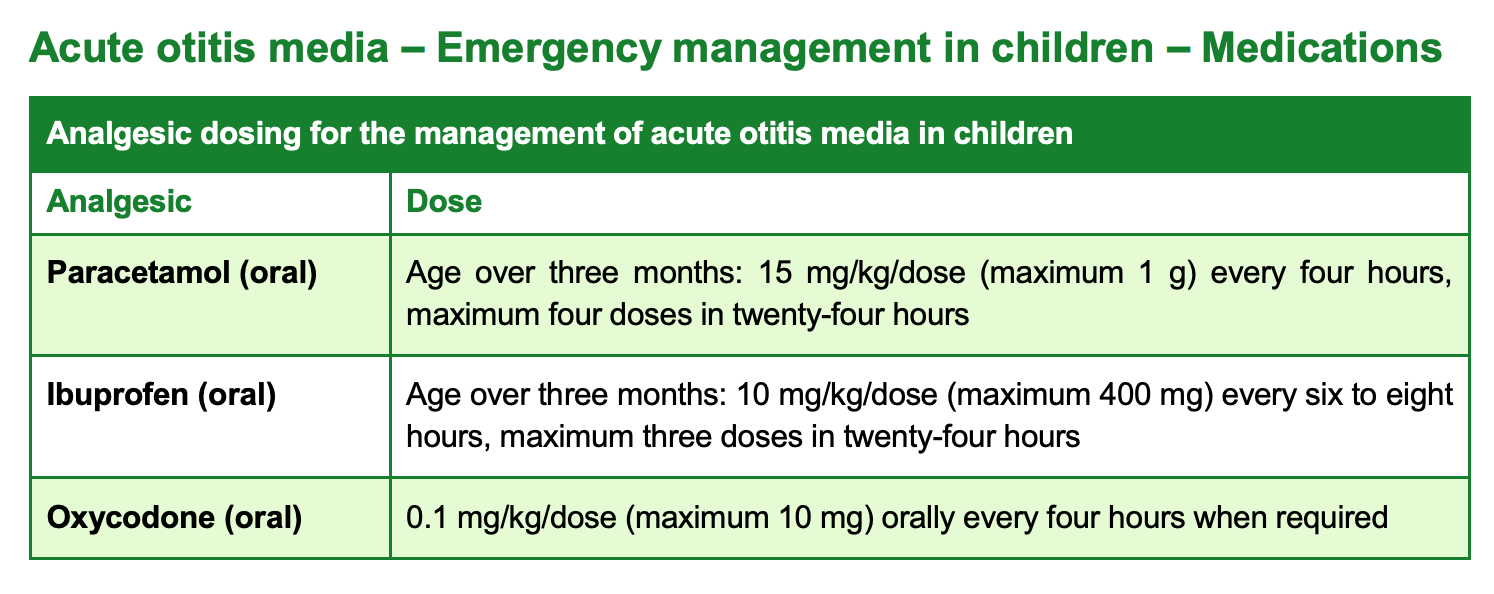
- QLD acute otitis media analgesia recommendations:
- Admission/Referral/High Risk Criteria
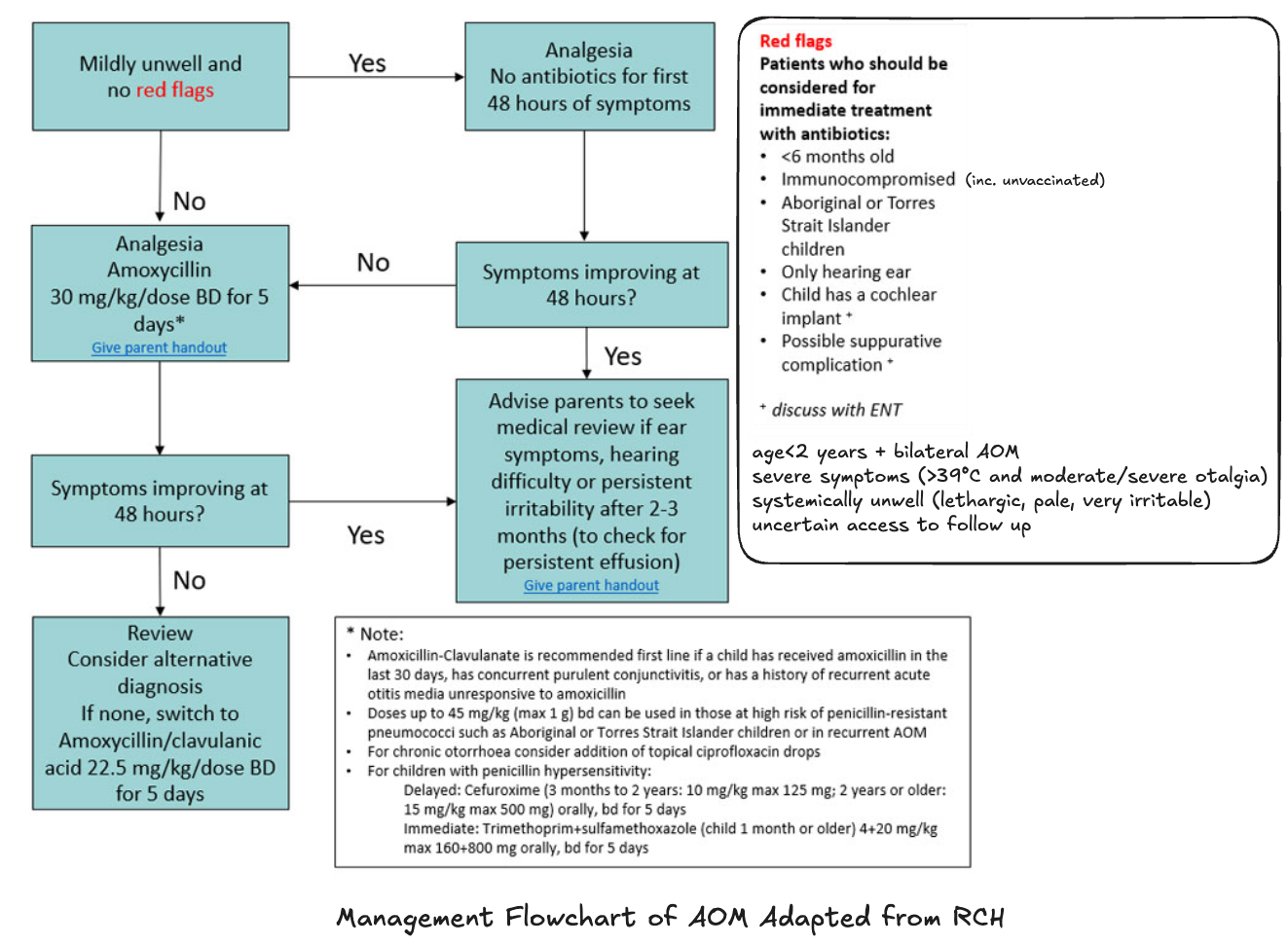
- Patients who should be considered for immediate treatment with antibiotics (see image below)
- <6 months old
- Immunocompromised
- ATSI
- Only hearing ear
- Child has cochlear implant → discuss with ENT
- Possible suppurative complication → discuss with ENT
- Patients who should be considered for immediate treatment with antibiotics (see image below)
- Non-pharm
- Avoid getting water in ear if perforated
- Pharm
- Antibiotic therapy
- Most cases of acute otitis media resolve spontaneously and antibiotics are not recommended
- For every 100 children treated with antibiotics, only five children will be better at 2 to 3 days as a consequence of taking antibiotics
- ABx therapy can cause harm including diarrhoea, rash and hypersensitivity reactions
- Refer to local guidelines for antibitoics
- NSW and SA (uses eTG):
- 1st line → Amoxicillin 15mg/kg up to 500mg PO 8-hourly for 5 days or Amoxicillin 30mg/kg up to g PO 12-hourly for 5 days
- If H. influenzae or M. catarrhalis suspected → Amoxicillin + clavulanate 22.5+3.2mg/kg up to 875+125mg orally 12 hourly for 5-7 days (older than >2 months old)
- Chronic otorrhoea → combine PO ABx with ciprofloxacin 0.3% ear drops, 5 drops in affected ear 12 hourly until free of discharge for ≥3 days
- Chronic suppurative otitis media (>6 weeks) ↓
- Clean the external ear by dry aural toilet before instilling ear drops
- Healthcare professsional: mechanical suction or, under direct visualisation, cotton wool on a probe
- Patient or carer: Roll corner of tissue and mopping the ear
- Ciprofloxacin 0.3% ear drops, 5 drops instilled into the affected ear, 12-hourly until the middle ear has been free of discharge for at least 3 days
- No need for PO antibiotics
- Clean the external ear by dry aural toilet before instilling ear drops
- QLD Paediatric antibiocard
- Amoxicillin 30mg/kg/dose every 8 hours (max 1g/dose) for 5 days
- Victoria (see RCH guidelines)
- WA (uses ChAMP PCH guidelines)
- Amoxicillin 15mg/kg/dose 8 hourly (max 1g) for 7 days; increase dose if no response after 4-7 days
- With perforation → amoxicillin 30mg/kg/dose (max 1g) 8 hourly for 14 days
- Persistent OME or recurrent AOM → oral amoxicillin 25/kg/dose (max 1g) 12 hourly
- Chronic suppurative otitis media ↓
- Clean and dry ear before each ear drop
- Topical ciprofloxacin 0.3% ear drops; 5 drops in the affected ear 12 hourly until free of discharge for at least 3 days
- NSW and SA (uses eTG):
- Most cases of acute otitis media resolve spontaneously and antibiotics are not recommended
- Antibiotic therapy
- Discharge planning, safety netting and follow up
- Return to your doctor if you experience any of the following:
- Severe ear pain with a headache
- An infection and you also have diabetes
- A worsening infection spreading around the outer ear and or the bone behind the ear
- Drooping of your face on the side of the ear infection
- Any other new symptoms affecting the muscle function of your face
- All children with perforation should be reviewed by a GP to ensure it has healed at around 10 days
- All children with AOM should be seen by their GP at three months to ensure the effusion has resolved
- Referral to ENT specialist may be considered for children who meet the following criteria:
- Effusion or perforation for more than 6 weeks
- Hearing impairment for more than 6 weeks
- Premature
- Indigenous or Torres Strait Islander background
- Flying recommendations
- Airlines recommend against flying if the passenger is unable to clear their eustachian tubes
- Children should be safe to fly two weeks after an adequately treated AOM, however many clinicians recommend waiting only 48 hours
- These children should be given a nasal decongestant at least 30 minutes prior to take-off and landing and analgesia prior to flying
- During take-off and landing they can be encouraged to suck, chew or swallow or, if old enough, perform a Valsalva manoeuvre to help equalise pressure
- Return to your doctor if you experience any of the following:
Complications of Acute Otitis Media
- Common
- Persistent middle ear effusion
- Tympanic membrane perforation
- Tympanosclerosis
- Other
- Cholestatoma
- Hearing loss
- Tinnitis
- Balance problems
- Facial nerve injury
- Unlikely but serious
- Mastoiditis
- Intracranial abscess
- Meningitis
- Venous sinus thrombosis
Otitis Media with Effusion Management
-
By 3 months 90% of effusions will resolve spontaneously
-
Effusion <3 months:
- If children has normal hearing and not at risk for speech or language problems → just observation
- Family education: Advise the family about the likely temporary hearing loss (usually around 20 dB) and the difficulty their child will have hearing speech, speech at a distance, and speech in background noise
- Discuss the importance of going to the health centre if their child develops ear discharge, pain, or if they have concerns about language development
- Review monthly recording date of each otitis media diagnosis
- Family education: Advise the family about the likely temporary hearing loss (usually around 20 dB) and the difficulty their child will have hearing speech, speech at a distance, and speech in background noise
- Refer to otolaryngolist if effusion is associated with speech delay or learning problems or structural damage to the tympanic membrane (e.g. significant retraction, cholestatoma) for consideration of tympanostomy tube or other interventions
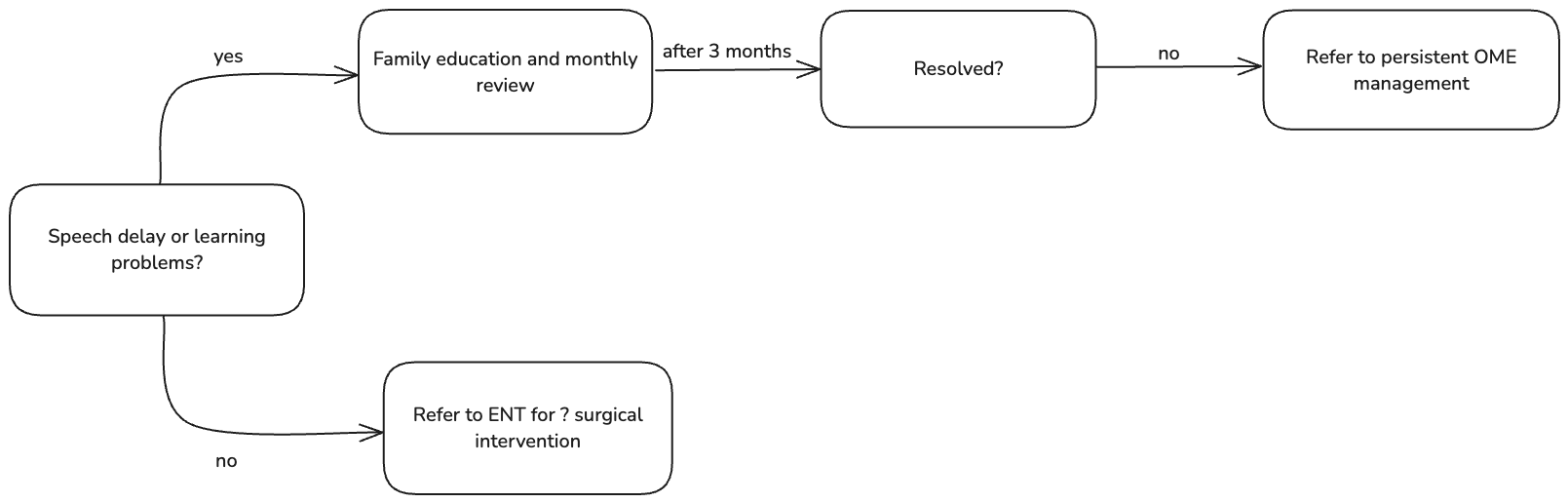
- If children has normal hearing and not at risk for speech or language problems → just observation
-
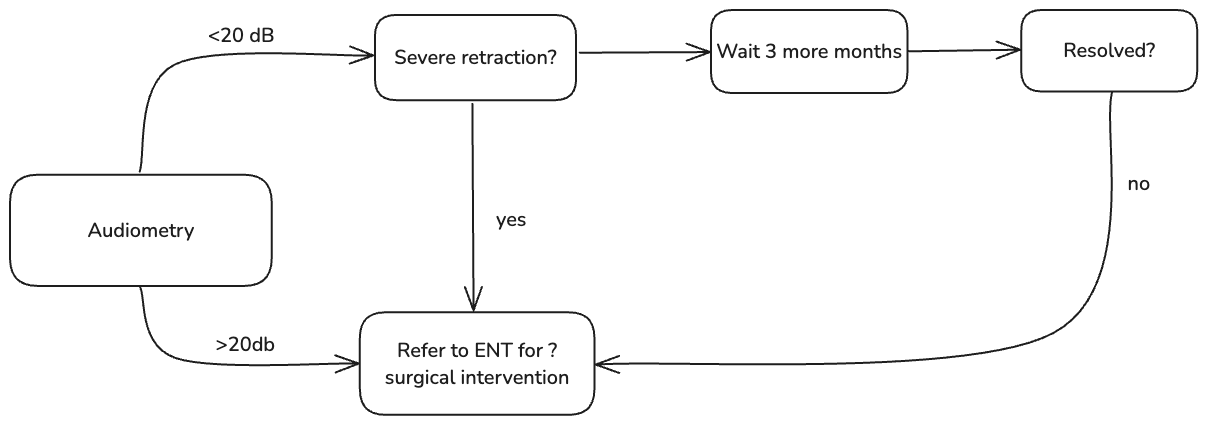
Effusion >3 months:
- Can present with conductive hearing loss or behavioural problems
- Refer all patients for audiometry
- Refer for ENT assessment if severe retraction of the tympanic membrane (i.e. retraction pocket or atelactsis)
- If hearing loss <20 dB suitable to wait a further 3 months and manage non-pharmacologically
- Review monthly to monitor for resolution
- Advise the family about the likely hearing loss (usually around 20 dB) and the difficulty their child will have hearing speech, speech at a distance, and speech in background noise
- Discuss the importance of going to the health centre if their child develops ear discharge, pain, or if they have concerns about language development
- School-aged children can have classroom sound-field amplification
- If hearing loss >20 dB or persistent OME for 3 months (6 months altogether) and/or speech and language delay → refer for ENT assessment for possible surgical intervention
- Refer children with hearing loss and speech delay to speech pathology
Sources
- RCH Guidelines
- Clinical Emergency Medicine Textbook
- eTG: Otitis Media
- Acute otitis media - emergency management qld guidelines
- Otitis Media Guidelines
Footnotes
-
Note that the otitis media guidelines for Aboriginal populations defines it as lasting ≥2 weeks and >2% of pars tensa has perforated ↩