Management
- Treatment of narrow-complex SVT is the same, irrespective of whether WPW is present (unlike SVT with aberrancy i.e. wide complex SVT))
- A broad-complex SVT with aberrancy from ventricular pre-excitation such as in WPW is treated the same as VT
- Unstable SVT: SVT with hypotension chest pain (angina), SOB (LV failure) or an altered mental state
- Call for senior help
- Apply high-flow oxygen by mask and gain IV access
- Attach the ECG monitor/defibrillator to the patient and confirm the rhythm
- Prepare procedural sedation such as propofol 200mg in 20mL IV and call an anaesthetist
- Once senior assistance is present, the treatment of choice is synchronised DC cardioversion beginning with 70-120J (biphasic) repeated up to three times
- Stable SVT (as in AVNRT or AVRT)
- Vagal manoeuvres
- Valsalva maneuvre:
- Place the patient in the Trendelenburg (foot of the bed up) position on a trolley
- Ask the patient to blow into the nozzle end of a 20 mL syringe for 10 seconds to try to force the plunger halfway up, then release suddenly
- Carotid sinus massage
- Check precautions below
- Turn the patient’s head to left and locate the carotid sinus just anterior to the sternocleidomastoid at the level of the top of the thyroid cartilage
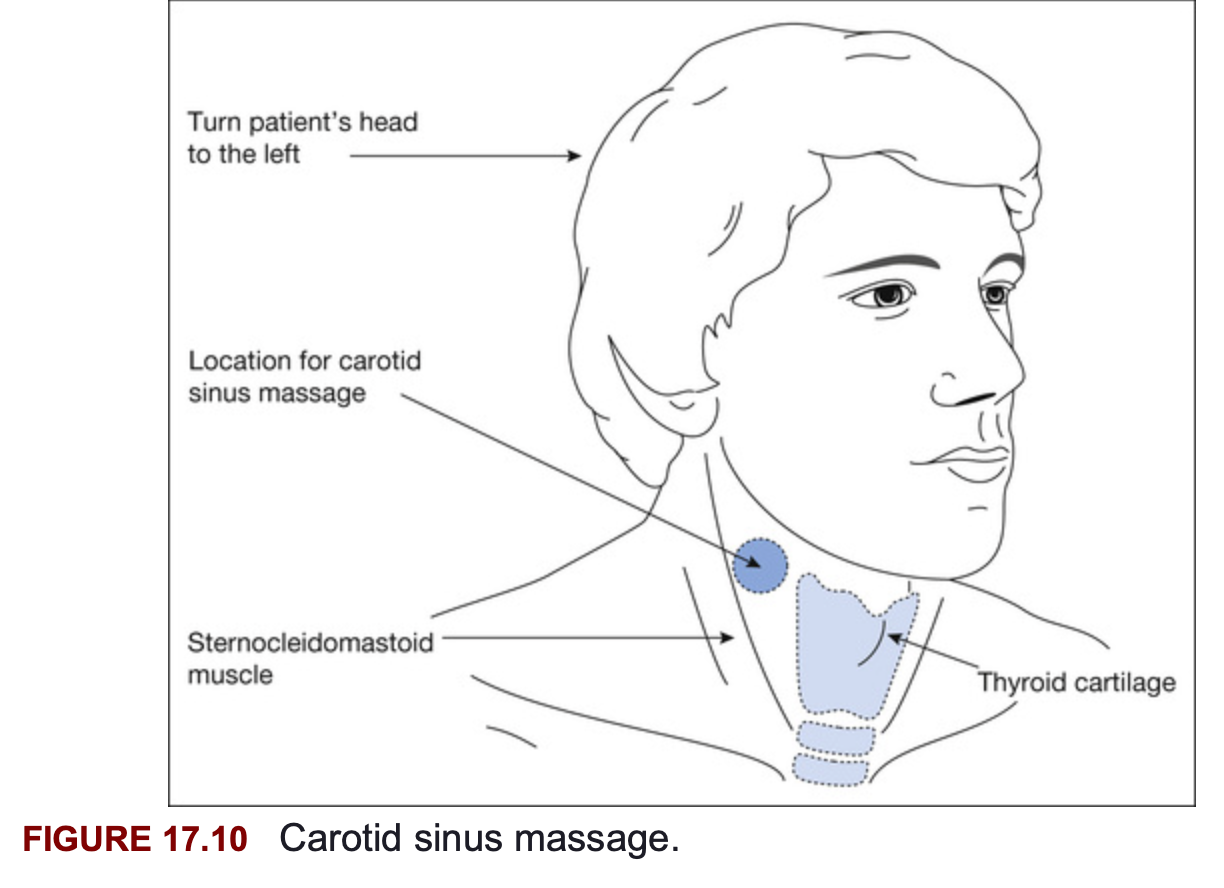
- Feel the carotid pulsation at this point and apply steady pressure to the carotid artery with two fingers for 10-15 seconds; try the right side and if this is not effective then try the left side (never perform bilateral massage)
- Drug therapy
- Adenosine
- Precautions in patients with COPD and asthma as it may precipitate wheeze and reduce dose in patients on dipyridamole
- Warn the patients of side effects as they are common and often poorly tolerated but are transient:
- Feeling of impending doom, also facial flushing, dyspnoea and chest pressure
- Make sure ECG monitoring
- 6mg as a rapid IV bolus followed by a 20mL saline flush
- If ineffective increase to adenosine 12mg IV push and repeat after 1-2 minutes if still no response
- Verapamil
- Verapamil 2.5-5mg IV over 1-2 minutes repeated every 5-10 minutes to a total dose of 15mg
- Verapamil may cause hypotension if injected too rapidly, so give slowly, particularly in the elderly
- It has a negative ionotropic effect
- Never give verapamil after a beta-blocker, when digoxin toxicity is suspected or if the patient has a wide-complex tachycardia; can cause fatal bradycardia
- If SVT still persists following verapamil, repeat the vagal manoeuvres
- Verapamil 2.5-5mg IV over 1-2 minutes repeated every 5-10 minutes to a total dose of 15mg
- Adenosine
- Valsalva maneuvre:
- Vagal manoeuvres
Carotid Sinus Massage Precautions
Always perform carotid sinus massage with IV atropine 600mcg available and continuous ECG monitoring as some patients develop asystole In some patients carotid sinus massage has resulted in stroke from carotid artery stenosis. Always listen over each carotid artery for bruit. Do not perform if there is any of:
- Carotid bruit or known carotid artery stenosis >50%
- TIA, stroke or AMI in past 3 months
- History of symptomatic bradyarrhythmias