- AVRT occurs in patients with accessory pathways and is due to the formation of a re-entry circuit between the AV node and the accessory pathway
- Pre-excitation features are lost in the ECG and may become apparent once reverted
- Pre-excitation features are lost in the ECG and may become apparent once reverted
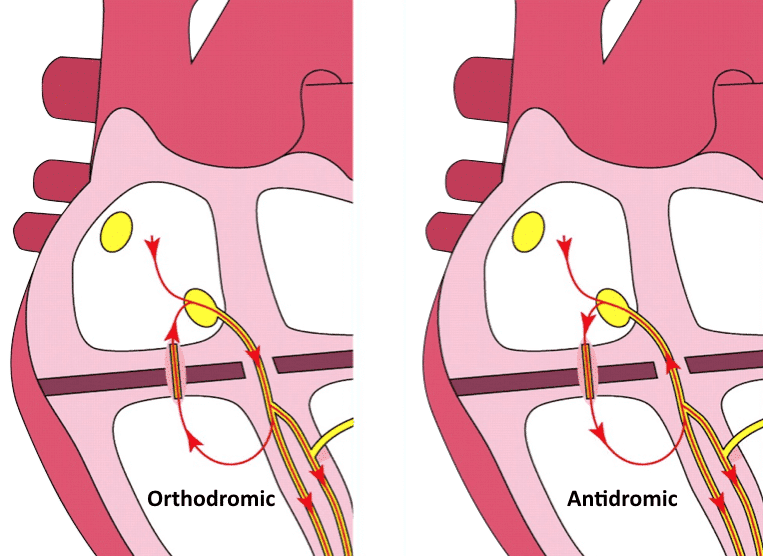
- Two types exist:
- Orthodromic AVRT which produces a regular narrow complex rhythm
- Antidromic AVRT which produces a regular wide complex tachycardia (difficult to differentiate from VT)
Orthodromic AVRT
After reverting to sinus rhythm after treatment with adenosine, the underlying WPW pattern is evident
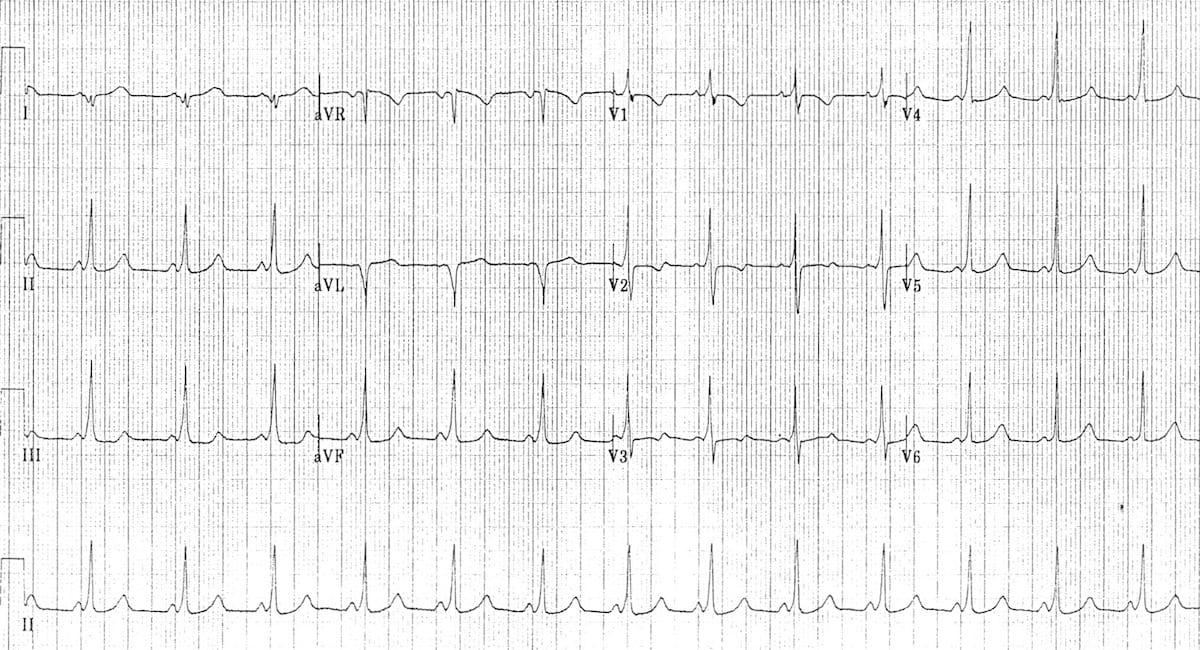
- The tall R waves in the right pre-cordial leads (V1-3) indicate a left-sided accessory pathway
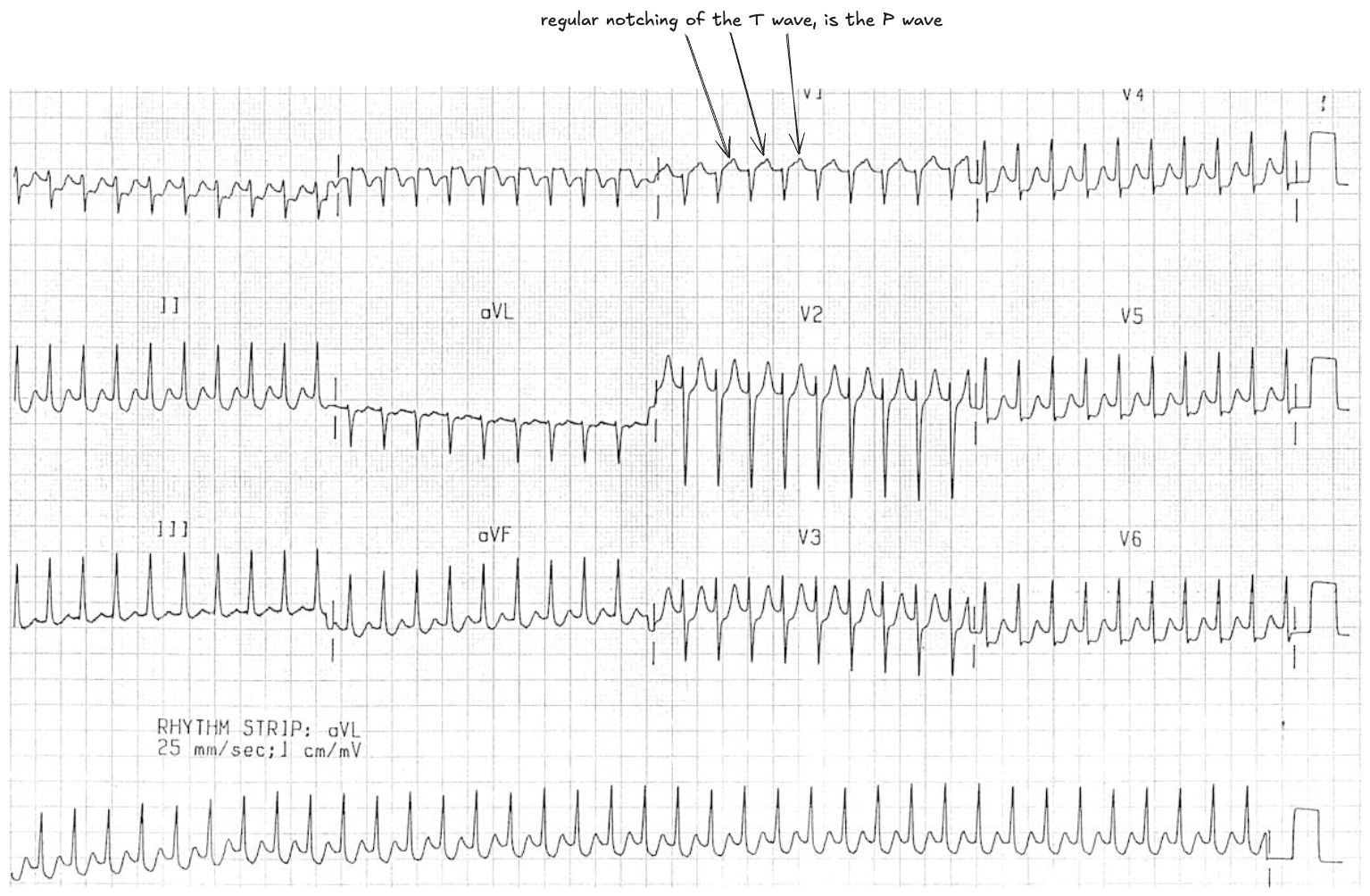
Differentiating orthodromic AVRT and AVNRT
- Typically AVNRT has retrograde P waves that occur early (typically buried in the QRS or pseudo R’ waves at the terminal portion of the QRS)
- In AVRT, retrograde P waves occur later, with a longer RP interval (typically >70 ms)
- Management however is the same between the two conditions and may reveal the underlying accessory pathway in AVRT once reverted
Antidromic AVRT
- Can be difficult to distinguish from VT and if any doubt should presume as VT
ECG Features
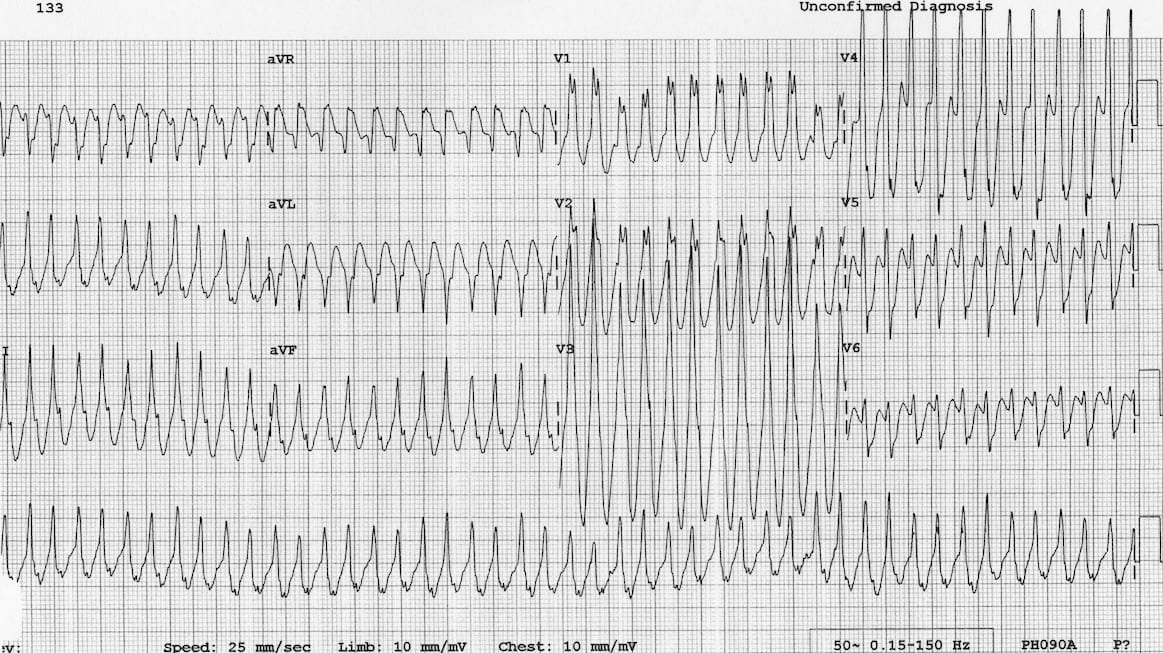
- Regular broad complex tachycardia ~280 bpm
- The patient is 5 year old by and VT is very unlikely in this demographic
- Rhythm resolved with vagal manoeuvres (despite it probably not being safe to do this)
Management
- In stable patients, target the accessory pathway with procainamide (class 1 antiarrhythmic) or second line options: ibutilide (class 3 antiarrhythmic) or amiodarone
WARNING
AV blockade with adenosine may interrupt this re-entry circuit but there is a small risk of inducing AF. If this occurs it will likely precipitate cardiac arrest due to rapid conduction via the AP