- Note that it is not the absolute BP level that dictates the need for intervention, but rather the threat to organ dysfunction
Non-life threatening asymptomatic hypertension management overview
- Recheck manual BP/different arm
- Check for end-organ damage
- PRN anti-hypertensives if any or once off dose of existing anti-hypertensives if applicable
- Amlodipine/GTN patch
Phone Call/Presentation Questions
- How high is the BP and what has it been previously?
- What was the reason for admission?
- Is the patient pregnant? ⇒ pre-eclampsia
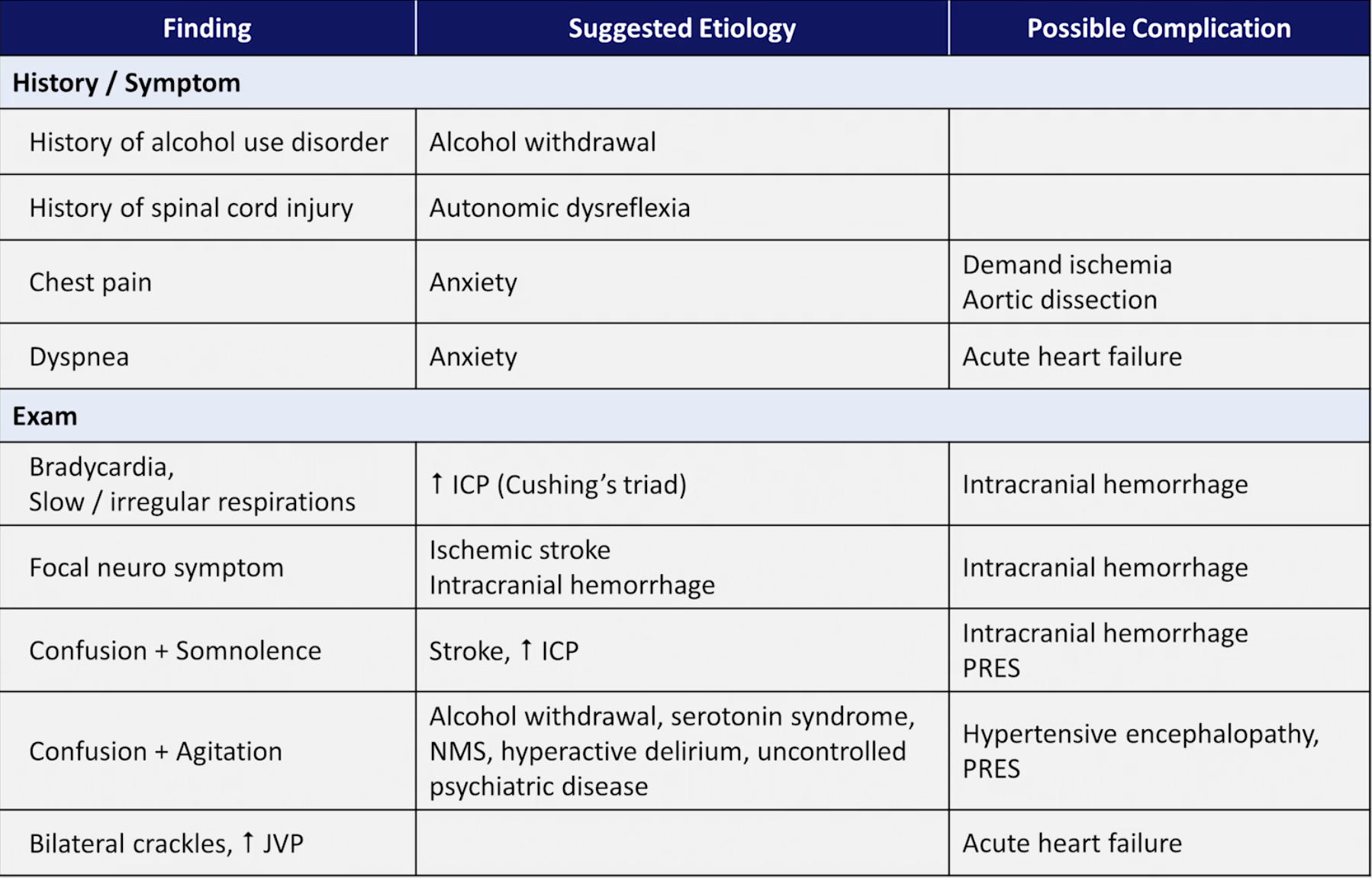
- Does the patient have symptoms suggestive of a hypertensive emergency?
- Sudden onset chest or back pain ⇒ aortic dissection
- Chest pain, arrhythmia or dyspnoea ⇒ Acute Coronary Syndromes and or Acute Pulmonary Oedema
- Sudden headache, vomiting, confusion, seizure ⇒ SAH or hypertensive encephalopathy
- What antihypertensive medication has the patient been taking?
- Is the patient taking a MAOI antidepressant
Instructions Over the Phone
- If features of hypertensive emergency or pregnant:
- Ask the nurse to stay by the patient’s bedside and get help from additional nursing staff
- Administer oxygen to maintain saturation >94%
- Attach ECG and pulse oximetry monitoring to the patient
- Request an IV trolley at the patient’s bedside with a selection of cannulae ready for insertion if not already in place
- If asymptomatic and no abnormal clinical signs, ask the nurse to check the BP again in 10 minutes and call you back with the result
- Ensure that the patient’s regular antihypertensive medication has not been missed recently
- Hypertension associated with acute end-organ damage needs to be seen immediately (hypertensive emergency)
- Hypertension in an asymptomatic patient does not need to be assessed immediately irrespective of how high the BP is; the BP can be safely brought under control over the following hours or days1
Common Causes (Corridor Thoughts)
- Essential Hypertension
- Especially outpatient anti-hypertensives being withheld
- Secondary hypertension
- Obstructive uropathy, renal artery stenosis, chronic pyelonephritis
- Glomerulonephritis, diabetic renal disease, polycystic kidney disease
- Endocrine disease such as Cushing’s syndrome, Conn’s syndrome, acromegaly, thyrotoxicosis, myxoedema
- Autoimmune disease such as SLE or scleroderma
- Medications
- Corticosteroids, oral contraceptive pill, NSAIDs
- Serotonin syndrome
- Neuroleptic malignant syndrome
- Catecholamine related
- Phaeochromacytoma
- Drug overdose (especially cocaine, amphetamines, ecstasy)
- Medication withdrawal
- Abrupt withdrawal from a beta-blocker, clonidine or ACE inhibitor resulting in a rebound hypertensive crisis
- Drug interaction
- MAOI antidepressant in combination with a sympathomimetic or other psychoatcive drug or a food containing tyramine (e.g. cheese or wine)
- Neurogenic
- Anxiety (e.g. white coat hypertension, unexpected/distressing hospital admission)
- Raised intracranial pressure (e.g. Cushing’s reflex of hypertension and bradycardia)
- Cerebral ischaemia (e.g Stroke)
- Autonomic dysreflexia (e.g. following high spinal cord injury)
- Other
- Preeclampsia
- Coarctation of the aorta
- Polycytheaemia
- Hypercalcaemia
- Hyperparathyroidism
- Sleep apnoea
- Hyperactive delirium
- Other miscellaneous that cause transient ↑ BP: pain, bladder distension, alcohol or nicotine withdrawal, agitation and anxiety
Assessment
NOTE
It is important to distinguish hypertension as the complication of a suspected disease from the aetiologies of hypertension and importantly not mutually exclusive
End of Bed
- The initial appearance often undermines the situation; even a patient with hypertensive encephalopathy may look deceptively well
A → E Assessment
- Blood pressure?
- Retake the blood pressure in both arms (lower pressure in one arm can indicate aortic coarctation)
- Heart rate?
- Bradycardia and hypertension in a patient not on beta-blockers ⇒ ? ↑ICP
- Tachycardia and hypertension ⇒ catecholamine related cause
- Respiratory rate?
- Dyspnoea may indicate pulmonary oedema with acute LVF → listen at lung bases for confirmatory basal crackles
Immediate Management
- If acutely symptomatic or suggestive of a serious cause:
- Call for senior help
- Oxygen to maintain the saturation >94%
- Attach cardiac monitoring and pulse oximeter to the patient
- Establish IV access
- Acute lowering of the BP may be required but only when critical hypertensive emergency is diagnosed
- The choice of antihypertensive agent otherwise depends on cause of the hypertension, age and medical history
Selective History and Chart Review
- Signs of end-organ damage indicating a hypertensive emergency?
- Sudden onset tearing chest or back pain ⇒ Aortic Dissection
- Focal weakness or sensory symptoms ⇒ Aortic Dissection
- Shortness of breath, orthopnoea ⇒ Acute Pulmonary Oedema
- Chest pain ⇒ myocardial ischaemia
- Sudden headache, confusion ⇒ Subarachnoid haemorrhage
- Headache, nausea and vomiting, confusion, blurred vision ⇒ Hypertensive encephalopathy
- Does the patient have a history of hypertension or any risk factors for hypertension?
- Ask specifically about previously diagnosed renal, autoimmune or endocrine disease, amphetamine or cocaine use, steroid therapy or progressive uraemia (renal hypertension)
- Was the patient taking antihypertensive medications prior to coming to hospital?
- Prescribed antihypertensive agents
- Also consider over-the-counter remedies containing ephedrine, liquorice, St John’s wort
- Check medication chart to ensure the patient’s normal antihypertensive medications have been charted
- Discontinuation of an antihypertensive medication often happens at admission → look back in the chart or for a GP’s letter
- Prescribed antihypertensive agents
- Charts
- Observation chart
- Check previous BP measurements and confirm that is abnormally high for the patient (check modifications)
- Decide whether there has been a sudden or slow change
- Check the HR (is the hypertension associated with tachycardia or bradycardia)
- Medication chart
- Check for prescribed agents that cause hypertension:
- Corticosteroid
- Amphetamine derivative (usually prescribed for appetite suppression or narcolepsy)
- NSAIDs
- Nasal decongestants (e.g. pseudoephidrine within 14 days of a MAOI)
- Oral contraceptive pill
- MAOI
- Check for prescribed agents that cause hypertension:
- Observation chart
Examinations
| Examination | Notes |
|---|---|
| Vitals | Repeat now and check BP in both arms |
| Mental | Agitation, confusion ⇒ ↑ ICP, SAH, hypertensive encephalopathy |
| Fundoscopy | Assess fundi for hypertensive changes (arteriolar narrowing, flame shaped haemorrhages near the disc, exudates and ischaemic changes ‘cotton wool spots’) |
| Papilloedema is a bad sign as it indicates hypertensive encephalopathy with cerebral oedema | |
| Severe hypertension may not show marked encephalopathy or papilloedema but will usually show retinal haemorrhages or exudates | |
| Resp | Tachypnoea, crackles, pleural effusion ⇒ APO |
| Cardiovascular | S3 gallop, elevated JVP ⇒ LVF and biventricular Acute Heart Failure |
| Absent pulse, new murmur ⇒ Aortic Dissection | |
| Neuro | Hyperreflexia, clonus, headache and visual disturbances ⇒ pre-eclampsia, hypertensive encephalopathy |
| Focal neurological defecits ⇒ Aortic Dissection, late sign of hypertensive encephalopathy |
Investigations
- Bedside
- ECG
- Urinalysis - Urinary beta-hCG in women of childbearing age (pre-eclampsia) - Proteinuria (pre-eclampsia, nephrotic syndrome, glomerulonephritis) - Haematuria (renal hypertension, glomerulonephritis, nephritic syndrome)
- Bloods
- FBC (polycythaemia, anaemia with chronic renal disease)
- U&E to determine renal function (cause or effect of hypertension)
- LFTs including urate (pre-eclampsia)
- Imaging
- CXR may show
- Cardiomegaly
- Evidence of heart failure
- Widened mediastinum
- CXR may show
Specific Management
NOTE
- Overly aggressive treatment may cause syncope, cortical blindness with occipital stroke, myocardial ischaemia. Do not treat the BP reading, only treat the complication(s) associated with it
- Typically reduce by 10-20% within first hour and another 5-15% within the next day
- Severe hypertension (SBP>180 mmHg) is common in hospitalised patients and usually has no features of a hypertensive emergency and a high reading alone does not require urgent treatment
- Isolated hypertension
- Exclude end-organ dysfunction: history, examination, urinalysis, ECG, renal function
- Identify precipitating cause:
- Non-compliance, incorrect dose, drug interaction
- Secondary cause (as outlined earlier)
- Gain control gradually over 48 hours or more using oral antihypertensive medications:
- Review the patient’s current antihypertensive treatment and consider in dose or one-off dose making a clear note in the patient’s chart
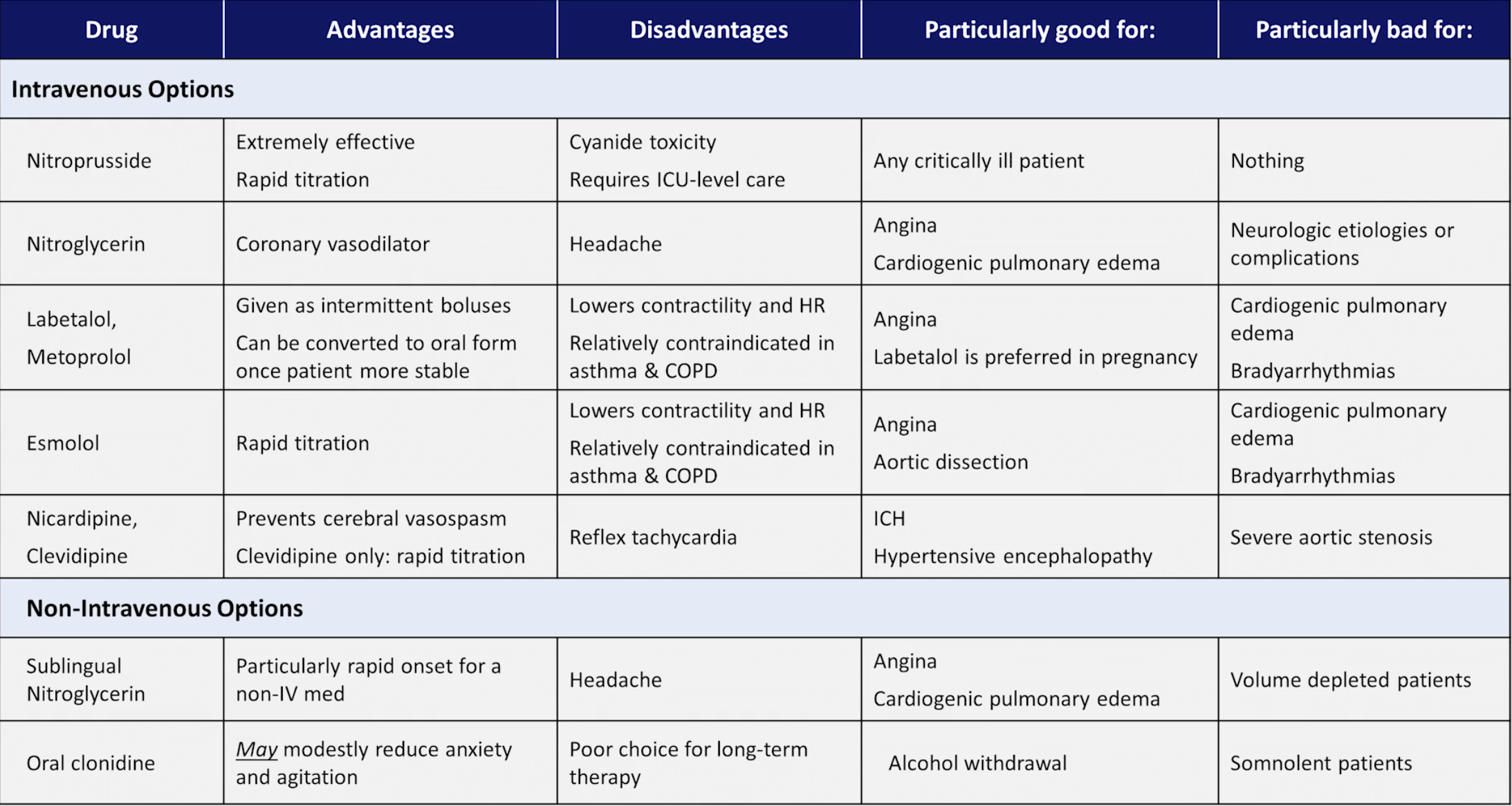
- A decision to use a new agent can usually await the patient’s regular medical care team (i.e. don’t change much on an overnight/on call shift) but can consider among: beta-blockers, diuretics, ACE inhibitors, ARBs, and CCBs
- Amlodipine 5mg or GTN patch 5mcg or 10mcg instructing nursing staff to check BP every 30 minutes and remove patch when SBP <100
- Can also consider Hydralazine 12.5mg PRN for hypertension if already on amlodipine
- Aortic Dissection Management
Hypertensive Encephalopathy
- Arrange an urgent CT brain scan to exclude alternative causes of confusion (e.g. SAH, space-occupying lesion, intracranial infection or stroke) and consider postictal state or non-convulsive status epilepticus
- Look for evidence of renal disease
- Check for proteinuria on urinalysis and send a sample for microscopy
- Look for retinal haemorrhages, exudates or papilloedema on fundoscopy
- If present, the BP should be carefully lowered over the next 2-4 hours; call for senior help
- Aim to initally reduce the MAP by 25% or for a DBP of 100-110 mmHg within the first 24 hours
- Start oral therapy:
- Atenolol 50mg, labetalol 100mg, amlodipine 5-10mg or felodipine sustained-release 5-10mg
- If unsuccessful, give hydralazine 5-10mg slow IV boluses every 15-30 minutes
- If still unsuccessful, arrange for admission to the ICU
- In ICU start sodium nitroprusside 0.25-10 mcg/kg/min IV with intra-arterial BP monitoring
- Start oral therapy:
- Once controlled, the usual medical team can continue oral therapy to maintain satisfactory BP control
Catecholamine Crisis
- Consider other presentations with sudden hypertension, headache, diaphoresis, anxiety, palpitations, nausea or abdominal pain which are more likely than phaeochromocytoma:
- Cocaine, ecstasy and amphetamine misuse
- In cocaine-induced hypertension, use high-dose titrated benzodiazepines such as diazepam 0.1-0.2mg/kg or midazolam 0.1mg/kg IV
- Check ECG and measure troponin to exclude myocardial damage
- In cocaine-induced hypertension, use high-dose titrated benzodiazepines such as diazepam 0.1-0.2mg/kg or midazolam 0.1mg/kg IV
- Abrupt antihypertensive medication withdrawal (clonidine)
- Interaction between MAOI and tyramine-containing foods (e.g. cheese or wine) and/or sympthaomimetic or other psychoactive drugs
- Call senior and transfer to ICU/CCU
- Phentolamine or nitroprusside may be used by beta-blockers should be avoided because of the risk of unopposed alpha stimulation causing increased BP
- Cocaine, ecstasy and amphetamine misuse
- If phaeochromocytoma suspected, call your senior and transfer the patient to the ICU/CCU for ECG and intra-arterial BP monitoring followed by alpha-adrenergic blockade
Pre-eclampsia and Eclampsia
- The treatment of choice near term is immediate delivery of the baby and magnesium sulfate IV. Call for senior help including the obstetric team, and commence magnesium for any complications:
- Give magnesium sulfate 4 g IV over 10–15 minutes, followed by maintenance infusion 1 g/hour continued for at least 24 hours after delivery.
- Magnesium sulfate does not significantly lower the BP. Therefore, other drugs such as hydralazine or labetalol are given according to local practice.
- Diuretics are avoided as the patient is already volume-depleted from an activated renin–angiotensin system, despite being hypertensive.
Sources
- FRCEM AFTBAFFF, FFSEM MCMMbcF, FACEM ACMMc. Marshall & Ruedy’s On Call: Principles & Protocols. 3rd edition. Elsevier; 2016. Chapter 19 Hypertension
- Acute Hypertension - Strong Medicine | Youtube
Footnotes
Footnotes
-
According to On Call ↩