Risk factors
- Increased risk of ACS with central obesity, autoimmune conditions, chronic renal disease, diabetes and HIV
Symptoms
- Pain or tightness in chest, jaw, neck, left arm, right arm or epigastrium associated with symptoms of dyspnoea, diaphoresis or fatigue
- Atypical symptoms of myocardial ischaemia occur in women, people with diabetes and the elderly
Classification
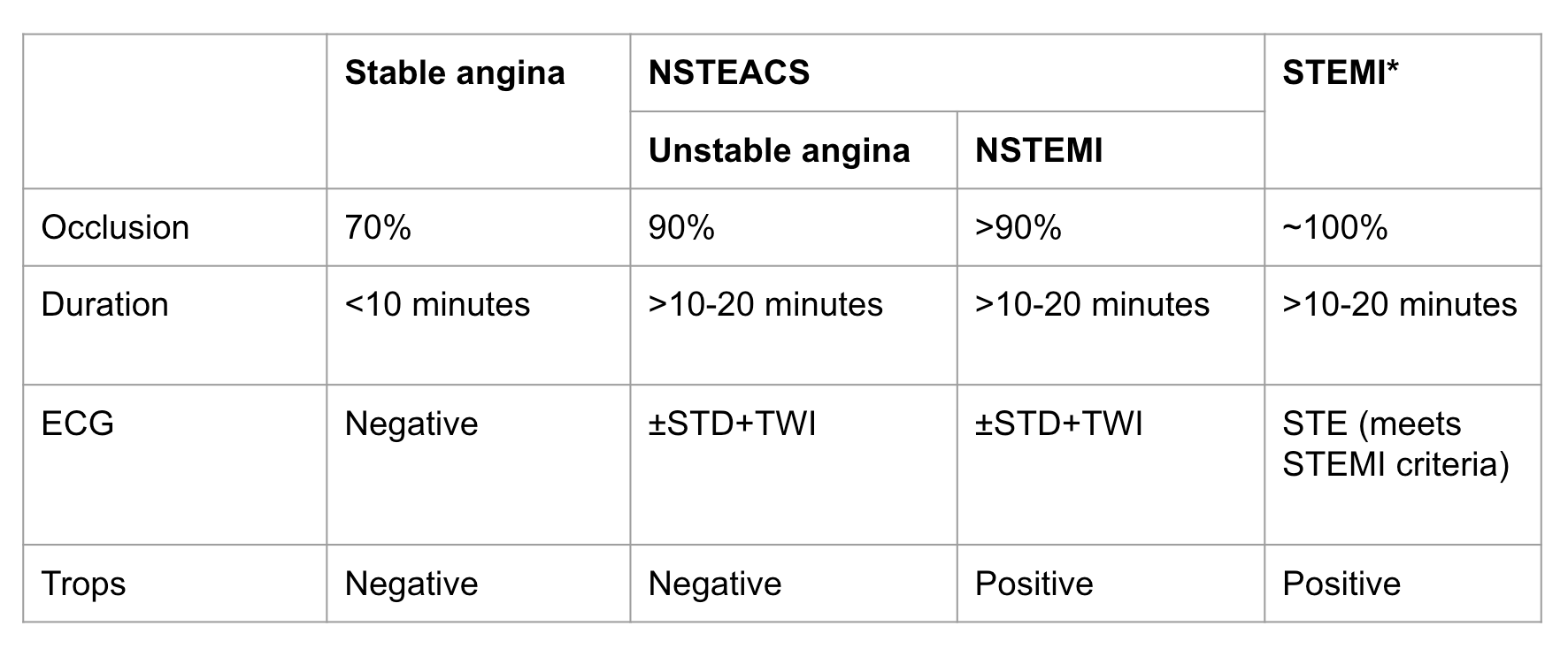
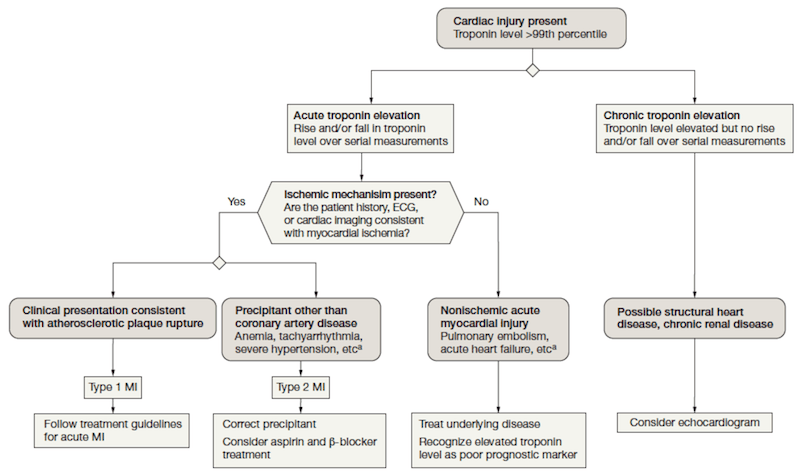
- Other classification
- Type 1 spontaneous myocardial infarction = atherothrombotic coronary occlusion compromises myocardial blood flow (i.e. heart attack due to coronary plaque rupture)
- Type 2 myocardial infarction = secondary to ischaemic imbalance between myocardial oxygen suply and/or demand. Can happen due to coronary artery spasm, tachyarrhythmias, bradyarrhythmias, anaemia etc
- Troponins
- For high sensitivity troponins, considered positive if1:
- Increase of ≥20% if first Tn elevated, or
- Increase of ≥50% in patients with small initial Tn elevations
- Can consider a third troponin
- For high sensitivity troponins, considered positive if1:
Clinical Features
- Some groups of people (females, diabetics, CKD and the elderly) are more likely to present with atypical or less-specific symptoms such as breathlessness and the pain is absent
Unstable Angina
- Defined by ≥1 of:
- Angina on exertion, occurring with increasing frequency over a few days, provoked by progressively less exertion (also known as crescendo angina)
- Episodes of angina like pain occurring recurrently and unpredictably, without specific provocation by exercise. These episodes may be relatively short-lived (e.g. a few minutes) and may settle spontaneously or be relieved temporarily by sublingual glyceryl trinitrate, before recurring
- An unprovoked and prolonged episode of chest pain, raising suspicion of AMI, but, without definite ECG changes or laboratory evidence of AMI
- In unstable angina the ECG may be:
- Be normal
- Show evidence of acute myocardial ischaemia (usually ST segment depression)
- Show non-specific abnormalities (e.g. T-wave inversion)
- In unstable angina, by definition, troponins are negative
STEMI
ECG STEMI Criteria
- Ongoing chest pain and any of the following:
- ST elevation of 1mm or more in 2 or more adjacent leads except V2 and V3 which require ST elevation of:
- 2.5mm or more in men under 40 years
- 2.0mm or more in men aged 40 years or over
- 1.5mm or more in women
- Left bundle branch block and haemodynamically unstable
- Left bundle branch block and haemodynamically stable with positive modified Sgarbossa criteria
- Posterior infarct (ST depression V1-V3); needs a posterior ECG to confirm
- de Winter T waves V2-V5
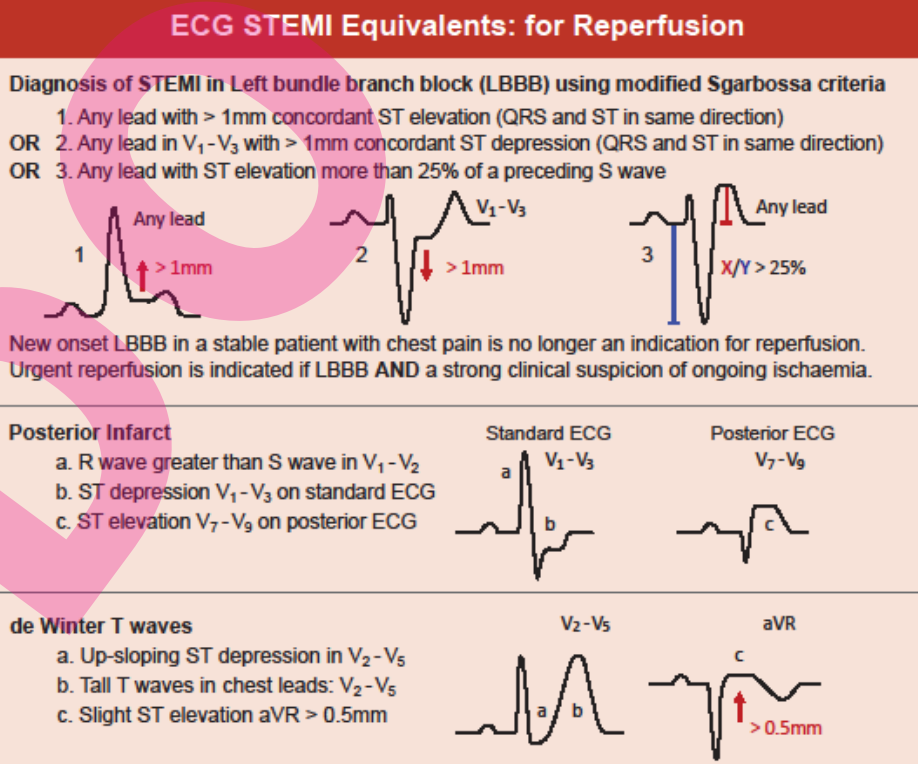
- ST elevation of 1mm or more in 2 or more adjacent leads except V2 and V3 which require ST elevation of:
As from: PASCA ACS Flowchart and PASCA STEMI Flowchart
Other STEMI
- In patients with inferior STEMI, RV infarction is suggested by:
- ST elevation in V1
- ST elevation in V1 and ST depression in V2 (highly specific for RV infarction)
- Isoelectric ST segment in V1 with marked ST depression in V2
- ST elevation in III > II
- Diagnosis is confirmed by the presence of ST elevation in the right-sided leads (V3R-V6R)
Acute Management
- Determine if alternate cause of ST elevation (i.e. type 2 MI) and manage that cause accordingly
- Call senior doctor and obtain an urgent cardiology consult
- Move to resuscitation bay and apply defibrillator pads
- Indications for reperfusion therapy for STEMI:
- Presented to hospital within 12 hours of chest pain/AMI symptoms
- Or if >12 hours since symptom onset any of:
- Ongoing ischaemia (e.g. persistent pain and dynamic ECG changes)
- Viable myocardiam (preservation of R waves in infarct-related ECG leads)
- Major complications (e.g. cardiogenic shock, heart failure, malignant arrhthymias)
- Consider advanced care directive and other factors affecting the patient’s overall survival (e.g. advanced age, frailty)
- PCI available in <60 minutes2:
- Request urgent transfer for PCI
- Anticoagulation before PCI:
- Aspirin 300mg if not already given as part of [[Chest Pain#Assessment#Initial Assessment (if not done on the phone)|chest pain initial assessment & management]]
- Heparin 5000 units IV
- Ticagrelor 180mg PO or Prasugrel 60mg PO preferred otherwise alternatively
- Clopidogrel 300-600mg PO
- Note that ticagrelor is contraindicated in 2nd or 3rd degree AV block
- Ask cardiologist if glycoprotein IIb/IIIa inhibitor is indicated (e.g. eptifibatide, tirofiban)
- Transfer for PCI
- PCI not available:
- Check for contraindications to thrombolysis:
- Symptoms present for more than 12 hours
- BP >180/110 → treat hypertension (see Hypertension) and reassess
- Major trauma or surgery or internal bleeding within one month
- Ischaemic stroke within 3 months
- Intracerebral bleed at any time
- Allergy to tenecteplase
- Request senior review if relative contraindication to thrombolysis present:
- Ischaemic stroke >3 months
- INR >1.8
- On anticoagulation
- Bleeding disorder
- Antiplatelet before thrombolysis
- Aspirin 300mg if not already given as part of [[Chest Pain#Assessment#Initial Assessment (if not done on the phone)|chest pain initial assessment & management]]
- Clopidogrel 300mg if <74 years or 75mg if ≥75 years
- Clopidogrel is preferred for thrombolysis
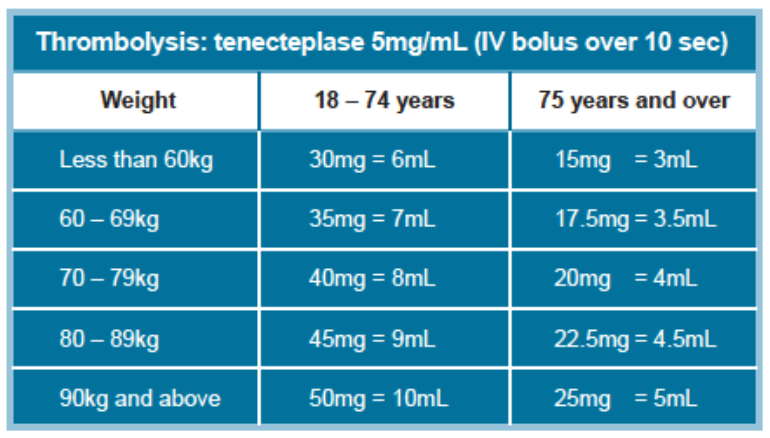
- Thrombolysis with tenecteplase, dosage based on weight
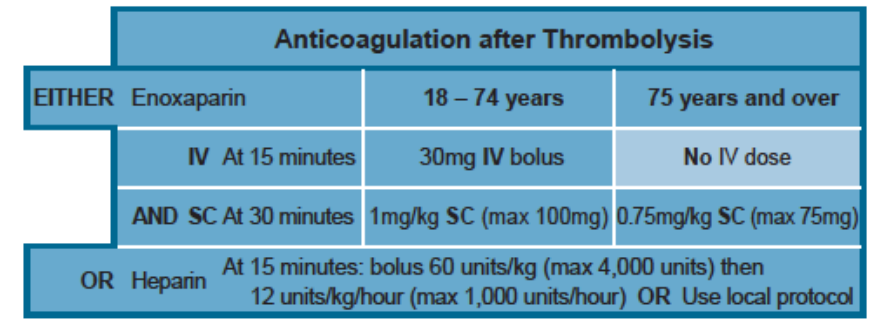
- Anticoagulation after thrombolysis
- Thrombolysis successful if all: - ECG >50% reduction in ST elevation - Symptoms largely resolved - Haemodynamically stable
- Admit or transfer for PCI depending on local protocols
- Failed thrombolysis → immediate transfer to PCI hospital for rescue PCI
- Sccuessful thrombolysis → Angiography ± PCI during same admission
- Check for contraindications to thrombolysis:
- Also organise echocardiogram
- Cardiogenic shock management
- In most cases IV fluid bolus is the mainstay of management; involve your senior early if hypotension is not fluid responsive
- Cardiogenic shock
- Clinically manifested by hypotension, elevated JVP and pulmonary oedema
- Treat ACS-related causes (see ACS)
- After giving aspirin, heparin and clopidogrel or prasugrel refer for immediate PCI
- Fibrinolytic therapy does not substantially improve the outcome in cardiogenic shock1
- Exclude other causes of hypotension with raised JVP using urgent echocardiogram
- Also perform urgent echocardiogram in patients with a new murmur as valve repair my be required
- Inferior STEMI
- Confirm RV infarction by placing right sided chest leads (usually just V4R but sometimes also with V5R and V6R)
- STE indicates RV infarction
- These patients are dependent on preload for their cardiac output so avoid dropping preload with GTN, morphine or diuretics
- Less likely to develop pulmonary oedema → try small aliquots of normal saline at 2 mL/kg
- Exclude aortic dissection causing shock from tamponade or severe aortic incompetence
- Arrange CT scan with IV contrast (CT angiography) or TOE to best distinguish Aortic Dissection from ACS
- General measures of shock
- Give maximal oxygenation, careful fluid management and consider inotrope infusions such as noradrenaline with or without dobutamine in the ICU.
- If these measures are unsuccessful, intra-aortic balloon pump, left ventricular assist device (LVAD) or circulatory bypass are required if a reversible pathological feature is present and it is available
Basic level (MONASH)
- Morphine
- Oxygen
- Nitrates
- Antiplatelets
- Save tissue
- Heparin
NSTEACS
Assessment
 As from PASCA ACS Checklist
As from PASCA ACS Checklist
Acute Management
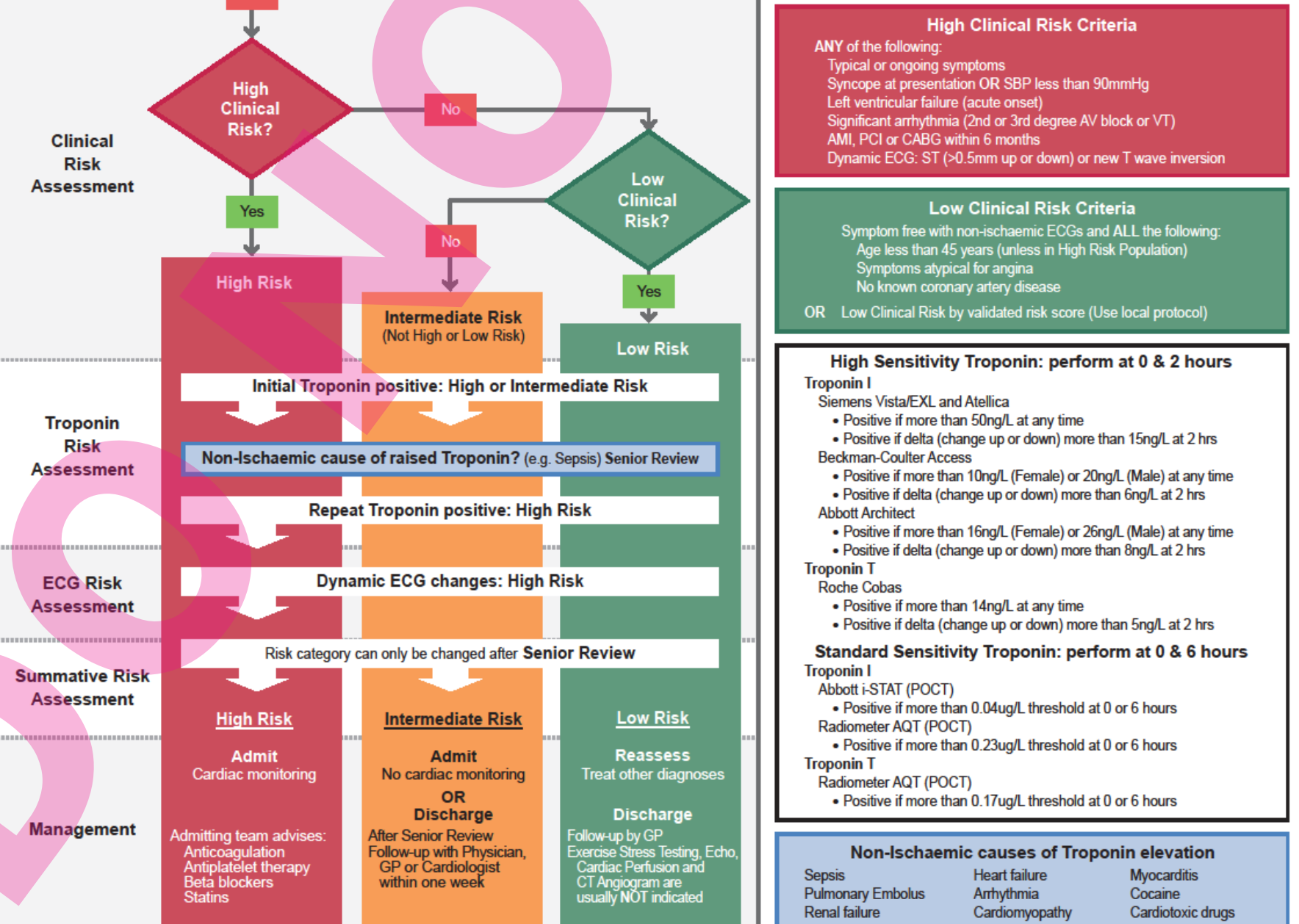
- Perform serial ECGs immediately and after 6-8 hours or every 15 minutes if the pain is continuing. Also perform ECG each time a troponin is taken
- Perform high sensitivity troponin at 0 and 2 hours
- Perform standard sensitivity troponin at 6 and 8 hours
- Aspirin 300 mg orally chewed or dissolved before swallowing if not given already
- 100-150 mg orally daily aspirin
- High clinical risk:
- Criteria: Any of the following
- Typical or ongoing symptoms
- On call makes mention of repetitive or prolonged (>10 min) ongoing chest pain or typical chest pain in patients with diabetes or chronic renal impairment (eGFR <60)
- Syncope at presentation or SBP <90mmHg
- Acute onset left ventricular failure
- Significant arrhythmia (2nd or 3rd degree AV block or VT)
- AMI, PCI or CABG in last 6 months
- Dynamic ECG: ST (>0.5mm up or down) or new T wave inversion
- Initial and repeat troponin positive with no non-ischaemic cause of troponin elevation
- Typical or ongoing symptoms
- Management
- If STEMI changes follow [[Acute Coronary Syndromes#STEMI#Management|STEMI Management as above]]
- Commence high-flow oxygen if shocked or hypoxic
- Give aspirin 300mg PO if not done so already
- Contact senior doctor immediately, then the cardiology registrar
- Give prasugrel 60mg PO (then 10mg OD), ticagrelor 180mg PO (then 90mg BD) or clopidogrel 300mg PO (then 75mg OD) as indicated by senior/reg
- Cardiology team will advise heparin anticoagulation; suitable options include
- LMWH if renal function allows
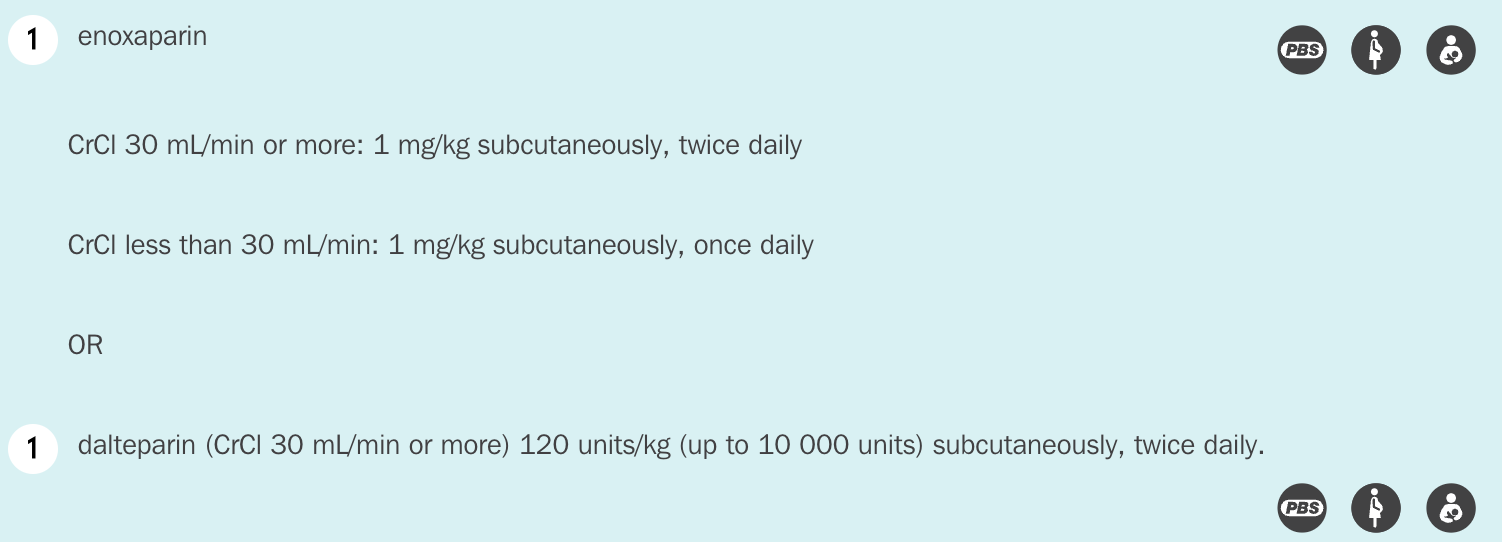
- UFH; ask senior for advice
- LMWH if renal function allows
- Cardiology will advise of use of glycoprotein IIb/IIIa inhibitors (e.g. eptifibatide or tirofiban) if immediate access to cath lab is not available
- Admit with cardiac monitoring (preferably to CCU) for consideration of angiography within next 48 hours3
- Admitting team will advise:
- Anticoagulation
- Antiplatelet therapy
- Beta blockers
- Or diltiazem if beta blockers are contraindicated
- Avoid dihydropyridine calcium channel blockers (e.g. nifedipine)
- Statins
- Criteria: Any of the following
- Intermediate risk
- Criteria: Doesn’t meet high or low risk criteria
- Management
- Give aspirin 300mg PO if not done so already
- Call senior doctor and refer to inpatient medical registrar
- Repeat ECG and troponin at 6-8 hours
- Admit without cardiac monitoring or discharge after senior review with follow up with GP/Cardiologist in one week
- Usually require exercise stress testing ideally within 72 hours to further categorise into EST-positive and EST-negative
- Low risk
- Criteria: Symptom free with non-ischaemic ECGs and ALL of the following:
- Age <45
- Symptoms atypical for angina
- no known coronary artery disease
- Management
- Treat other diagnoses
- Give aspirin 300mg PO if not done so already
- Review precipitating cause of angina (e.g. anaemia, aortic stenosis, thyrotoxicosis and HCM) and ECG
- If known diagnosis of angina
- Determine if threshold for angina has decreased or the severity of pain increased
- Consult with senior for adjustment to antianginal medication
- If episode was prolonged or worse with no easily fixable precipitant repeat troponin and ECG at 6-8 hours
- Follow up with GP or cardiology outpatient
- Exercise stress testing, echo, cardiac perfusion and CTA NOT usually indicated4
 As from: PASCA ACS Flowchart
As from: PASCA ACS Flowchart
- Criteria: Symptom free with non-ischaemic ECGs and ALL of the following:
Other Management
Recurrent Pain
- Recurrent episodes of ischaemic chest pain may require GTN infusion for a short period of time; prolonged infusion rapidly induces tolerance
- GTN 10 micrograms/minute by IV infusion increasing by 10 micrograms/minute every 3 minutes until pain is controlled provided systolic blood pressure ≥95 mmHg
Long Term Management
- Aspirin and a P2Y-12 inhibitor (DAPT)
- Statin
- Beta-blocker
- ACE-inhibitor
- Should be started within 24-48 hours of acute myocardial infarciton
- Contraindications include haemodynamic instability and hypotension
Sources
- More so from Pathway for acute coronary syndromes: https://aci.health.nsw.gov.au/networks/eci/clinical/tools/cardiology/pathway-for-acute-coronary-syndrome Published June 2021
- ACI chest pain guidelines: https://aci.health.nsw.gov.au/ecat/adult/chest-pain Published December 2023.
- eTG pages: Acute chest pain of possible cardiac origin, Acute coronary syndrome pages
- Less so from FRCEM AFTBAFFF, FFSEM MCMMbcF, FACEM ACMMc. Marshall & Ruedy’s On Call: Principles & Protocols. 3rd edition. Elsevier; 2016. 648 Chapter 16: Chest Pain p. 117
- Brown, Cadogan (2020) Emergency Medicine : Diagnosis and Management, Taylor & Francis Group.
Footnotes
-
As from https://www.aliem.com/high-sensitivity-troponin-testing/ ↩
-
eTG says if PCI is available within 120 minutes ↩
-
eTG says within 2 hours for very high risk and within 24 hours for high risk ↩
-
eTG says for patients with unstable angina considered low risk non-invasive investigations such as stress testing are usually appropriate ↩