Aetiologies
- Bronchospasm, sputum plugging, pneumothorax, viral illness, pneumonia
- Right, left or biventricular failure; arrhythmia (e.g. AF)
- ACS
- PE
- Malignancy
- Drug non-compliance, inadequate steroid, inappropriate sedation
- Environment allergens, weather change
History
- Objective: gain an idea of baseline capacity and elicit cause of exacerbation:
- Current treatment
- Inhalers, steroids, antibiotics, theophylines, nebulisers
- Home oxygen use
- Past history: previous admissions, comorbidity and previous ICU assessments/admissions
- Usual and current daily exercise capacity and level of dependence (e.g. How far can they walk without stopping? How many stairs can they climb? Do they get out of the house?)
- Elicit cause of exacerbation:
- Smoking or dust exposure
- New features of cardiac or respiratory disease
- Episodes of ischaemic or pleuritic chest pain
- Worsening peripheral oedema or orthopnoea
- Non-compliance with medication, including steroids or diuretics
- Excess sedatives or opioids
- Known cardiac disease
- Ask sputum volume and colour
- Current treatment
- Indications for hospital admission for a COPD exacerbation (COPD exacerbations can often be managed in the community without referral or admission to hospital as from eTG)
- inadequate response to ambulatory management
- inability to walk between rooms (in patients who are usually mobile)
- inability to eat or sleep because of dyspnoea
- inability to manage at home, even with home-care resources
- high-risk comorbidity-pulmonary (eg pneumonia) or nonpulmonary
- altered mental status suggestive of hypercapnia
- worsening hypoxaemia or cor pulmonale
- worsening or new-onset central cyanosis
- newly occurring arrhythmia
- development of peripheral oedema
- haemodynamic instability
- acute respiratory failure
- onset of new physical signs (eg peripheral oedema).
Examination
- Hyperexpanded, barrel-shaped chest, ↑WOB (tachypnoea, accessory muscle use and lip pursing)
- Fever, wheeze, sputum production
- Cor pulmonale - right Acute Heart Failure 2° to Pulmonary Hypertension
- Signs of hypercarbia: tremor, bounding pulses, peripheral vasodilation, drowsiness or confusion
- Check for other causes of acute Dyspnoea (e.g. Asthma Exacerbation, Acute Pulmonary Oedema, Pneumothorax, PE)
Investigations
Bedside
- Spirometry and PEFR
- Spirometry during an acute episode is inaccurate and may distress the patient
- ECG looking for:
- Large P waves (P pulmonale)
- RVH or strain, multifocal atrial tachycardia or AF
- Signs of ischaemia
- Respiratory viral swabs
- Sputum culture is not routinely recommended for COPD exacerbations as many patients with COPD are colonised with Haemophilus influenzae, Moraxella catarrhalis or Streptococcus pneumoniae
- Consider sputum culture for patients with a COPD exacerbation and ≥1 of the following:
- Severe airflow obstruction (FEV1 < 50% of predicted)
- Frequent COPD exacerbations (≥2 per year)
- Current or recent hospitalisation (within past 3 months)
- Recent isolation of or known colonisation with Pseudomonas aeruginosa within the past 3 months
- Supplemental home oxygen therapy
- Consider sputum culture for patients with a COPD exacerbation and ≥1 of the following:
Bloods
- CRP can help to determine the presence of bacterial infection in COPD exacerbations and subsequently the potential benefit of antibiotic therapy
- FBC, UEC, Glucose
- ABG (or VBG + pulse oximetry)
- Perform an ABG only if:
- Severe episode
- No response to treatment
- Any suggestion of acute or worsening retention with altered mental status
- Chronic retention is indicated by a raised from metabolic compensation; a pH <7.3 suggests acute respiratory acidosis (see ABG Interpretation)
- Perform an ABG only if:
- If pneumonia suspected and/or pyrexial: blood cultures and pneumococcal antigens
CXR
- May show features suggestive of COPD as well as complications (e.g. atelactasis, consolidation, pneumothorax, pulmonary oedema or malignancy)
Management
- Cardiac monitoring and pulse oximeter
- Oxygen therapy:
- If evidence of retention (raised or ) → Controlled oxygen therapy initially at 28% via a Venturi mask
- Otherwise → higher dose oxygen (40-60%) mask
- Consider NIV (preferably BiPAP):
- BiPAP:
- Start at 10cm IPAP/ 5cm EPAP and titrate upwards:
- To treat persistent hypercapnia, ↑ IPAP by 2cm at a time
- To treat persistent hypoxia, ↑ IPAP and EPAP by 2cm at a time.
- The maximum IPAP/EPAP is 25/15cm
- Start at 10cm IPAP/ 5cm EPAP and titrate upwards:
- CPAP:
- Commence treatment at 5-8cm
- BiPAP:
- Bronchodilator therapy:
- Hold all home bronchodilators
- pMDI with spacer option (for patients with FEV1 >30% of predicted)
- Salbutamol 100mcg per puff for up to 8 puffs at a time via a pMDI with spacer repeated as required or
- terbutaline 500 mcg per actuation, 1 or 2 actuations via DPI or (except in those taking a LAMA)
- ==ipratropium 21 mcg per actuation, up to 4 actuations (one at a time via pMDI with spacer)
- Nebuliser option
- Salbutamol 2.5 to 5mg via nebuliser to the initial three nebulisers then give 6 hourly
- ipratropium 250 to 500mcg can be used instead or if symptoms are severe can be combined
- Ipratropium has a slower onset of effect than salbutamol
- Ipratropium is contraindicated in patients taking LAMAs
- If a nebuliser is required, it should be driven by compressed air rather than oxygen to avoid hyperoxygenation
- Salbutamol 2.5 to 5mg via nebuliser to the initial three nebulisers then give 6 hourly
- Corticosteroid therapy
- Prednisolone 50mg PO or hydrocortisone 200mg IV if unable to swallow if:
- Patient has bronchospasm or
- Patient is on long-term inhaled or oral steroids
- eTG also recommends 5 day course of steroids for exacerbations that don’t respond sufficiently to inhaled bronchodilators; dosage options include:
- Prednisolone 30-50mg PO OD for 5 days
- Hydrocortisone 50mg IV 6 hourly until oral intake is tolerated
- Prednisolone 50mg PO or hydrocortisone 200mg IV if unable to swallow if:
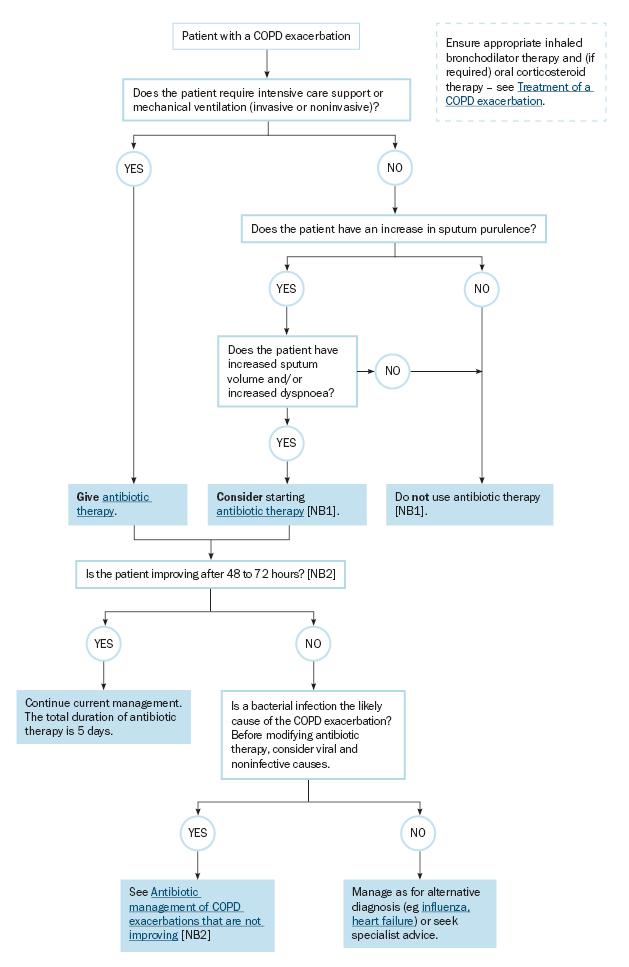
- Antibiotic therapy
- Determine if antibiotic therapy is indicated:
- A bacterial cause of the COPD exacerbation is more likely if the patient has an acute increase in dyspnoea together with both of the following clinical features:
- increased sputum volume
- sputum purulence or a change in sputum colour.
- Sputum culture is not routinely recommended for exacerbations of COPD
- A bacterial cause of the COPD exacerbation is more likely if the patient has an acute increase in dyspnoea together with both of the following clinical features:
- Treat infection with antibiotics depending on guidelines (Amoxicillin 500 mg PO 8-hourly, amoxicillin 1 g PO 12-hourly or doxycycline 200 mg PO once, then 100mg daily usually for 5 days)
- Lack of a response to initial antibiotic therapy for COPD exacerbation rarely requires switching to broader spectrum antibiotics ⇒ in mild COPD, symptoms can last for 7-10 days and in moderate-severe COPD, symptoms can persist for weeks
- Evaluate patients who are deteriorating or not improving for comon viral and non-infective causes of COPD exacerbations and consider other diagnosis such as Pneumonia, Acute Pulmonary Oedema
- For patients with severe COPD who have a COPD exacerbation that does not resposne to initial antibiotic therapy after 48-72 hours and if bacterial infection remains the likely cause consider amoxicillin + clavulanate 875+125 mg PO, 12-hourly for 5 days
- If P. aeruginosa is identified in sputum (current isolation or known colonisation in past 3 months) consider ciprofloxacin 750 mg PO 12-hourly for 5 days
- Determine if antibiotic therapy is indicated:
- If RV Acute Heart Failure with fluid overload → Furosemide 40mg IV or PO
- Consider naloxone if the patient is on opioid analgesics that may cause respiratory depression
- If no response to above and ongoing hypoxial (<85%), extreme respiratory distress, ↑ , patient is exhausted or acidaemia is worsening then commence non-invasive BiPAP ventilation
Approaching COPD and possible pneumonia
- Start on antibiotic coverage for pneumonia (e.g., ceftriaxone plus azithromycin) and check a procalcitonin.
- If procalcitonin is low (<0.5 ng/ml), this argues against typical bacterial pneumonia. Ceftriaxone can be discontinued, while azithromycin is continued to treat COPD.
- If procalcitonin is elevated, then continue combination antibiotic therapy for pneumonia (along with full-bore COPD therapy as well – the presence of PNA doesn’t exclude concomitant COPD).
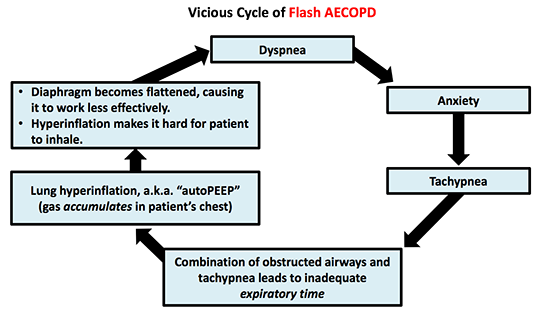
- A combination of BiPAP and anxiolytics may be very helpful in breaking patients out of a Flash AECOPD
Additional Therapies
- Extracorporeal carbon dioxide removal
- However the VENT-ACOID trial did not demonstrate significant benefit to avoid intubation or wean from mechanical ventilation although the very low intubation rate in NIV arm suggesting that the population may not have been that sick
Sources
- IBCC book: https://emcrit.org/ibcc/AECOPD/#top
- Wyatt JP, Taylor RG, Wit K de, Hotton EJ. Oxford Handbook of Emergency Medicine. Oxford: OUP Oxford; 2020. 795 p. 112
- Extracorporeal Carbon Dioxide Removal to Avoid Invasive Ventilation During Exacerbations of Chronic Obstructive Pulmonary Disease: VENT-AVOID Trial – A Randomized Clinical Trial Duggal et al. 2024; American Journal of Respiratory and Critical Care Medicine March 1, 2024 Pages xv-616