Aetiologies
- Common
- S. pneumoniae >50%
- H. influenzae especially in COPD
- Atypicals: Legionella spp., Mycoplasna, Chlamydia
- Viruses: Influenza, Chickenpox
- Less common
- S. aureus and gram negatives (esp. in alcoholics)
- Immunosuppression consider pneumocystis jiroveci
History
- Classic presentation: Dyspnoea, fever, productive cough, pleuritic chest pain and haemoptysis
- Other less classic features: Referred upper abdominal pain, diarrhoea, confusion
- Also consider features suggestive of TB: fever >5 days, night sweats, haemoptysis, weight loss, recent travel or past exposure
Exam
- Dull percussion note, bronchial breathing
- Usually only localised moist crepitations with diminished breath sounds
Investigations
Bedside
- Sputum for microscopy and culture
- Ziehl-Neelsen staining for TB
- Antigen testing and serology:
- Legionella, pneumococcal urinary antigen
- Respiratory viruses including influenza PCR
Bloods
- FBC, BSL, UEC, LFT and blood cultures (esp. if severe or hospital-acquired)
Chest X-ray
- Infiltrates (can be unilateral or bilateral or lobar or patchy)
- Parapneumonic effusion
Management
- High dose oxygen, aiming for oxygen saturation >95%
- Obtain IV access and give normal saline in patients with moderate or severe pneumonia
- These patients are often dehydrated or have hypovolaemia from sepsis
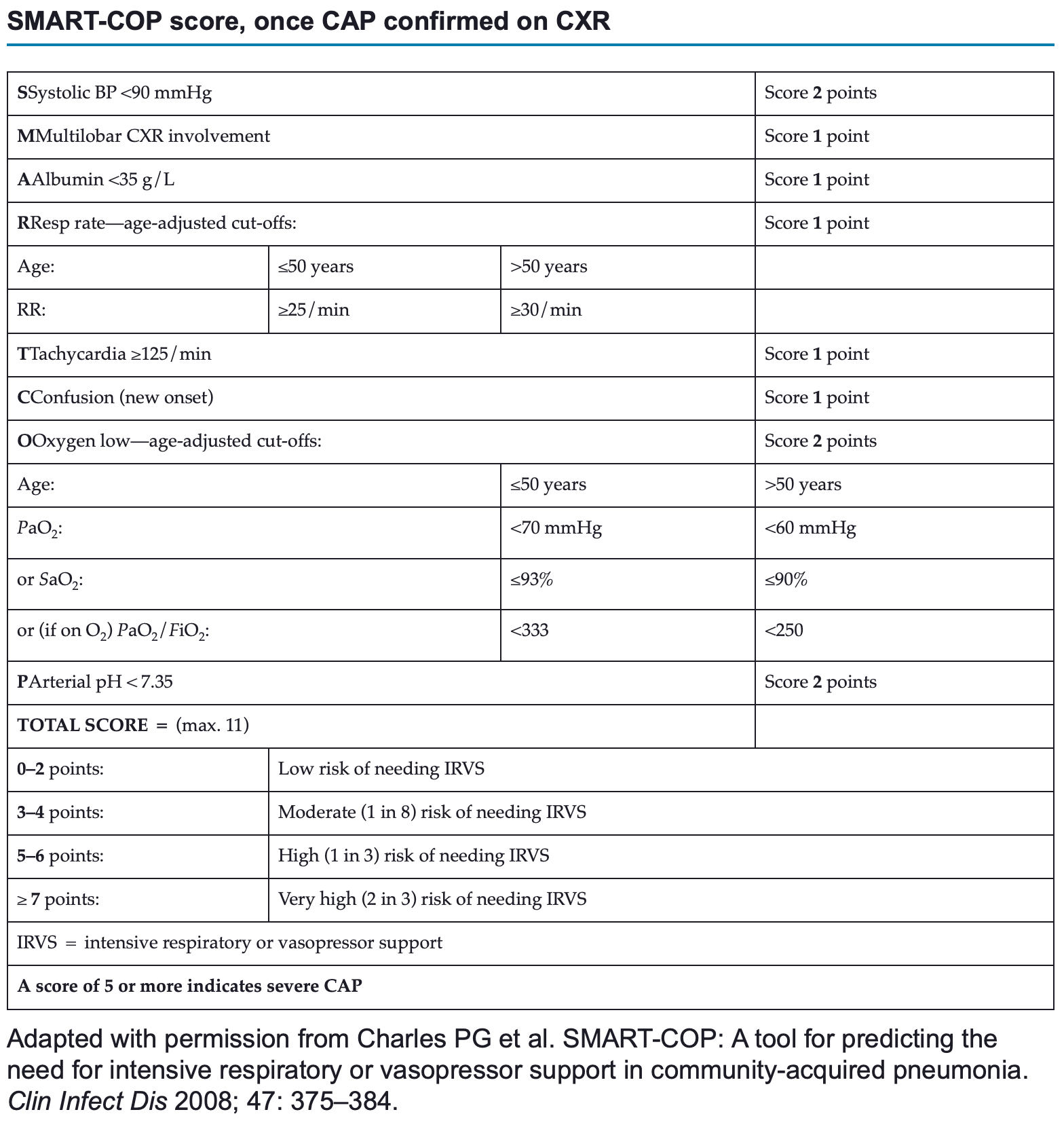
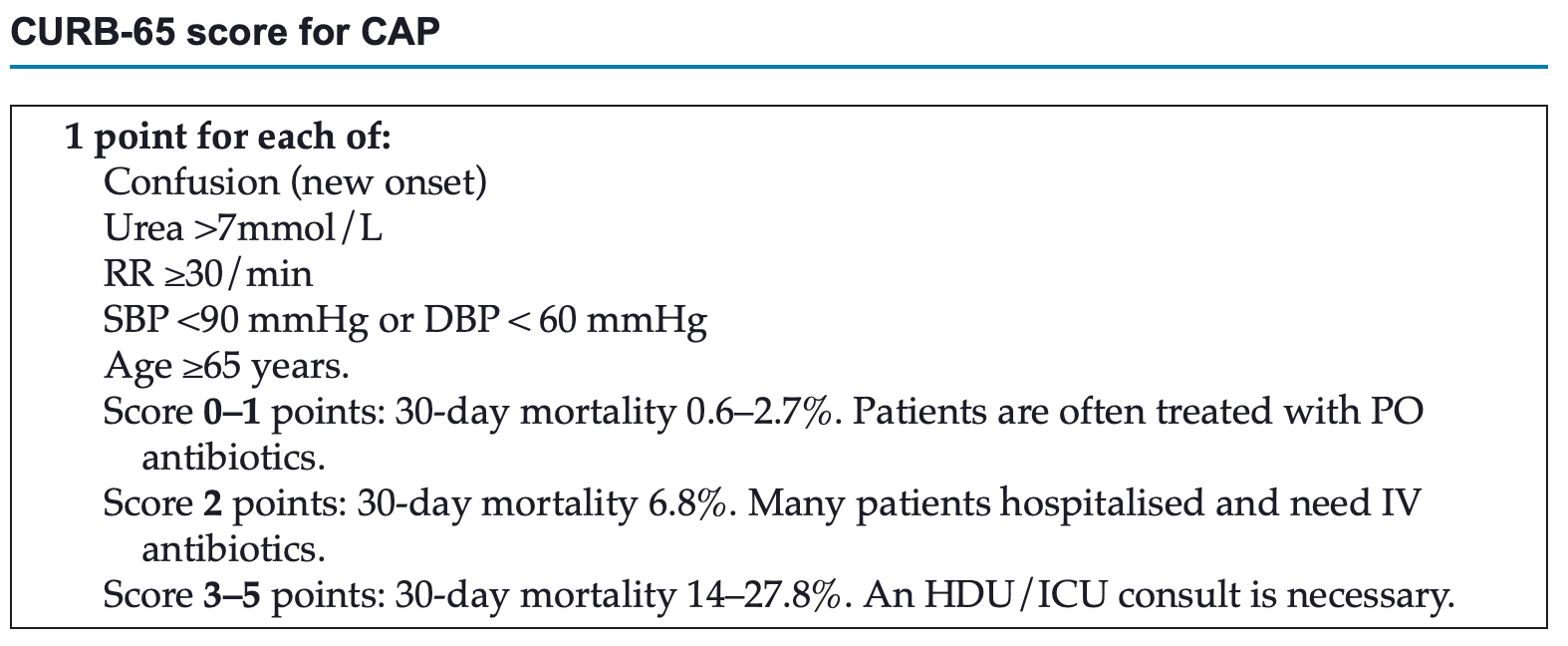
- Determine severity CAP using SMART-COP score, using CURB-65 or Pneumonia Severity Index (PSI)
- SMART-COP: ≥5 indicates severe disease requiring hospital admission, empirical IV antibiotics and referral to intensive care
 Also see: https://litfl.com/wp-content/uploads/2019/09/etg-smartcop.pdf
Also see: https://litfl.com/wp-content/uploads/2019/09/etg-smartcop.pdf
Antibiotic Therapy
CAP
- Mild CAP:
- Amoxicillin 1g PO 8 hourly for 5-7 days
- If Mycoplasma pneumoniae, Chlamydophila pneumoniae or Legionella suspected give doxycycline 100mg PO 12 hourly for 5-7 days instead
- Also add doxycycline if failing to improve by 48 hours
- If hypersensitivity to pencillin give doxycycline or moxifloxacin 400 mg PO daily
- Moderate CAP:
- Benzylpenicillin 1.2g IV 6-hourly until imrpovement then change to amoxicillin 1g PO 8 hourly for 7 days + (doxycycline 100 mg PO 12-hourly for 7 days or Clarithromycin 500 mg PO 12 hourly for 7 days (if pregnant))
- Add gentamicin 5mg/kg IV daily (if renal function normal) or change the benzylpenicillin to ceftriaxone 1g daily IV if Gram-negative bacili are identified in blood or sputum
- Consider oseltamivir 75mg BD PO in the influenza season
- Severe CAP (SMART-COP ≥5 or CURB-65 ≥3)
- Refer to HDU/ICU
- Give ceftriaxone 1g IV daily + azithromycin 500 mg IV daily
- If renal impairment or pencillin allergy give moxifloxacin 400 mg IV daily
HAP (develops ≥48 hours in hospital)
- Consult with microbiology or infectious disease
- Amoxicilling-clavulanic acid in mild pneumonia
- Ticarcillin-clavulanic acid, ceftriaxone or piperacillin-tazobactam in moderate or severe pneumonia.
- Add vancomycin if high prevalence of MRSA and consider ciprofloxacin plus azithromycin if Legionella suspected
Aspiration pneumonia
- Consider in patients with ↓LOC or ↓cough reflex (e.g ETOH, stroke, seizure, postsurgery)
- Minor aspiration doers not require antibiotics; only reat aspiration pneumonia
- Manage aspiration pneumonia as community- (<48 hours) or hospital-acquired (>48 hours) pneumonia initially depending on their length of stay in hospital
- Review patient next day and consider stopping antibiotics if improving and aspiration pneumonitis likely
| Aspiration pneumonitis | Aspiration pneumonia |
|---|---|
| Acute chemical injury to the lung parenchyma after aspiration of acidic stomach contents. Also known as chemical pneumonitis or Mendelson syndrome. Symptom onset is rapid (usually within hours of aspiration). This is the key difference between aspiration pneumonitis and aspiration pneumonia. Clinical features can be difficult to distinguish from aspiration pneumonia and the chest X-ray can appear similar to pneumonia. Severity ranges from mild symptoms such as cough or wheeze to severe acute respiratory distress syndrome (ARDS). In most patients, symptoms improve quickly (usually within 24 to 48 hours). | A bacterial infection caused by aspiration of organisms from the oropharynx. It can also follow aspiration pneumonitis, particularly in patients taking gastric acid suppression therapy or with bowel obstruction. Symptom onset is delayed; this differentiates aspiration pneumonia from aspiration pneumonitis. Clinical features suggestive of pneumonia include tachypnoea at rest, tachycardia, persistent fever, rigors, hypoxaemia or crepitations (crackles) on auscultation that do not clear with coughing. |
| Closely monitor the patient for deterioration. If unable to differentiate between aspiration pneumonitis and aspiration pneumonia, start antibiotic therapy and review within 24 to 48 hours (see Initial management of aspiration pneumonia). Consider stopping antibiotic therapy if the patient has significantly improved and aspiration pneumonitis is a more likely diagnosis. | Antibiotic therapy required see above |