Quick Links
- External
- Internal
Phone Call/Presentation Questions
- Pain (SOCRATES):
- Characteristic?
- Does it change with breathing?
- Where is the pain maximal? Radiation?
- How severe is the pain?
- Vital signs?
- Reason for admission?
- Does the patient have a history of ischaemic heart disease?
- If yes, is it similar to their usual angina or previous MI?
Instructions over the phone
- If you suspect AMI or angina (heavy, crushing, tight pain radiating to jaw or left or right arm):
- Ask the nurse to stay by the patient’s bedside and call for additional nursing staff if necessary
- Give oxygen if hypoxic or shocked maintaining a saturation of >94% after attaching monitoring (pulse oximetry and cardiac monitoring)
- Urgent 12-lead ECG
- Aspirin 150-300 mg PO unless contraindicated by hypersensitivity
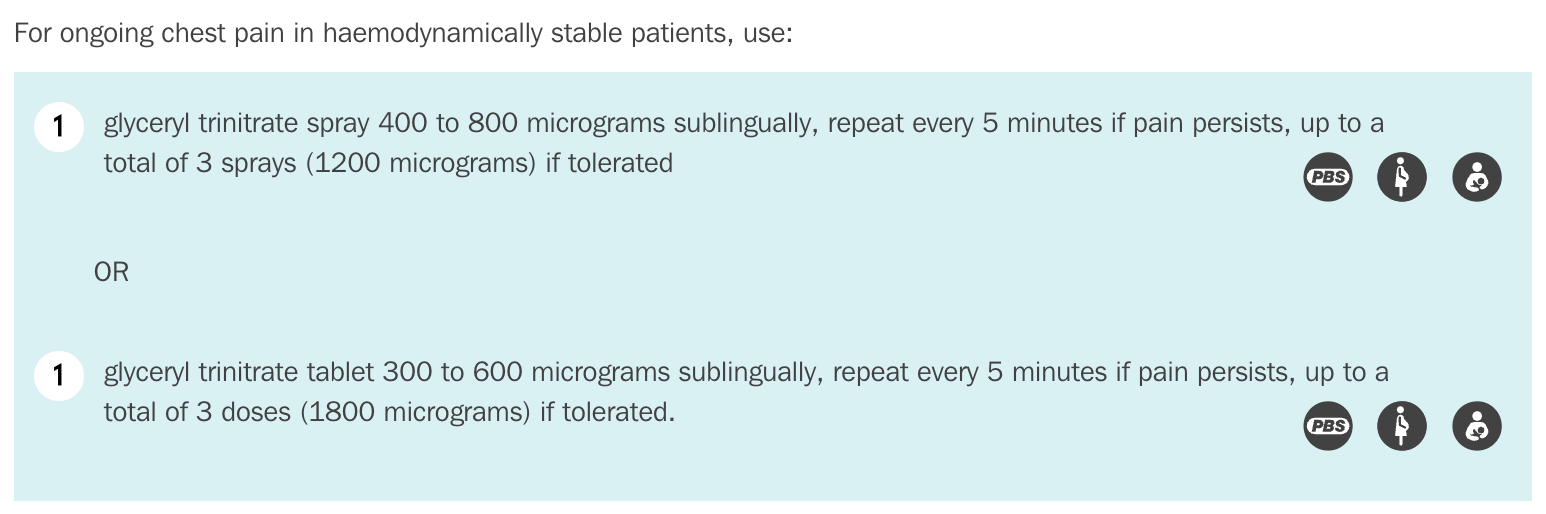
- Administer GTN SL (0.6 mg tablets or 0.4mg spray) and repeat every 5-10 minutes if pain persists and SBP remains >90mmHg
- Request and IV trolley for the patient’s bedside with a range of cannulae ready for insertion
- Attend any patient with chest pain immediately
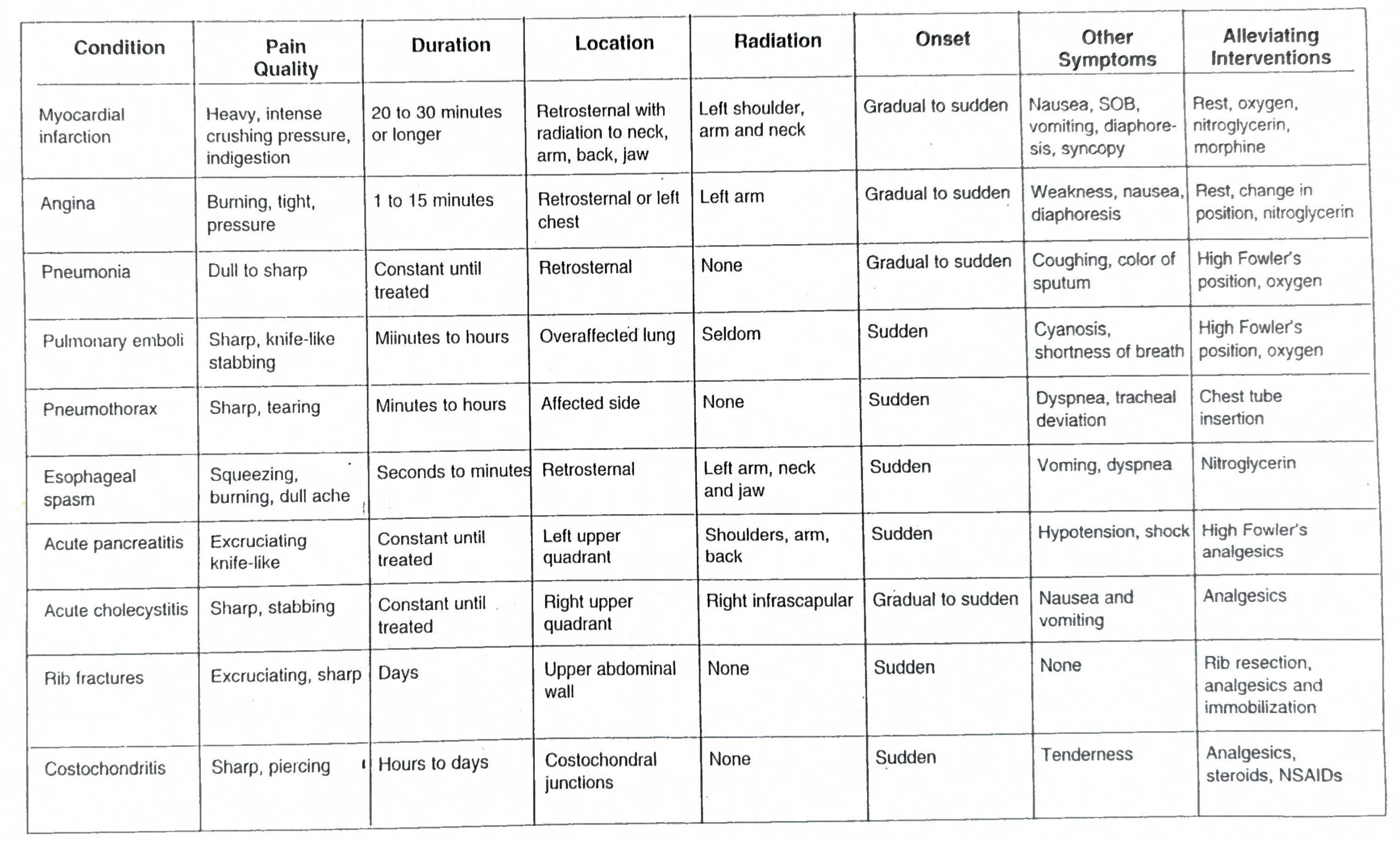
Common Causes (Corridor Thoughts)
- Cardiac
- ACS
- Acute aortic dissection
- Pericarditis
- Arrhythmias
- Hypertensive emergency
- Respiratory
- Gastrointestinal
- Oesophagitis, Oesophagel spasm
- Ruptured oesophagus (inc. Boerhaave’s syndrome)
- Hiatus hernia
- Peptic ulcer disease
- Biliary colic/cholecystitis
- Musculoskeletal
- Costochondritis
- Fractured rib
- Referred pain from spinal disease
- Herpes zoster or postherpetic neuralgia
- Psychiatric
- Anxiety and panic disorders
The main ones to rule out are ACS (and its complications), acute aortic dissection, PE
Assessment
Initial Assessment (if not done on the phone)
- Aspirin 300 mg soluble
- IV access, bloods (including troponin), cardiac monitoring, CXR and analgesia
- ECG at 0 and 2 hours, when repeating troponin and every 30 minutes if ongoing symptoms (ECG shold be done within first 10 minutes during the initial assessment)
- If meets STEMI criteria (will need senior input and compare to previous ECGs) see STEMI Management
- Ongoing chest pain and any of the following:
- ST elevation of 1mm or more in 2 or more adjacent leads except V2 and V3 which require ST elevation of:
- 2.5mm or more in men under 40 years
- 2.0mm or more in men aged 40 years or over
- 1.5mm or more in women
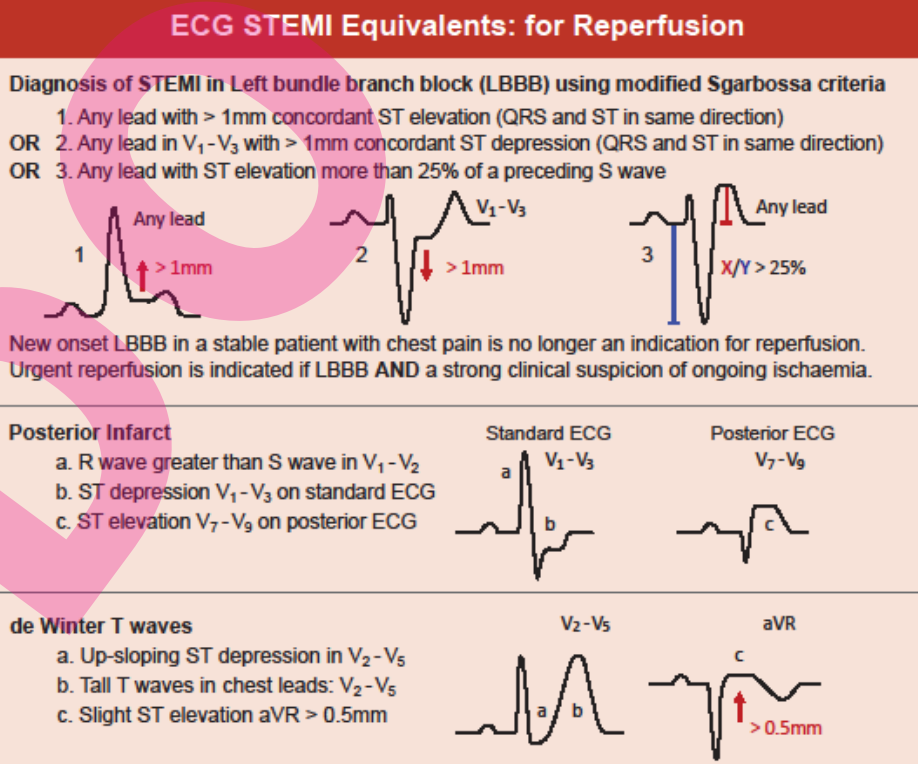
- Left bundle branch block and haemodynamically unstable
- Left bundle branch block and haemodynamically stable with positive modified Sgarbossa criteria
- Posterior infarct (ST depression V1-V3); needs a posterior ECG to confirm
- de Winter T waves V2-V5
- ST elevation of 1mm or more in 2 or more adjacent leads except V2 and V3 which require ST elevation of:
- Ongoing chest pain and any of the following:
- If meets STEMI criteria (will need senior input and compare to previous ECGs) see STEMI Management
- GTN: caution if SBP<100mmHg and in right sided and inferior infarcts
- if <93% otherwise not required in stable patients
End of Bed
- Patients with chest pain from ACS may look anxious and pale, or are shocked, breathless and clearly unwell
- Patients with aortic dissection have severe pain and are restless and agitated
- Patients with PE, pericarditis or pneumothorax are dyspnoeic and breathe with shallow, painful respirations (pleuritic pain)
- However, even if patients look well and appear comfortable at rest, they may still have a life-threatening underlying cause such as ACS, aortic dissection or PE
A → E Assessment
Prioritise assessing C in stable patients; see immediate management below
- C
- Blood pressure?
- Most patients have normal BP
- Take BP in both arms if the pain is suspicious of aortic dissection (sudden onset, sharp, tearing or migratory)
- Acute aortic dissection (AAD) suggested by a difference of >15mmHg
- Hypotension occurs in ACS, massive PE and AAD with cardiac tamponade
- Hypertension with ACS or aortic dissection should be treated urgently in resuscitation area (see: Hypertension)
- Heart rate?
- If HR >150 or <40 obtain 12 lead ECG and/or rhythym strip to diagnose the arrhythymia
- Consider AF or VT in HR>140 and therefore consider urgent cardioversion especially if associated with chest pain or hypotension
- Immediate treatment of bradycardia is not required unless the patient is hypotensive or syncopal and/or the rate is extremely slow (<40)
- If HR >150 or <40 obtain 12 lead ECG and/or rhythym strip to diagnose the arrhythymia
- ECG?
- Compare with old tracing if possible
- ST elevation or depression, T wave changes and presence of new Q waves suggest myocardial ischaemia from ACS
- Only 50% of patients with ACS will have a diagnostic ECG, with non-specific or no initial ECG changes in the remainder
- Make the diagnosis based of troponins in this case
- The ECG in a patient with pericarditis shows diffuse, concave ST-segment elevation with PR depression
- If the first ECG is non-diagnostic repeat after 15 minutes if the chest pain is continuing
- Repeat the ECG whenever the chest pain recurs, stops or changes in severity or character, as well as after 6–8 hours with repeat cardiac biomarkers (troponin) to rule out ACS
- Blood pressure?
Immediate Management
- Call senior for:
- Persistent hypoxia, hypotension or altered mental status despite the above measures
- HR >150 beats/min or <40 beats/min associated with hypotension as cardioversion or pacing may be required
- Persistent pain and ST segment changes on ECG; need senior input to determine if STEMI is due to atherosclerosis or alternative cause
- Position the patient in the position of comfort
- A
- Address any airway compromise (see Acute Airway Failure)
- Attach continuous non-invasive ECG, BP and pulse oximeter monitoring to the patient
- B
- Commence oxygen if hypoxic or shocked to maintain oxygen saturation >94%
- High-dose 40-60% oxygen unless obstructive airway disease ⇒ 28% Venturi mask
- Commence oxygen if hypoxic or shocked to maintain oxygen saturation >94%
- C
- For possible STEMI or high risk ACS with haemodynamic compromise move patient to the resuscitation area and/or attach patient to a defibrillator
- Commence or continue initial therapy for acute chest pain of possible cardiac origin:
- Aspirin 300 mg orally, chewed or dissolved before swallowing

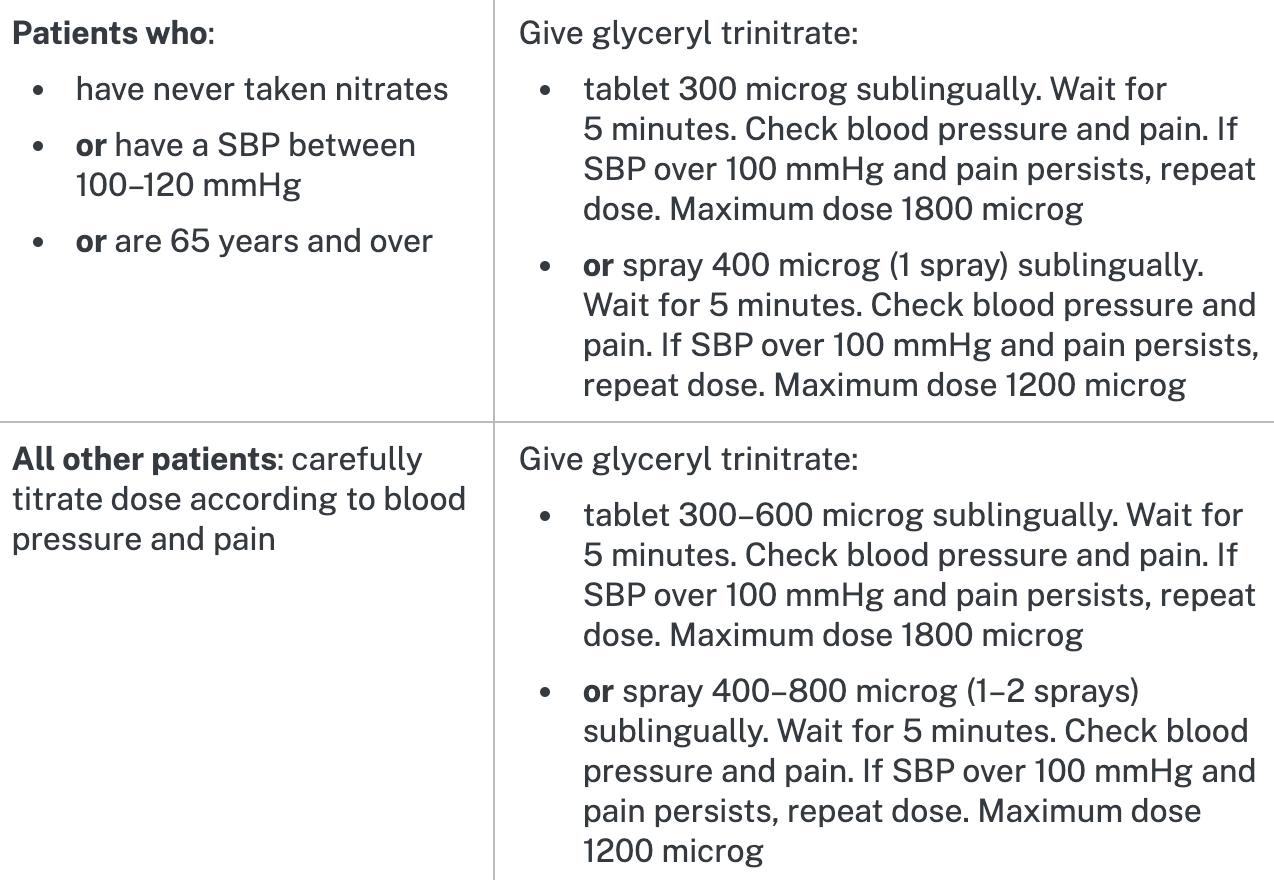
- GTN Spray (400-800 micrograms) or tablet (300-600 micrograms SL) x1
- If SBP >90mmHg (and ongoing chest pain)
- Second dose of GTN 300-600 microgram SL and a third after 5 more minutes if pain still present; caution in right-sided and inferior infarcts → try look at ECG first (II, III, avF)
- Give morphine 2.5-5mg IV with metoclopramide 10-20mg IV for nausea, if pain persists despite two to three doses of GTN
- Can also use fentanyl 25-50 microgram IV as an initial dose repeated every 5 to 10 minutes if required
- Older patients start at lower end of dose range
- If SBP <90mmHg
- Check that the lung bases are clear to auscultation and give a bolus of 125-250mL IV normal saline
- If bases has signs of pulmonary oedema with an S3 gallop tachypnoea and basal crackles, treat as cardiogenic shock
- Aspirin 300 mg orally, chewed or dissolved before swallowing
- Establish IV access with two cannulae in peripheral veins if not done so already
- Draw and send bloods for: FBC, UEC, cardiac biomarkers (troponin I and T) and caogulation profile
- Examine for signs of shock: (tachcardia and CRT ≥3 seconds) and/or abnormal skin perfusion and/or hypotension (see Shock)
- If shock (as above) and/or SBP <90mmHg give 250mL of 0.9% saline bolus
- Monitor patients with CCF for signs of fluid overload
- Consider IV metoprolol if in sinus tachycardia and the patient is not hypotensive and demand ischaemia is the suspected cause of chest pain
- D
- Measure GCS
- Manage pain (see Pain Management) if not done so already
- Mild: paracetamol 1000mg oral
- Moderate: (+paracetamol 1000mg oral)
- Oxycodone
- 16-65 years: 5mg oral, repeat if required after 30 minutes, max dose 10mg
- ≥65 years: 2.5mg oral, repeat after 30 minutes, max dose 5mg
- Oxycodone
- Severe: (do not give morphine or fentanyl if SBP <100mmHg)
- Morphine IV
- 16-65 years: 5mg IV, repeat if required after 5 minutes, max dose 10mg
- ≥65 years: 2.5mg IV, repeat if required after 5 minutes, max dose 5mg
- OR Fentanyl IV
- 16-65 years: 50mcg IV, repeat after 5 minutes, max dose 100 mcg
- ≥65 years: 25mcg IV, repeat after 5 minutes, max dose 50mcg
- Morphine IV
- Exposure
- Measure temperature
- Fluids
- Commence fluid balance chart as required
- Manage nausea and vomiting if not done so already
- metoclopramide 10 mg orally or IV/IM once only (over 20 years only)
- or ondansetron 4 mg orally or IV/IM. If symptoms persist after 60 minutes, repeat once, maximum dose 8 mg
- or prochlorperazine 5 mg orally once only or 12.5 mg IV/IM once only
- Glucose
- Measure BGL
- If BGL<4mmol/L and NO ↓LOC → give sugary drink
- If BGL<4mmol/L and ↓LOC → glucose 10% 200mL by infusion over 15 minutes once only or glucagon 1mg IM
- Portable CXR
As from: https://aci.health.nsw.gov.au/ecat/adult/chest-pain and eTG: Acute Chest Pain of Possible Cardiac Origin
Selective History and Chart Review
- Onset of the chest pain?
- Crescendo, build-up of pain ⇒ ACS
- Sudden onset ⇒ PE, aortic dissection, oesophageal rupture
- With physical exertion or emotional stress ⇒ ACS
- With coughing ⇒ Pneumothorax, also see Cough
- Sudden onset + vomiting ⇒ oesophageal rupture
- Character of pain?
- Get a score and get the patient to rescore to get an ongoing evaluation
- Is the pain like the patient’s previous usual angina pain?
- Crushing, vice-like or squeezing pain is characteristic of ACS, but note that ‘atypical’ pain still due to ACS occurs in women, elderly people and those with diabetes and renal impairment
- Tearing or ripping pain is characteristic of an AAD. Likewise, severe pain that is poorly relieved by large doses of morphine suggests an aortic dissection or an oesophageal rupture
- Sharp, well-localised pain suggests a pleuritic or musculoskeletal origin
- Related symptoms?
- Nausea, sweating and light headedness
- Collapse or syncopal episode should be taken seriously
- Dyspnoea
- Alleviating or aggravating factors?
- Worse on coughing or deep breathing → pleuritic chest pain ⇒ Pneumothorax, Pericarditis, PE, Pneumonia, rib fracture or costochondritis
- Worse on deep inspiration, lying flat or when raising both legs ⇒ Pericarditis
- Worse on swallowing ⇒ oesophageal source or Pericarditis
- Specific movements ⇒ MSK
- PMHx
- ACS is more likely when:
- Ischaemic heart disease
- Increasing age >65 years
- Comorbid conditions: Diabetes, hypertension, smoking, hyperlipidaemia or end-stage renal disease
- Family history of premature ischaemic heart disease in first-degree relative under age 50 years
- Aortic dissection is more likely when:
- Aged 60-80
- Male with chronic hypertension
- Younger patients with connective tissue disorder (e.g. Marfan’s or Ehler-Danlos syndrome)
- Family history
- PE is more likely when:
- Recent surgery, immbolisation, malignancy, prior VTE
- Family history of 1° relative with thromboembolism
- ACS is more likely when:
- Charts:
- Confirm prescribed antianginal medications are given
- Check for DVT prophylaxis
- Check for corticosteroids or NSAIDs as a possible cause of gastritis or oesophagitis
Examination
| Examination | Notes |
|---|---|
| Vitals | Repeat |
| Appearance | Marfanoid appearance? Tall thin patient with long lmbs and arachnodactyly ⇒ ↑ risk of aortic dissection |
| HEENT | Xanthelasma around eyelids |
| Exudate in oral cavity or pharynx | |
| Resp | Asymmetrical expansion of the chest (pneumothorax, large pleural effusion or massive haemothorax) |
| Tracheal deviation (away ⇒ pneumothorax, effusion or towards ⇒ collapse, consolidation) | |
| Percussion (hyperresonance ⇒ pneumothorax, dullness ⇒ effusion, consolidation) | |
| Auscultation (↓ breath sounds ⇒ pneumothorax, pleural rub ⇒ PE or pneumonia, crackles ±wheeze ⇒ pulmonary oedema, PE or pneumonia) | |
| Chest wall | Tender costal cartilage (costochondritis) |
| Localised rib pain ⇒ rib fracture | |
| CVS | Unequal carotid pulses ⇒ aortic dissection |
| Unequal upper limb BP or ↓ radial or femoral pulses ⇒ aortic dissection | |
| ↑JVP ⇒ biventricular failure with CCF, RV failure secondary to PE, tension pneumothorax or cardiac tamponade | |
| LV heave ⇒ LV failure | |
| RV heave ⇒ acute RV failure 2° to PE | |
| Auscultation | S3 gallop ⇒ LV failure, Loud P2 ⇒ Acute RV failure 2° cor pulmonale |
| Muffled heart sounds ⇒ cardiac tamponade, pericarditis | |
| Systolic murmur: AS ⇒ angina MR ⇒ acute papillary muscle or chordae tendinae dysfunction 2° to ACS Late ⇒ MVP (Barlow’s syndrome) | |
| Diastolic murmur: Early ⇒ aortic regurgitation associated with proximal aortic root dissection Pericardial rub ⇒ pericarditis | |
| GIT | Guarding, rigid abdomen ⇒ perforated peptic ulcer |
| Epigastric tenderness ⇒ peptic ulcer disease | |
| Generalised abdominal pain ⇒ mesenteric infarction from aortic dissection | |
| Skin | Unilateral, vesicular maculopapular rash, dermatomal distribution ⇒ herpes zoster |
Investigations
- Bedside:
- ECG
- POCUS
- Acutely ↓ contractility ⇒ ACS
- Lack of lung sliding ⇒ Pneumothorax
- Dilated RV and flattening of LV septum ⇒ PE
- Pericardial effusion ⇒ Pericarditis
- Bloods:
- Take blood for FBC, coags, BSL, UEC, LFT, cardiac enzymes
- D-dimer if low pre-test probability for PE
- Repeat cardiac biomarkers 6-8 hours after
- Accelerated chest pain rule-out protocol
- Imaging:
- CXR
Specific Management
- See STEMI Management
- See NSTEACS Management
- See Aortic Dissection Management
- See Pericarditis Management
- See PE Management
- Oesophagitis
- Give an antacid 15-20mL every 2 hours in the acute phase, then TDS after meals and once before bedtime
- Prescribe a PPI (e.g. omeprazole 20-40 mg PO OD) or H2RA (e.g. rantidine 150mg PO BD)
- Advice lifestyle modification such as stopping smoking, reducing alcohol consumption, omitting hot or spicy food from the diet, eating small meals regularly during the day and not eating immediately before sleep
- Refer for endoscopic evaluation and H. pylori testing
- MSK causes
- Palpate and compress the chest wall to identify a tender muscle, fractured rib(s) or tender costochondral junction. Palpate and gently percuss the spine to identify a crush fracture, which may be causing referred dermatomal pain.
- The ECG is normal and other investigations are unhelpful.
- Treat musculoskeletal causes of pain with an NSAID, such as ibuprofen 400 mg PO TDS or naproxen 250–500 mg PO TDS
- Anxiety and panic disorders
- Due to the possibility of a life-threatening cause of chest pain, panic and anxiety disorders are always a diagnosis of exclusion → discuss the patient with your senior
- Attempt to control the hyperventilation by reassurance
- Alternatively, ask the patient to re-breathe into a paper bag or mask to control the ventilatory loss of
- Give diazepam 2-5mg PO or lorazepam 1-2mg SL acutely if there is no response to the initial treatment or the attack recurs
Other Resources