Soft-tissue retraction-tracheal tug, rib or abdominal recession
Loss, or an uncoordinated rise and fall, of the chest and/or abdomen
‘See-saw’ pattern of chest and abdominal movement: the chest is drawn in and the abdomen expands on inspiration and the opposite occurs on expiration
Altered level of consciousness or mental status or agitation
GCS ≤8
Features of partial airway obstruction
Tripod position
Reluctance to speak or cough
Increased work of breathing with nasal flaring accessory muscle use
Inspect
Upper airway for foreign material if possible or using laryngoscopy
Erythema or urticaria with lip, tongue or palatal swelling
Listen for bronchospasm and examine for circulatory features that suggest Anaphylaxis
Localised trauma, burns infection or tumour
Palpate the anterior neck, including the thyroid cartilage for pain, inflammation, crepitus, swelling or masses
Investigate for any cause of depressed consciousness (e.g. hypoglycaemia or opioid intoxication)
Signs and features of complete airway obstruction
No stridor, airway sounds or breath sounds on lung auscultation
Inability to ventilate the patient with a bag-mask
Rapid development of cyanosis and unconsciousness
Call senior immediately
MET call should be made for any patient with a threatened airway (including partial airway obstruction)
Management
General measures
Administer high-flow oxygen and reverse cause of depressed consciousness
Apply non-invasive monitoring, including ECG, pulse oximeter and BP
Obtain reliable IV access
Call senior for help and summon staff experienced in airway management
Reposition the patient if in coma
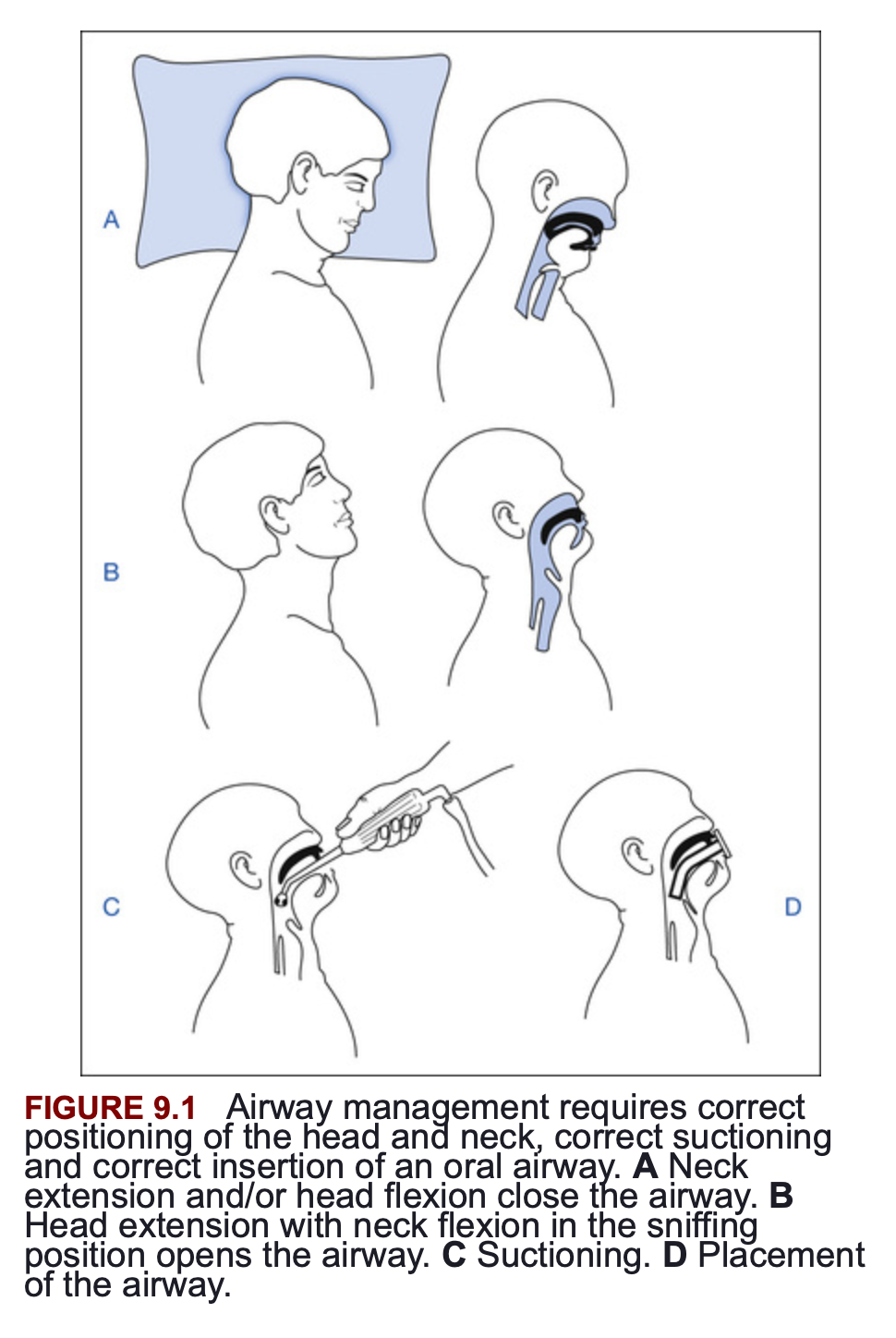
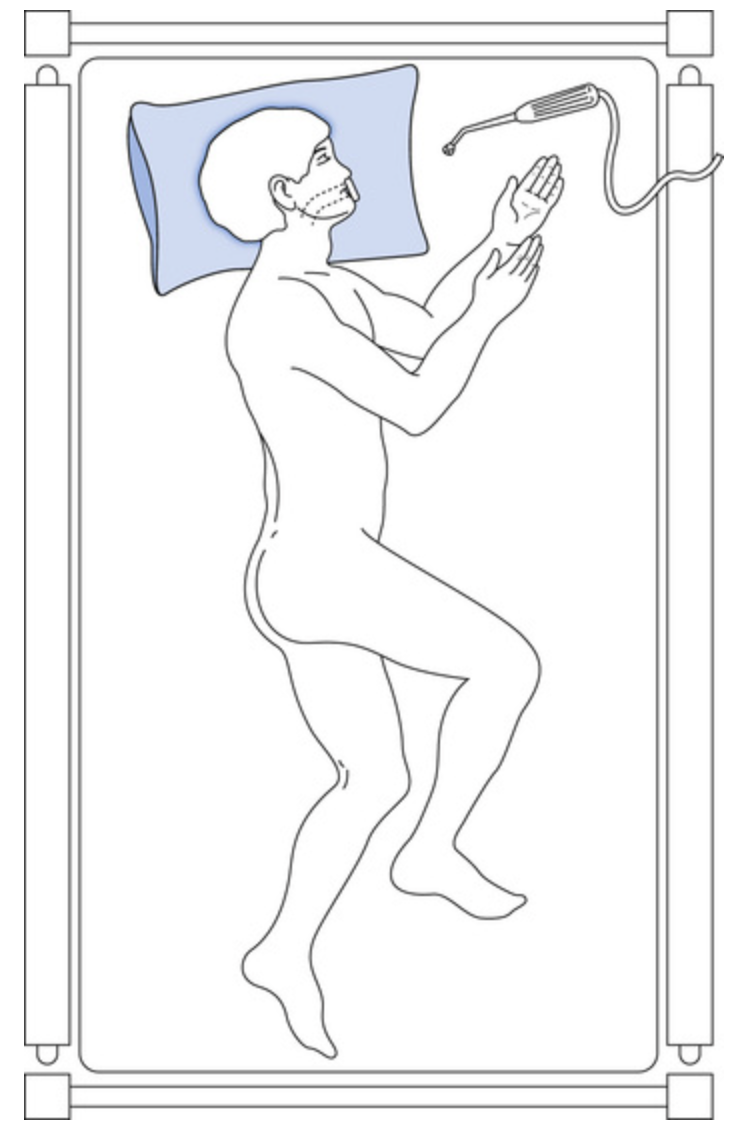
Flex neck at cervicothoracic junction and extend head at the cervico-occipital junction (‘sniffing position’) provided no neck trauma; place pillow or support behind the head
Head tilt: tilt the head gently back with pressure on the forehead
Jaw thrust: place fingers behind the angle of the mandible and push the jaw forwards to life the soft tissues away from the pharynx to relieve obstruction
Apply with head tilt unless possibility of spine injury
Chin lift
Single operators at the side of the patient for expired air resuscitation when combining with CPR (BLS)
Recovery position: left lateral position to keep airway open and assist in drainage of secretions
Clear foreign material
Manually remove any intra-oral foreign body (e.g. loose-fitting dentures)
Suction secretions and smaller foreign material using a large-bore rigid (Yankauer) sucker
Laryngoscope and Magil forceps if material is lodged in the upper airway
Can consider insertion of a nasogastric tube to empty the stomach
Airway adjuncts
Oropharyngeal (Guedel) airway
Sized using distance from the angle of the jaw to the centre of the lips
Remember to insert upside down and then rotate
Not tolerated in a semiconscious patient who will gag or develop laryngospasm
Nasopharyngeal airway
Sized from the tip of the nose to the tragus of the ear (size 6 or 7 is suitable for adults)
Consider spraying the nasal cavity with vasoconstrictor/anaesthetic spray to prevent bleeding and decrease discomfort
Lubricate airway thoroughly
Better tolerated in semiconscious patient and may be used in patients with clenched jaws or trismus (e.g. during seizure)
Laryngeal mask airway
Most LMAs have a patient weight range printed on them, assisting the choice of the correct size
The outer lip of the cuff must be lubricated, then the LMA is inserted through the mouth and pushed backwards against the palate with a confident thrust until resistance is felt from the pharynx
The cuff is inflated and ventilation is commenced
Endotracheal intubation
Search and treat underlying cause
Local trauma: stabilise fracutres, re-position, stop bleeding by local pressure or pack and call surgeon
Local infection: call ENT and commence antibiotics, drain any abscess (e.g. Ludwig angina) and consider IV steroids to decrease oedema
Local tumour: consider steroids to decrease oedema and arrange ENT assessment
Angio-oedema
Hereditary angio-oedema: Urgent C1 esterase inhibitor IV or icatibant 30 mg in 3 mL SC (B2-receptor antagonist)
Choking
Allow the patient to clear the obstruction by coughing
Usually more effective than chest compression
Be prepared to assist if the patient has a weak cough or depressed consciousness
Give five firm blows to the back if the patient cannot breath or cough
If unsuccessful give five chest compressions; similar to CPR but performed more slowly with a more prolonged compression time
Continue this cycle until the obstruction is cleared or the patient becomes unconscious
If the patient becomes unconscious
Commence CPR
Suction the airway
Under direct visualisation at laryngoscopy remove the foreign material with Magill foreceps
Only use a finger sweep to clear an airway if solid material is visible