Presentation
- Patients have breathlessness, cough, sputum production and wheeze, and are susceptible to infections. Most patients have a smoking history.
- Bronchiectasis is a less common cause of obstructive lung disease with chronic productive cough, and halitosis.
- Chronic bronchitis, emphysema and asthma overlap, as some reversibility is present with COPD and some patients with asthma will develop irreversible components of the disease
- Typically older than 35 who are smokers or ex smokers with breathlessness, cough, recurrent respiratory tract infection, sputum production
- Suspect alpha-1-antitrypsin deficiency in patients in whom COPD develops at a young age (<40 years), particularly if they have a family history of COPD
Differences with Asthma Exacerbation
- COPD features:
- Onset after age 40
- Persistent airflow limitation
- Lack of response to asthma therapy (e.g. symptoms persisting despite ICS treatment)
- Heavy tobacco smoke exposure
- Asthma features:
- Onset before age 20
- Significant day-to-day variability in airflow limitation and symptoms
- normal lung function between symptoms
- Symptoms worse at night or in the early morning
- Family history of asthma or atopy
- Seasonal variability in symptoms
- Spontaneous improvement in symptoms
Investigations
Lung Function Testing
- A postbronchodilator FEV1/FVC ratio less than 0.7 is diagnostic of COPD.
Chest-Xray
- Hyperinflation of the lungs with flattened diaphragms
- Increased anteroposterior diameter
- Occasional infiltrates
- Occasionally pneumomediastinum
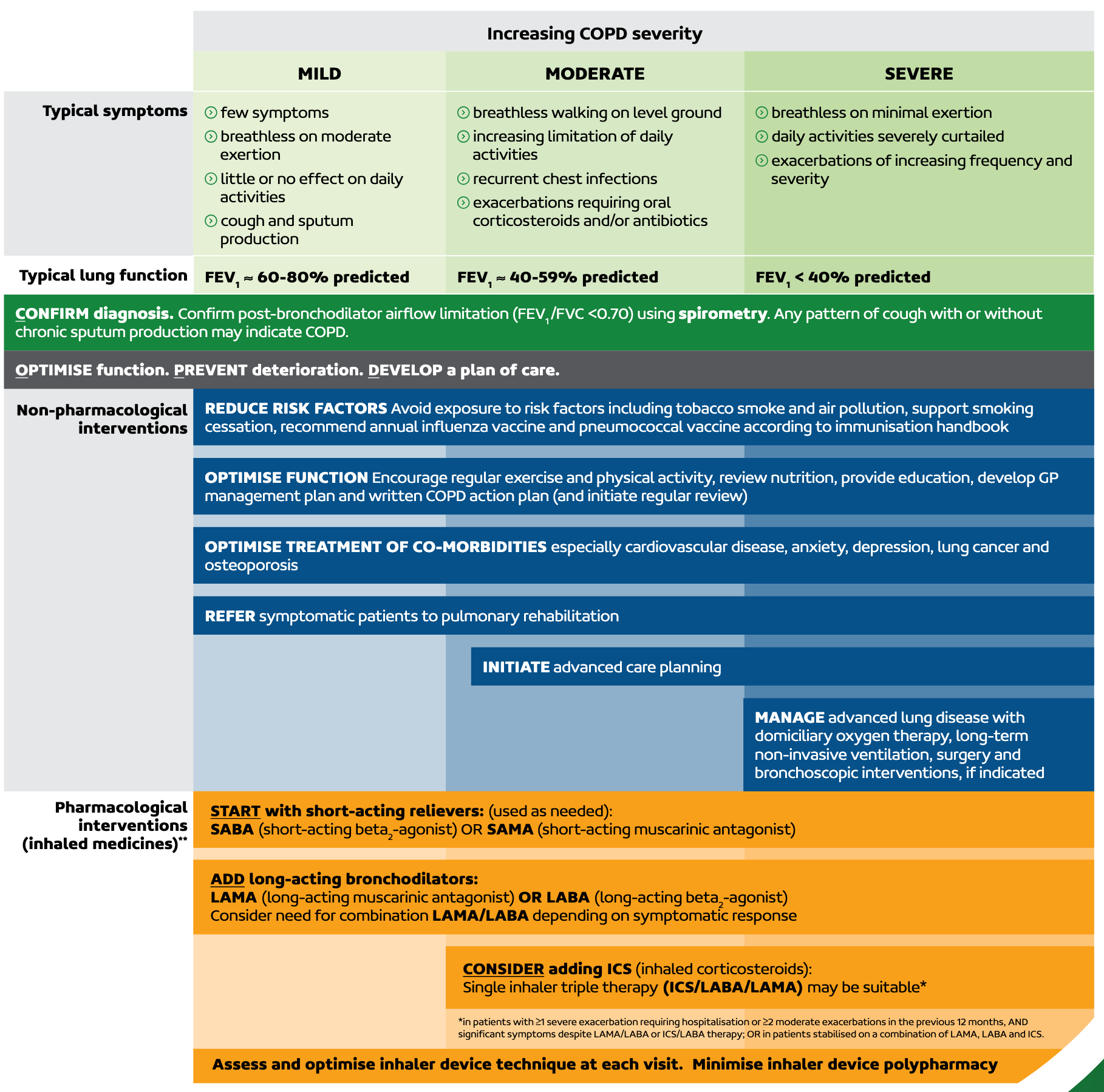
Assessment of Severity
| Mild | Moderate | Severe | |
|---|---|---|---|
| Symptoms and exacerbation history | Few symptoms Breathless on moderate exertion Daily activities minimally limited or unaffected Cough and sputum production | Breathless walking on level ground Daily activities increasingly limited Recurrent chest infections Exacerbations requiring oral corticosteroids or antibiotics | Breathless on minimal exertion Daily activities severely limited Exacerbations of increasing frequency and severity |
| Typical lung function | FEV1 60-80% of predicted | FEV1 40-59% of predicted | FEV1 < 40% of predicted |
Management of Stable COPD
- Non-pharmacological
- Smoking cessation
- Physical activity
- Pulmonary rehabilitation
- Maintenance of up-to-date vaccination
- Good nutrition
- Pharmacological
- Usually progresses int he following order
- SABA (salbutamol 100-200 mcg PRN or terbutaline 500 mcg PRN)
- LABA or LAMA monotherapy
- Indicated when SABA and non-pharm measures not adequate
- Options include:
- LAMA: aclidinium, glycopyrronium, tiotropium, umeclidinium
- LABA: indacaterol
- LABA + LAMA
- LABA + LAMA + ICS
- Indicated if both:
- Patient has severe exacerbations (requiring hospitalisation) or at least two moderate exacerbations in previous 12 months and
- Patient has significant symptoms despite dual therapy with LAMA + LABA
- Indicated if both:
- Assess 3-6 months after starting treatment and in those who remain symptomatic or have continued exacerbations, check inhaler technique and adherence before stepping up therapy
- Usually progresses int he following order
- Additional therapy
- Home oxygen
- Oral mucolytics (bromhexine)
- Long term macrolide antibiotics
Other Notes on Management
- Beta blockers should not be stopped in patients with COPD and HFrEF or a Myocardial Infarction within the last 3 years
- Patients with COPD are at an increased risk of bone fractures; identify patients with Osteoporosis
- Limit the use of oral corticosteroids in patients with COPD and diabetes
- Mild to moderate Pulmonary Hypertension is common in patients with COPD