Symptoms
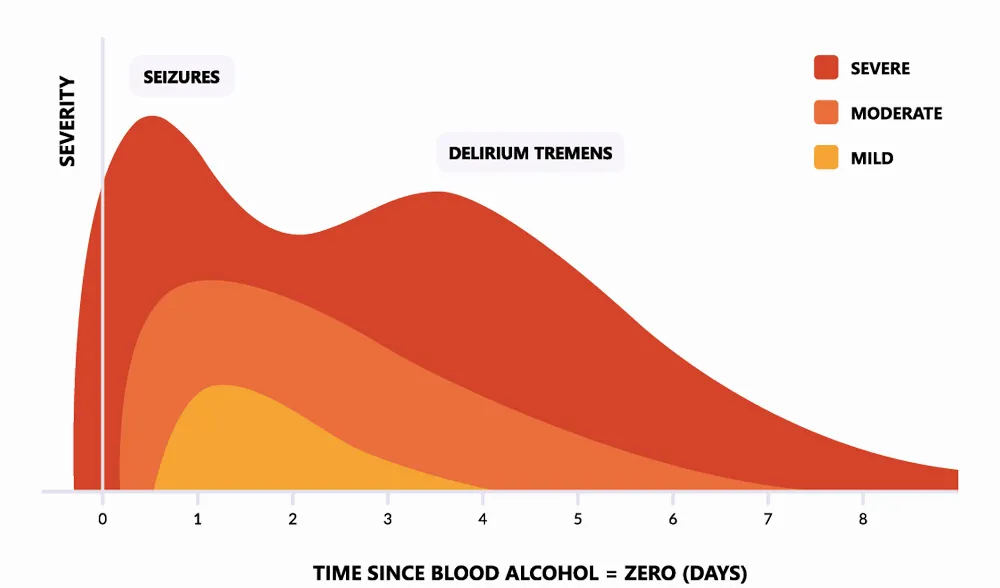
- Alcohol withdrawal seizures typically occur between 6-24 hours after the last drink is consumed
- Alcohol withdrawal seizures are typically followed by features of adrenergic activity such as:
- Tachycardia, agitation, sweating
- A calm, drowsy post-ictal patient is likely to have a comorbid seizure disorder.
- This helps to differentiate with seizures due to other causes. Alcohol withdrawal seizures are usually:
- brief (not longer than 30 to 60 seconds)
- generalised
- seen in people with alcohol dependence with a long history of high alcohol intake
- evident early in withdrawal
- Alcohol withdrawal delirium typically occurs between 2-3 days after the last drink is consumed
Management
Diet Nutrition and Rehydration
- Consider fluid chart
- Check magnesium levels and replace if deficiency identified
- IV fluids may be necessary
Thiamine and Other Supplements
- Provide thiamine to all patients undergoing alcohol withdrawal before any carbohydrate load
- Healthy patients with good dietary intake should be administered oral thiamine 300mg per day for 3 to 5 days, and maintained on 100mg oral thiamine for a further 4 to 9 days (total of 1 -2 weeks of thiamine)
- People with chronic alcohol use with poor dietary intake and general poor nutritional state should be administered parenteral (IM or IV) thiamine doses of 300mg per day for several days, with subsequent oral thiamine doses of 300mg per day for several weeks
- Continue thiamine in alcohol dependent patients who continue to drink alcohol
Pharmacotherapy
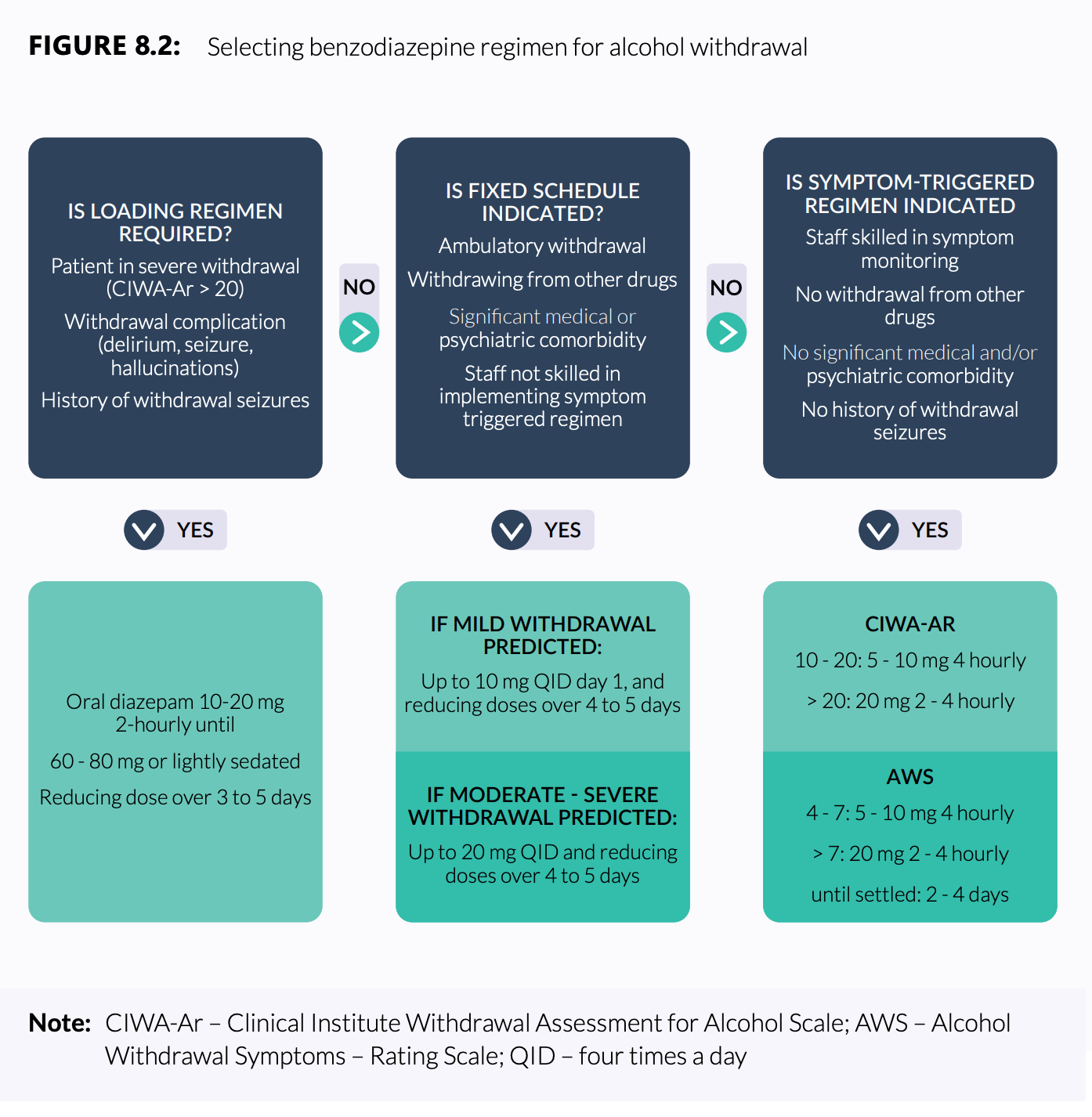
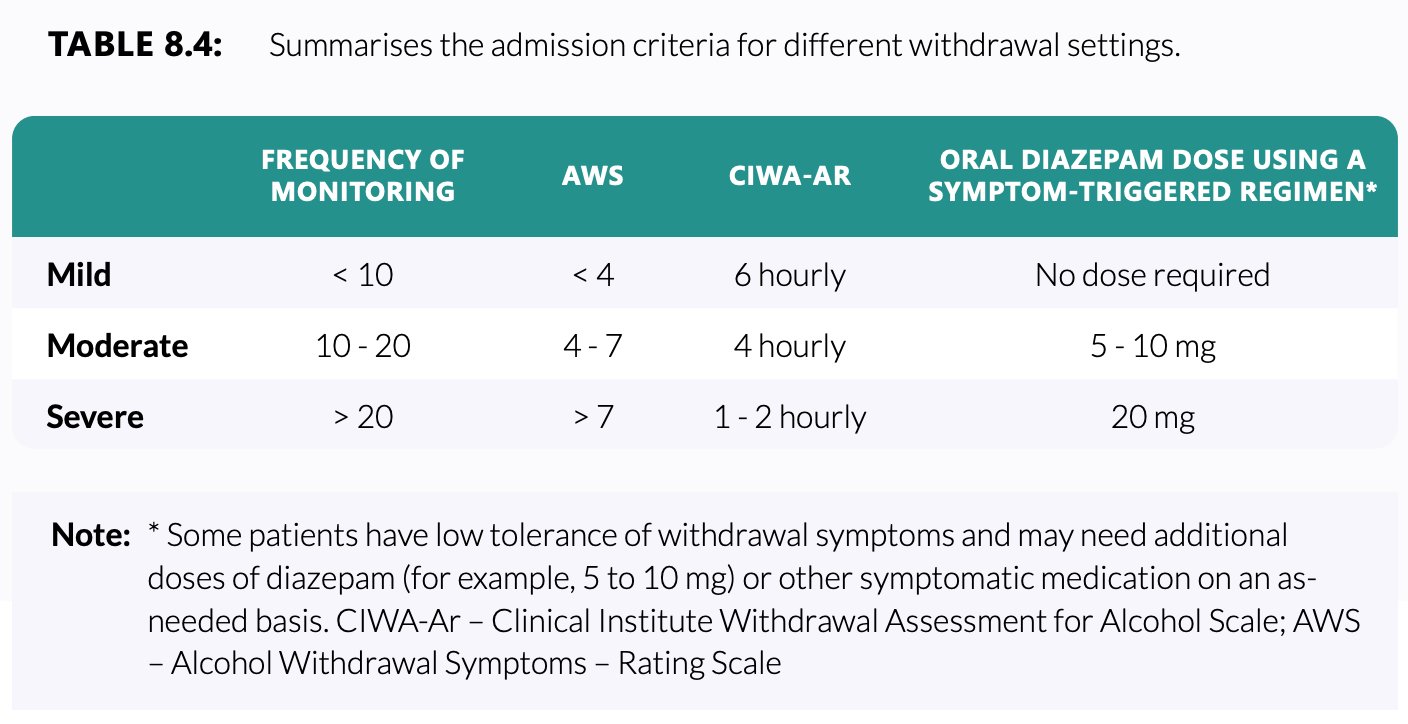
- Symptom triggered therapy (for patients with low risk of seizures or withdrawal complications)
- Diazepam 5-10mg PO 4-6 hourly as required to control symptoms typically for 1-2 days
- Diazepam 5-10mg PO 4-6 hourly as required to control symptoms typically for 1-2 days
- Loading dose therapy
- Indicated for patients:
- With a history of severe withdrawal complications (seizures, delirium)
- Patients presenting in severe alcohol withdrawal and/or severe withdrawal complications (delirium, hallucinations or following an alcohol withdrawal seizure)
- A common diazepam-loading regimen under these circumstances is 10- 20 mg orally every 1- 2 hours (eg 10 mg hourly) until 60–80 mg is reached or the patient is sedated
- Medical review should occur if the patient remains agitated after 80 mg or 4 hours
- Indicated for patients:
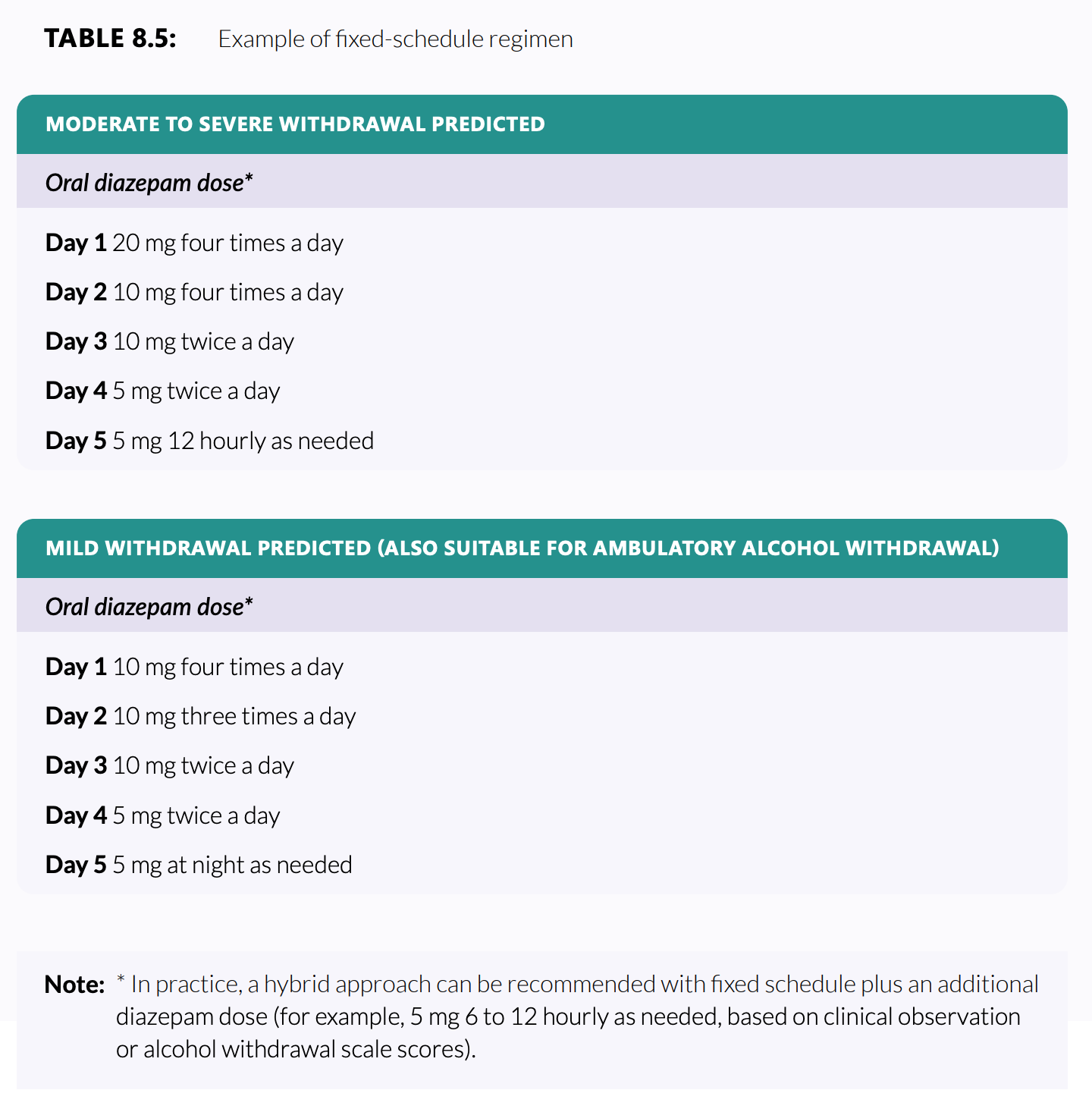
- Fixed schedule therapy
- Appropriate for complex hospitalised patients, ideally with daily review by specialist drug and alcohol clinicians
- Appropriate for complex hospitalised patients, ideally with daily review by specialist drug and alcohol clinicians
- Choice of benzodiazepine
- Diazepam is usually the benzodiazepine of choice1 but avoid in patients where there is concern about prolonged sedation:
- Elderly
- Recent head injury
- Liver failure
- Respiratory failure
- Other serious medical illness
- Severely obese patients
- Lorazepam is usually next preferred; 2mg lorazepam PO is equipotent to 10mg diazepam PO
- Diazepam is usually the benzodiazepine of choice1 but avoid in patients where there is concern about prolonged sedation:
Sources
- https://alcoholtreatmentguidelines.com.au/pdf/guidelines-for-the-treatment-of-alcohol-problems.pdf from page 116 onwards
- eTG: Alcohol withdrawal
- AMH Online: Alcohol withdrawal
Footnotes
-
Chlordiazepoxide is not registered in Australia ↩