Part of: Mechanical Ventilation
- Ventilator modes are just pre-set combinations of ventilator settings
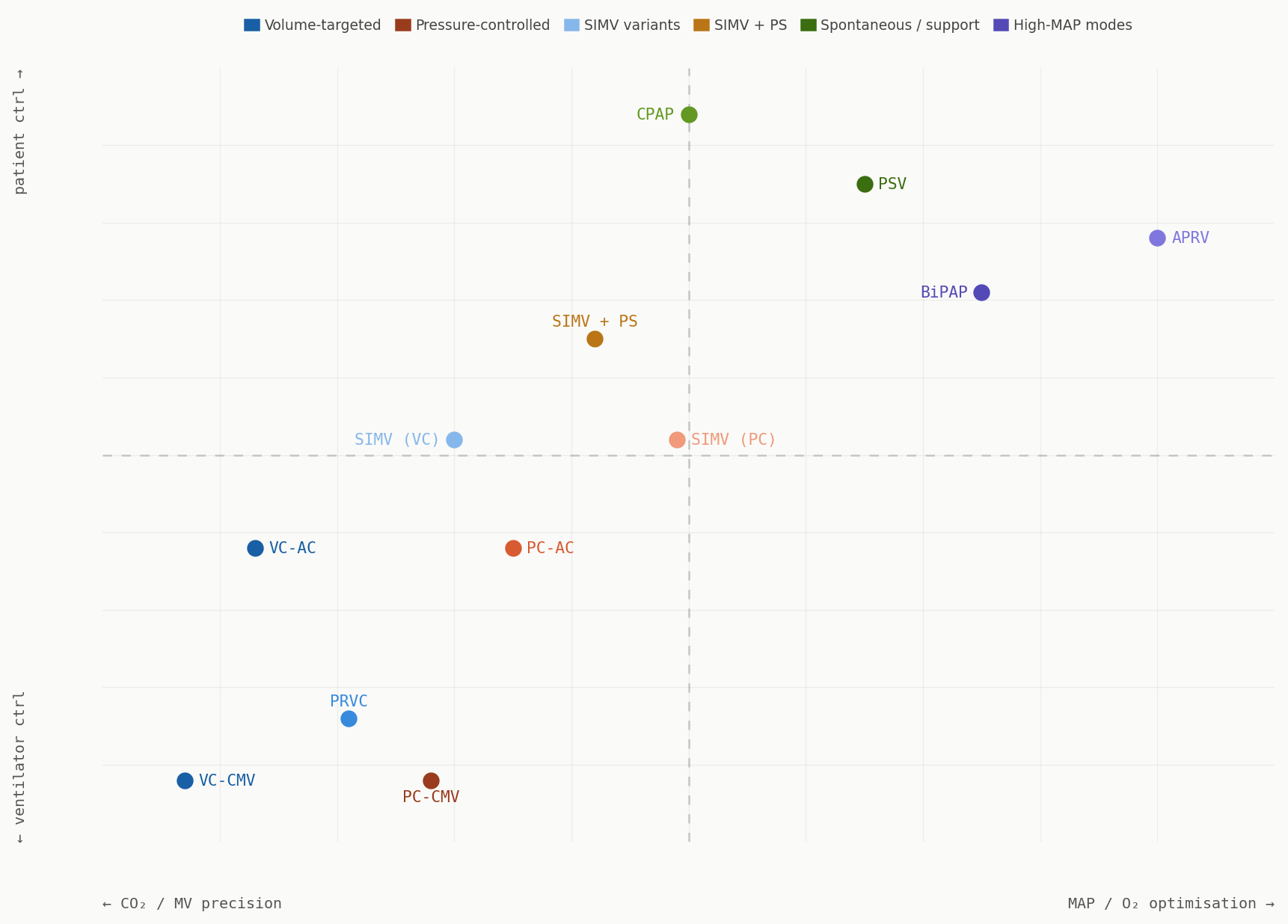
- Generally classified according to their major characteristics:
- The control variable: pressure vs. volume
- Breath sequence: spontaneous vs. mandatory
- Targeting scheme: set point, dual targeting, servo control, adaptive etc.
Continuous Mnadatory Ventilation (CMV)
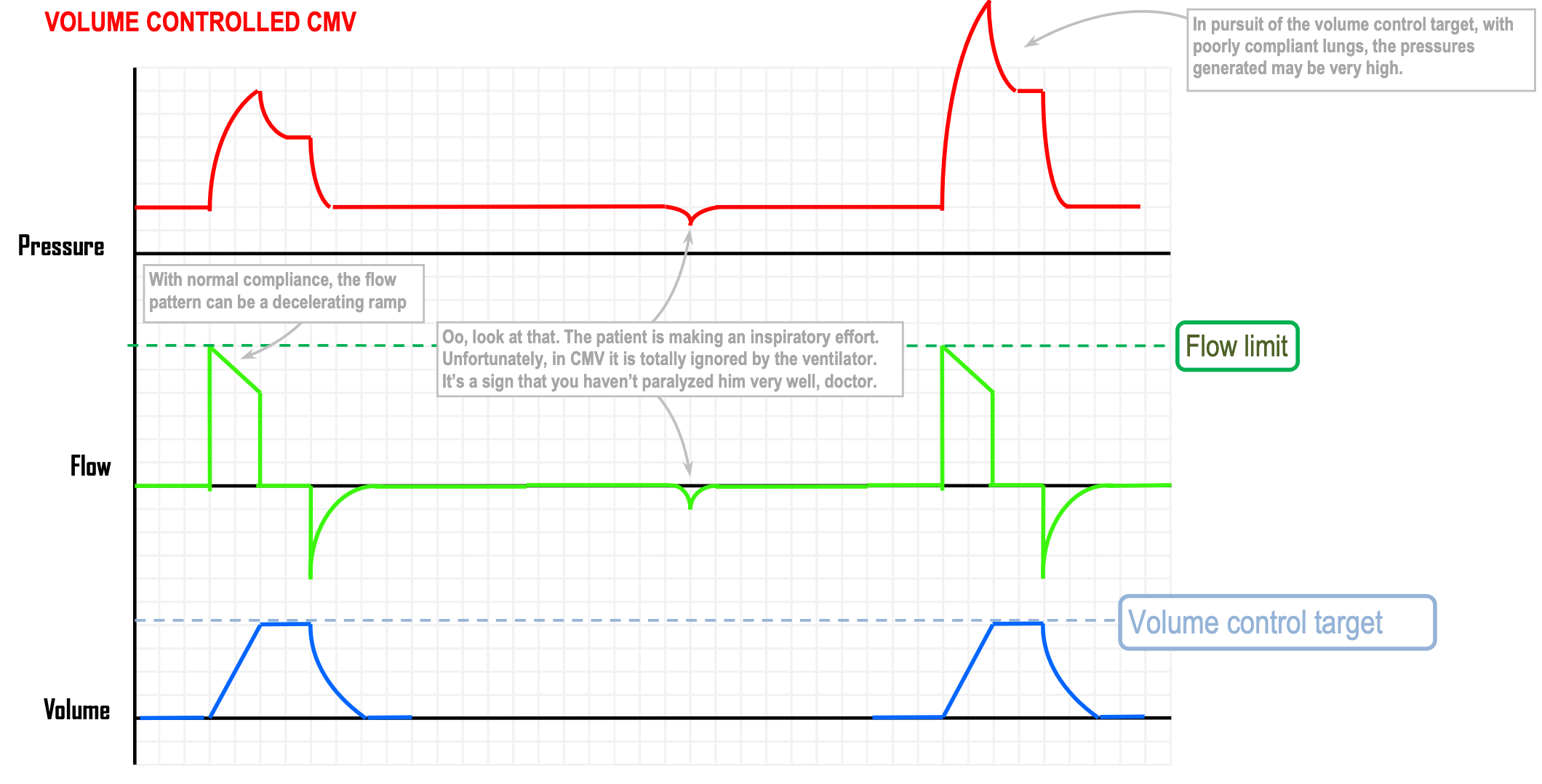
- The main feature is that it ignores attempts at breathing and all components of the respiratory phase delivered by the ventilator are mandatory (i.e. controlled by time)
- This means it is time triggered and typically time cycled
- Control variable: Typically volume controlled but can be pressure
- Time triggered
- Volume, pressure or flow limited
- Time-cycled but can be volume cycled to avoid an inspiratory pause
- Advantages:
- Gives optimal control over minute volume; therefore useful when maintaining a narrow range (e.g. in a paralysed sedated head injury patient)
- Disadvantages
- Uncomfortable; requires decent sedation
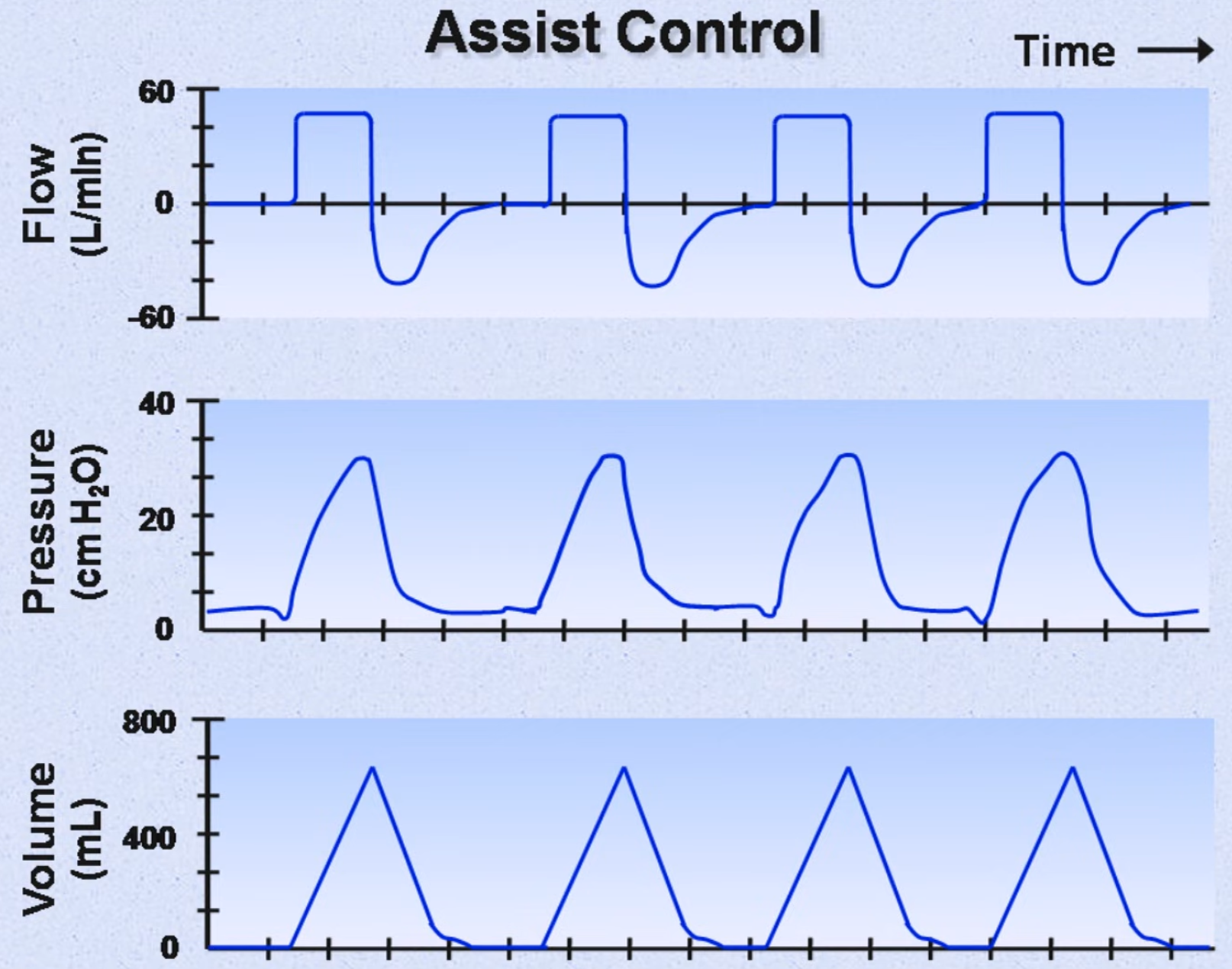
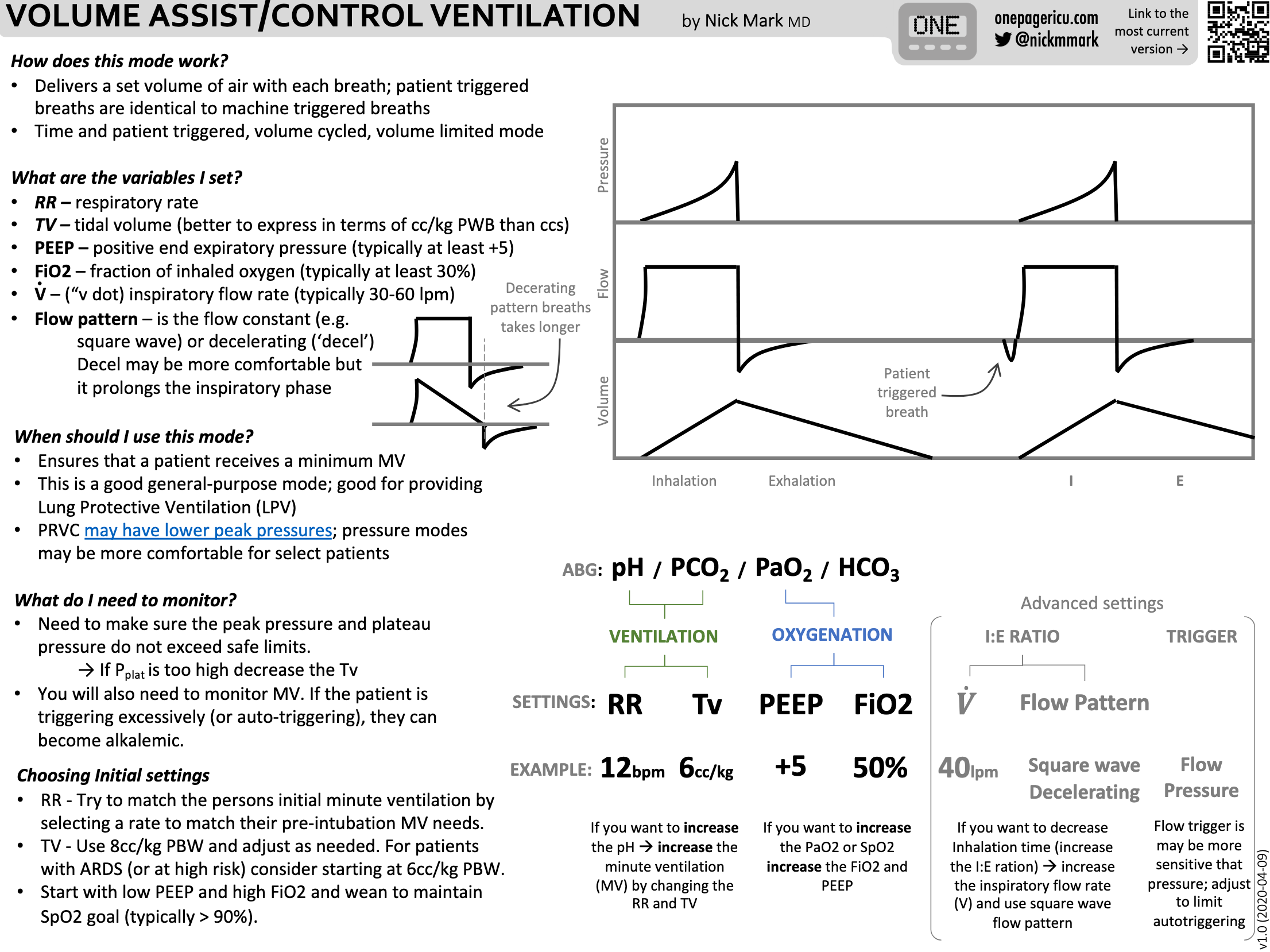
Assist Control (AC)
- Mix of mandatory and assisted breaths with all breaths, once triggered, are treated the same and have a consistent tidal volume
- Trigger: time, pressure or flow
- Control: flow (volume)
- Cycling: time but can be volume cycled to avoid inspiratory pauses
- Advantages
- Guarantees a minimum minute ventilation
- Low work of breathing
- Disadvantages
- Can lead to respiratory alkalosis, auto-PEEP and hypotension in hyperventilating patients as every breath leads to a fully supported breath
- Uncomfortable
- Indications
- Critically ill patients requiring full ventilatory support and in whom fluctuations in is undesirable
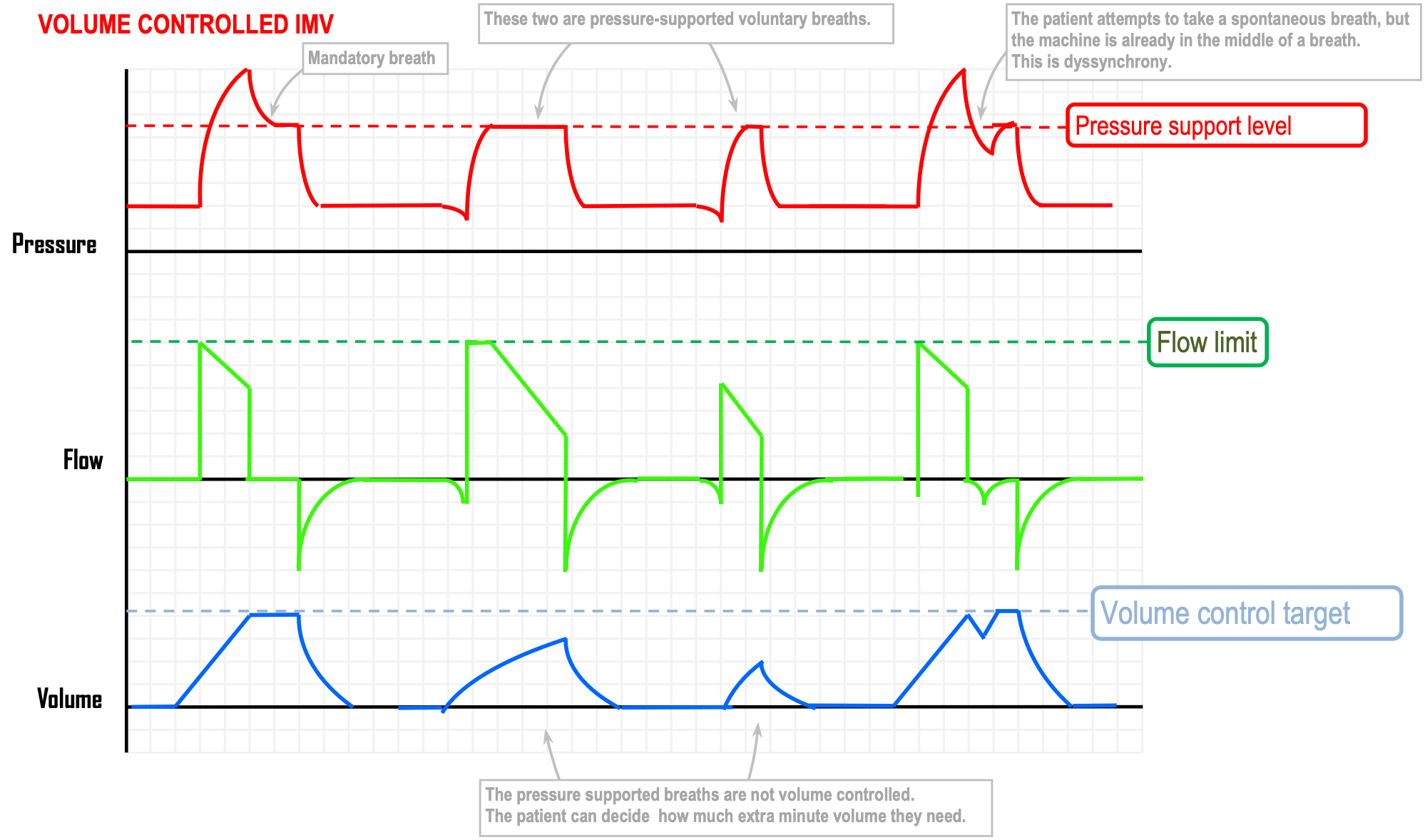
Intermittent Mandatory Ventilation (IMV)
- Not continuously mandatory, the patient can decide their own respiratory rate and take a number of pressure supported breaths; the machine also gives a set number of mandatory breaths
- Advantages:
- Guarantees a minimum minute ventilation
- Guarantees a minimum minute ventilation
- Mandatory breaths are volume controlled
- Mandatory breaths are time triggered and the pressure supported breaths are flow triggered
- Time cycled but can be volume cycled to avoid inspiratory pauses
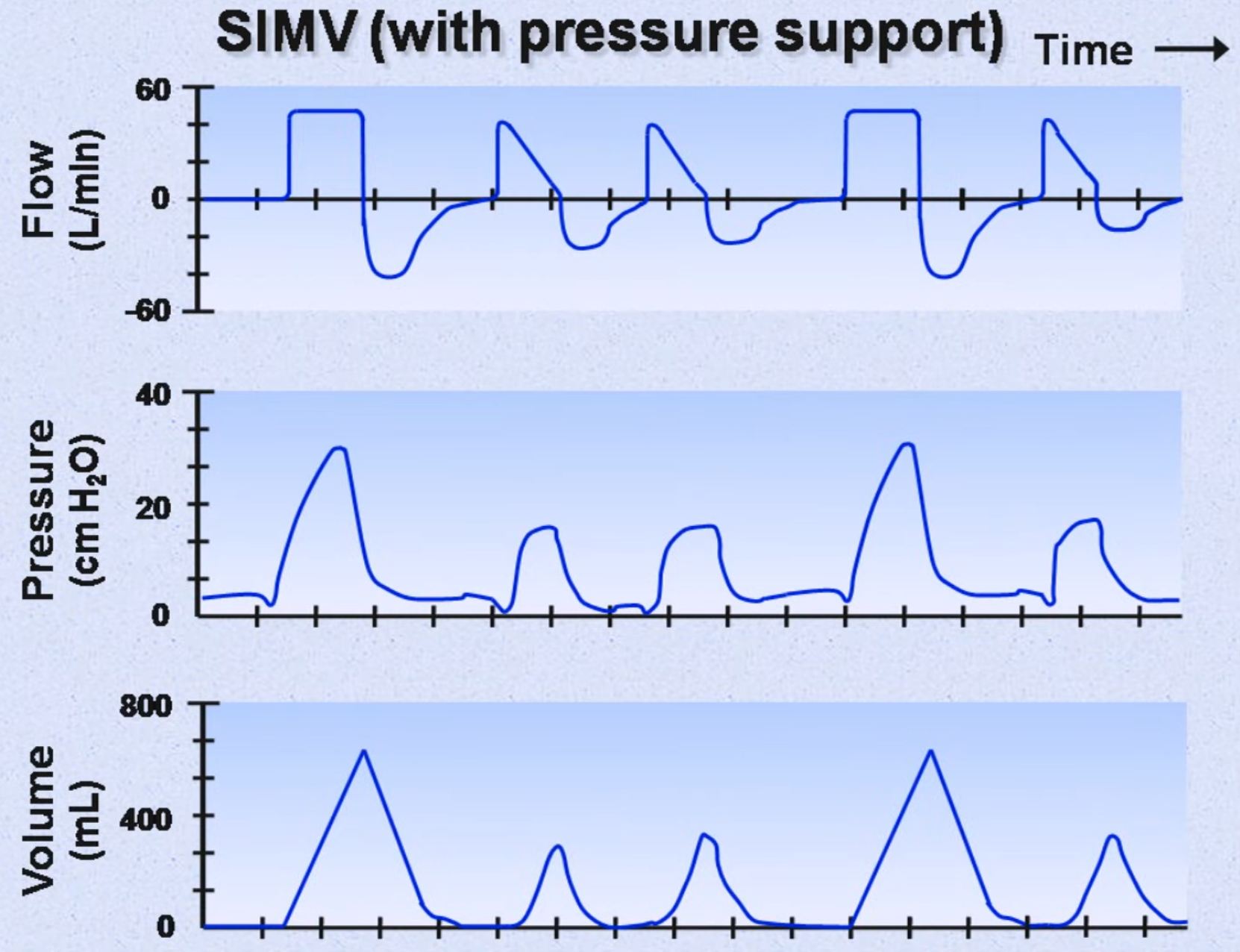
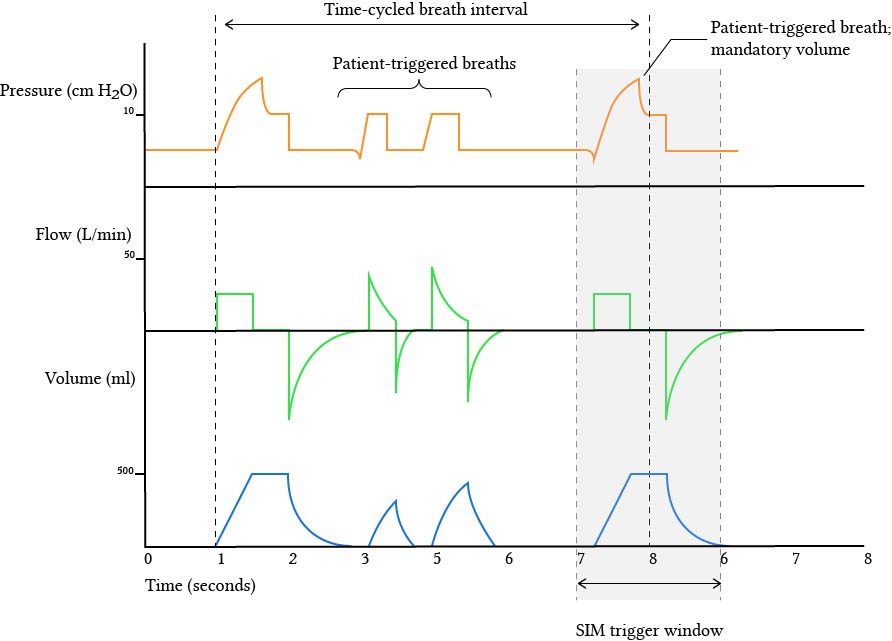
Synchronised Intermittent Mandatory Ventilation (SIMV)
- Main difference with IMV is that it is synchronised (as in the name); the patient can decide their own respiratory rate and they can take a number of pressure-supported breaths
- Among these breaths, the machine also gives a set number of mandatory breaths and if the patient makes an effort around the same time the next mandatory breath is due, the ventilator delivers to them an assist-control breath, with volume control
- Mix of mandatory breaths (some of which are synchronised with spontaneous breaths), and assisted breaths
- Mandatory (non-synchronised breaths):
- Trigger: time
- Control: volume
- Cycling: time or volume
- Synchronised breaths:
- Trigger: pressure or flow
- Control: volume
- Cycling: time or volume
- Non-synchronised breaths
- Trigger: pressure or flow
- Control: pressure
- Cycling: flow
- User sets a rate and volume
- There is a window of opportunity around each timed breath, during which a patient effort will be converted into a mandatory breath
- Advantage
- Guarantees a minimum minute ventilation
- Lower mean airway pressure when compared with AC
- Can provide a wide range of respiratory support
- Comfortable for the patient
- Disadvantages
- Increased work of breathing for patient
- ? Lower cardiac output in patients with LV dysfunction
- Limited control over the minute ventilation
- Indications
- Critically ill patients who are hyperventilating or otherwise prone to auto-PEEP or high airway resistance
NOTE
The main difference between SIMV and AC is that spontaneous breaths in excess of the set respiratory rate:
- In AC receive full support
- In SIMV receive partial support
Therefore in a patient with no spontaneous breaths AC = SIMV
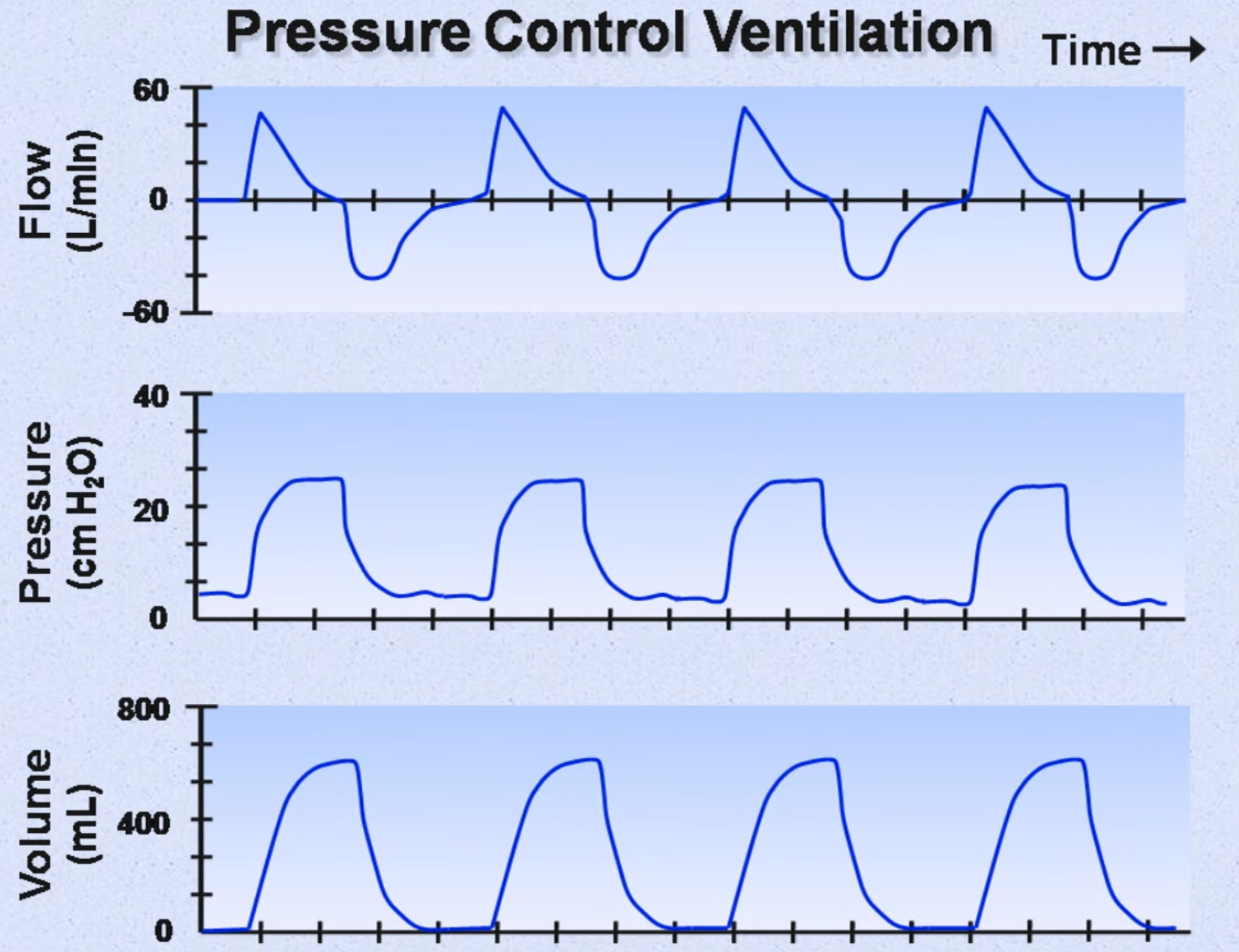
Pressure Control Ventilation (PCV)
- The main feature is that pressure is the control variable (CMV, IMV, SIMV, ACV can all be pressure controlled)
- Trigger: time (but typically flow triggered; the patient will become tachypnoeic if the is inadequate compensating for the low compliance)
- Control: pressure
- Cycling: time
- Indications
- Patients who are at a particularly high risk of barotrauma (i.e. those with low compliance)
- Little control over the minute volume
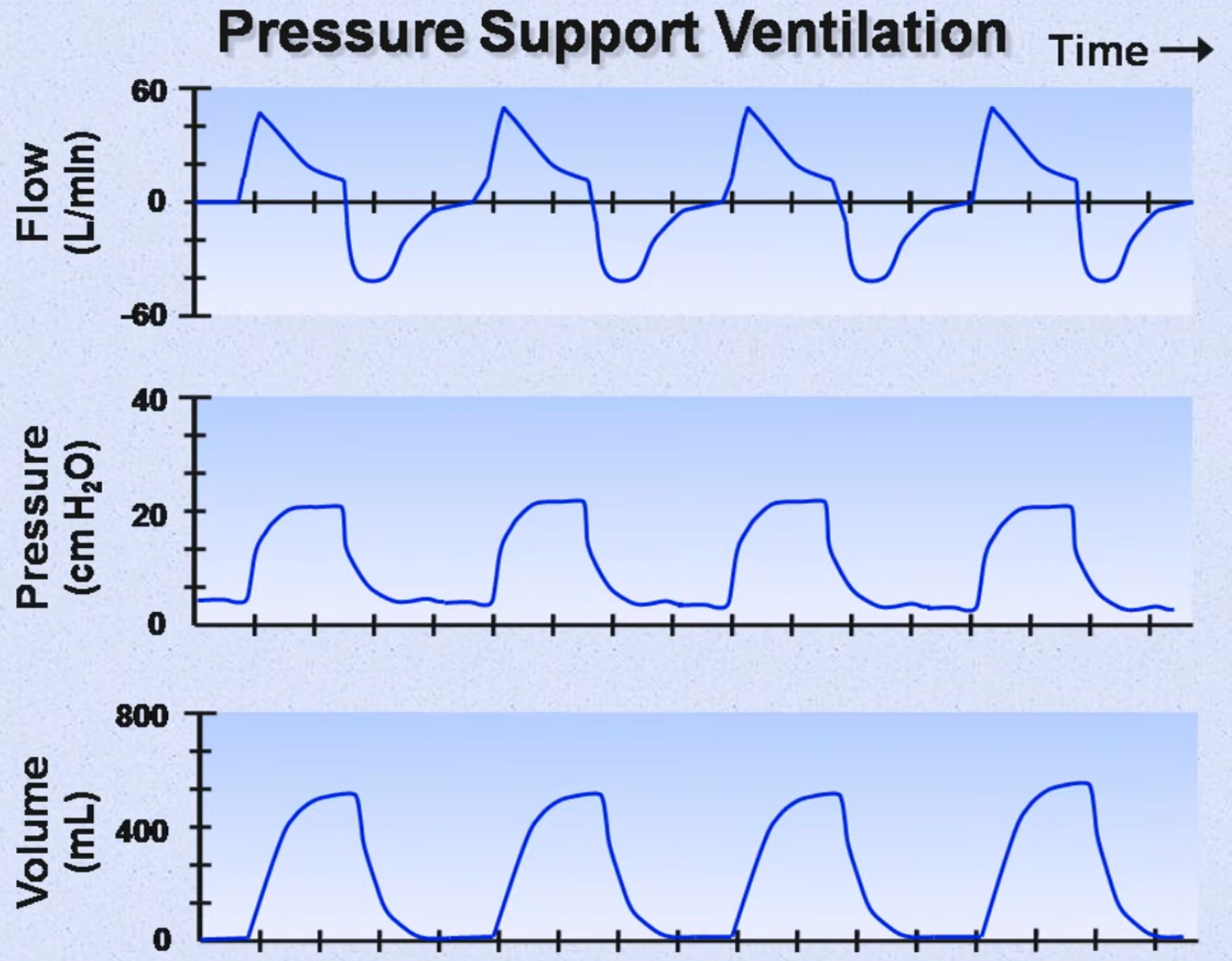
Pressure Support Ventilation (PSV)
- The ventilator only controls the pressure support level and the rate, volume, cycling time etc are controlled by the patient
- You can only control the the pressure support value (indirectly controlling the tidal volume) and the flow cycling trigger (decreasing it will make the breath last longer)
- There are no mandatory breaths; every breath must be triggered by the patient
- This mode is typically combined with SIMV as the non-mandatory component
- Trigger: Pressure or flow
- Control: Pressure
- Cycling: Flow
- Advantages:
- Probably the most comfortable mode for the awake, conscious patient
- Disadvantages:
- Patient must trigger each breath
- A minimum minute ventilation cannot be guaranteed
- Associated with poorer quality sleep
- Generally incapable of providing full ventilatory support
- Indications
- Conscious patient
- As a stepping stone immediately prior to extubation
Dual Control Modes
- Use instantaneous feedback to control aspects of lung volume and airway pressure simultaneously
- Examples include
- Pressure-regulated volume control
- Volume support
- Volume assured pressure support
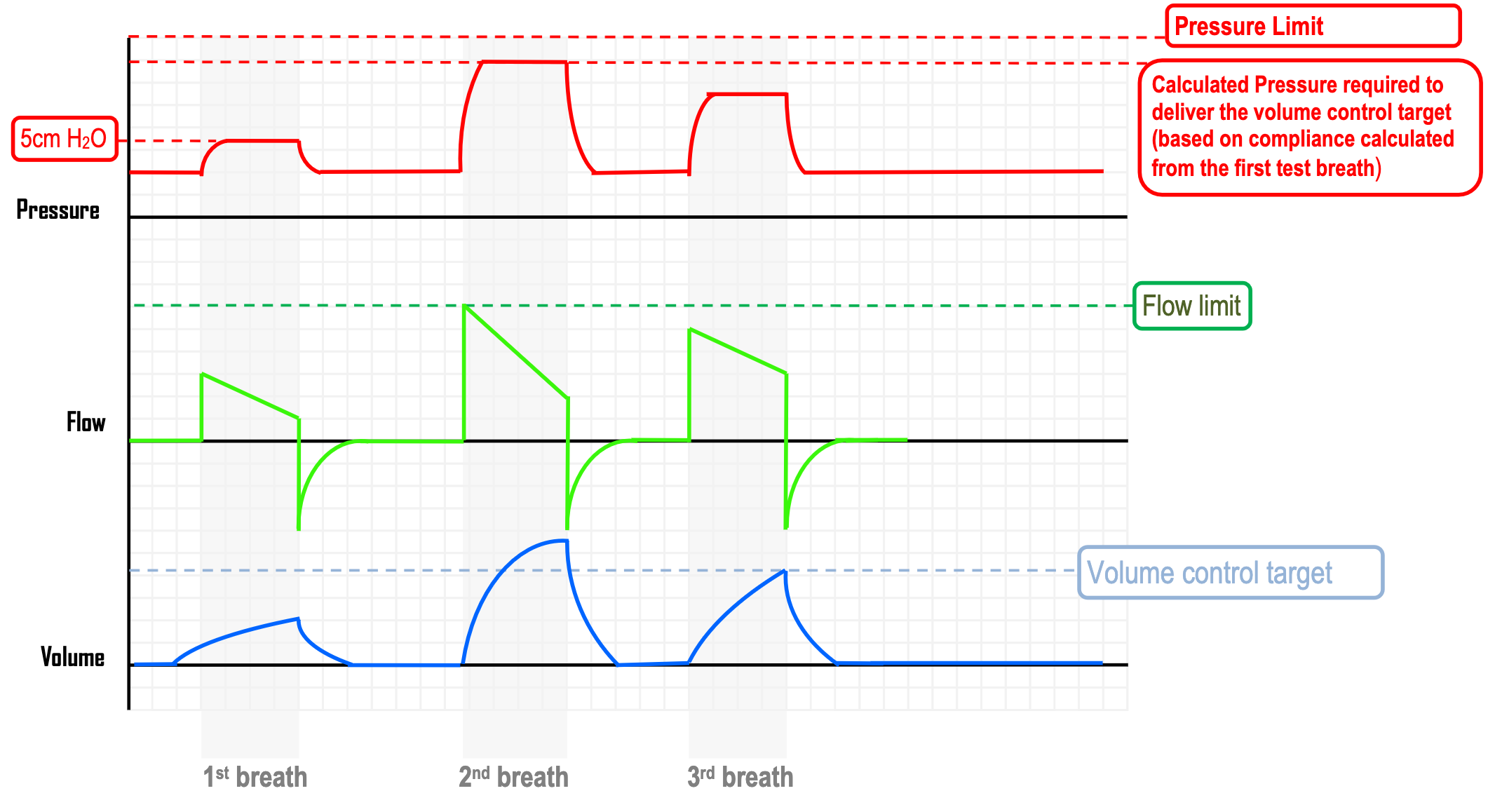
Pressure Regulated Volume Control (PRVC)
-
The user sets a target tidal volume (as in volume control modes)
-
The ventilator performs an assessment of the dynamic lung compliance over the course of three initial calibrating breaths
- First breath tests compliance and is typically a low volume low pressure calibration breath
- The next breath is delivered at a calculated pressure depending on the compliance from the previous breath; if the controlled target volume is exceeded, the ventilator adjusts the flow rate so that the next breath the pressure is slightly lower
-
Using this data, it then determines the appropriate pressure level required to achieve the prescribed tidal volume
-
The main feature is that the lowest possible pressure to achieve the volume control target is applied
-
Advantages and disadvantages are similar to SIMV with the added benefits from PCV
-
Advantages:
- Mean airway pressure is as high as with PCV
- Pressure is minimised for any given prescribed tidal volume
- A minimum minute volume is guaranteed, preserving a degree of control over PaCO2