Mechanical Ventilation
Quick reference: Mechanical Ventilation - Quick Reference
Sub-Notes
- I felt I had to split up this topic otherwise there would be too much to scroll through in one note
| Note | Contents |
|---|---|
| Physiology of Mechanical Ventilation | Lung mechanics, gas exchange, phases of MV, monitoring |
| Ventilator Modes | AC, SIMV, PCV, PSV, PRVC — trigger/control/cycle, pros/cons, indications |
| Ventilator Settings | Control variables, targeting schemes, phase variables, FiO₂, VT, RR, PEEP, PS, I:E ratio, initial settings |
| Ventilator Waveform Interpretation | Pressure and flow waveforms, P-V loops, work of breathing |
| Lung Protective Ventilation | VALI, barotrauma, biotrauma, ARDS protocol, permissive hypercapnoea |
| Ventilator Consequences | Effects on gas exchange, haemodynamics, ICP; auto-PEEP, dyssynchrony, VAP |
| Ventilatory Weaning | SBT readiness, passing/failing SBT, extubation checklist, post-extubation |
| Ventilator Troubleshooting and Alarms | Crashing patient, DOPES, COPD, all alarm types |
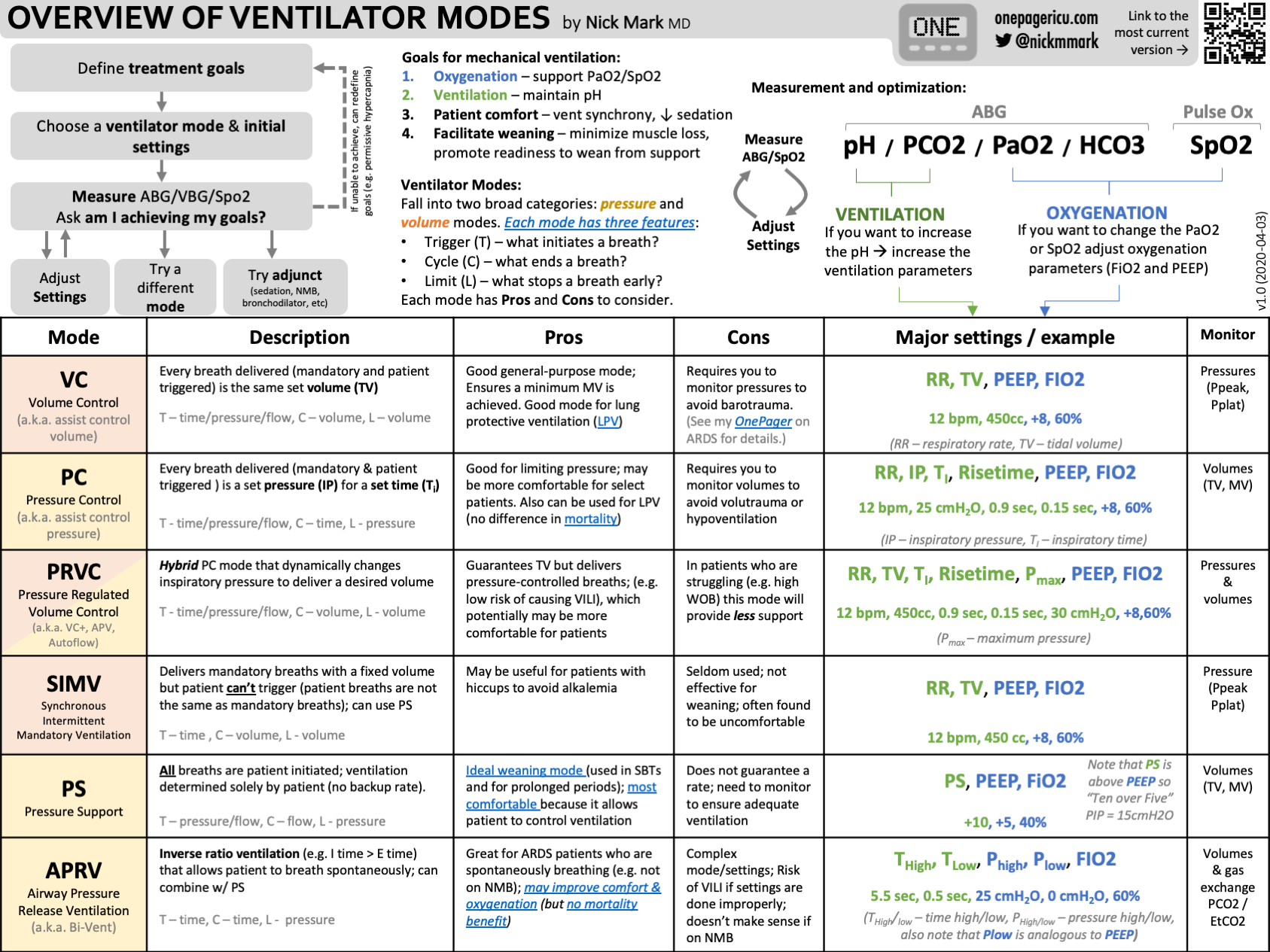
Ventilator Modes Overview
| Mode | Control | Trigger | Cycle | Key Use |
|---|---|---|---|---|
| AC | Volume | Time/P/Flow | Time | Full support, no hyperventilation |
| SIMV | Volume + Pressure | Time + P/Flow | Time + Flow | Hyperventilating patient, auto-PEEP risk |
| PCV | Pressure | Time only | Time | High barotrauma risk |
| PSV | Pressure | P/Flow | Flow | Conscious patient, pre-extubation |
| PRVC | Adaptive (P→V) | Time | Time | Guarantees VT, minimises P |
AC vs SIMV: excess spontaneous breaths get full support in AC, partial support in SIMV
Initial Settings at a Glance
| Parameter | Normal | COPD | ARDS |
|---|---|---|---|
| VT | 10 mL/kg IBW | 8 mL/kg IBW | 6 mL/kg IBW |
| RR | 10–20 | Avoid ↑ | 10–20 |
| FiO₂ | Start 100%, wean to ≤60% | ← | ← |
| PEEP | 5–8 cmH₂O | Low/ZEEP | ≥8–12 cmH₂O |
| I:E | 1:2 | 1:3 or 1:4 | 1:2 |
Pressure Interpretation
| Meaning | ||
|---|---|---|
| ↑ | Normal | ↑ Airway resistance (bronchospasm, secretions, kink) |
| ↑ | ↑ | ↓ Lung compliance (oedema, pneumothorax, ARDS) |
Delirium Prevention
- The FAVoR trial demonstrates a reduction in delirium for ventilated patients receiving scripted family-recorded voice message to re-orientate them
- There was only a 1.1% improvement in delirium free days, a low number of patients recruited to the trial, and although small the differences in baseline characteristics between the intervention & control groups may be significant given the small difference in outcome. I would therefore want to see further data before pushing for widespread adoption of this technique
- Delirium Reduction via Scripted Family Voice Recordings in Critically Ill Patients Receiving Mechanical Ventilation CL Munro. Am J Crit Care. 2025; Nov 1;34(6):429-437. doi: 10.4037/ajcc2025486
Sources
- Strong Medicine Playlist: Mechanical Ventilation - YouTube
- ICU One Pager
- Deranged Physiology
- Flow, volume, pressure, resistance and compliance
- Phases of a mechanical breath
- Basics of Mechanical Ventilation
- Phase variables: triggering, limits, cycling and PEEP
- Control variables: volume and pressure
- Triggering of a mechanically supported breath
- Limit (target) variables in mechanical ventilation
- Selecting and adjusting PEEP
- Inspiratory pause, I:E ratio and inspiratory rise time
- Practical differences between pressure and volume controlled ventilation
- Mandatory and spontaneous modes of ventilation
- Ventilator Alarm (DOPES) - YouTube
- EMCrit 239 - Vent Alarms = Code Blue
- Ventilator Alarms: Types, Causes, and Troubleshooting (2026)
- Liberation from the ventilator - EMCrit Project