Part of: Mechanical Ventilation
- Mode
- Fraction of inspired oxygen
- Tidal volume ()
- Respiratory rate (RR)
- Positive End-Expiratory Pressure (PEEP)
- Pressure Support (PS)
- Flow shape/contour
- Inspiratory:Expiratory (I:E) ratio
Control Variables
- The variable which the ventilator uses as feedback signal for controlling inspiration
- Flow cannot be a control variable because flow is a volume over time and thus when volume is controlled, flow is controlled indirectly
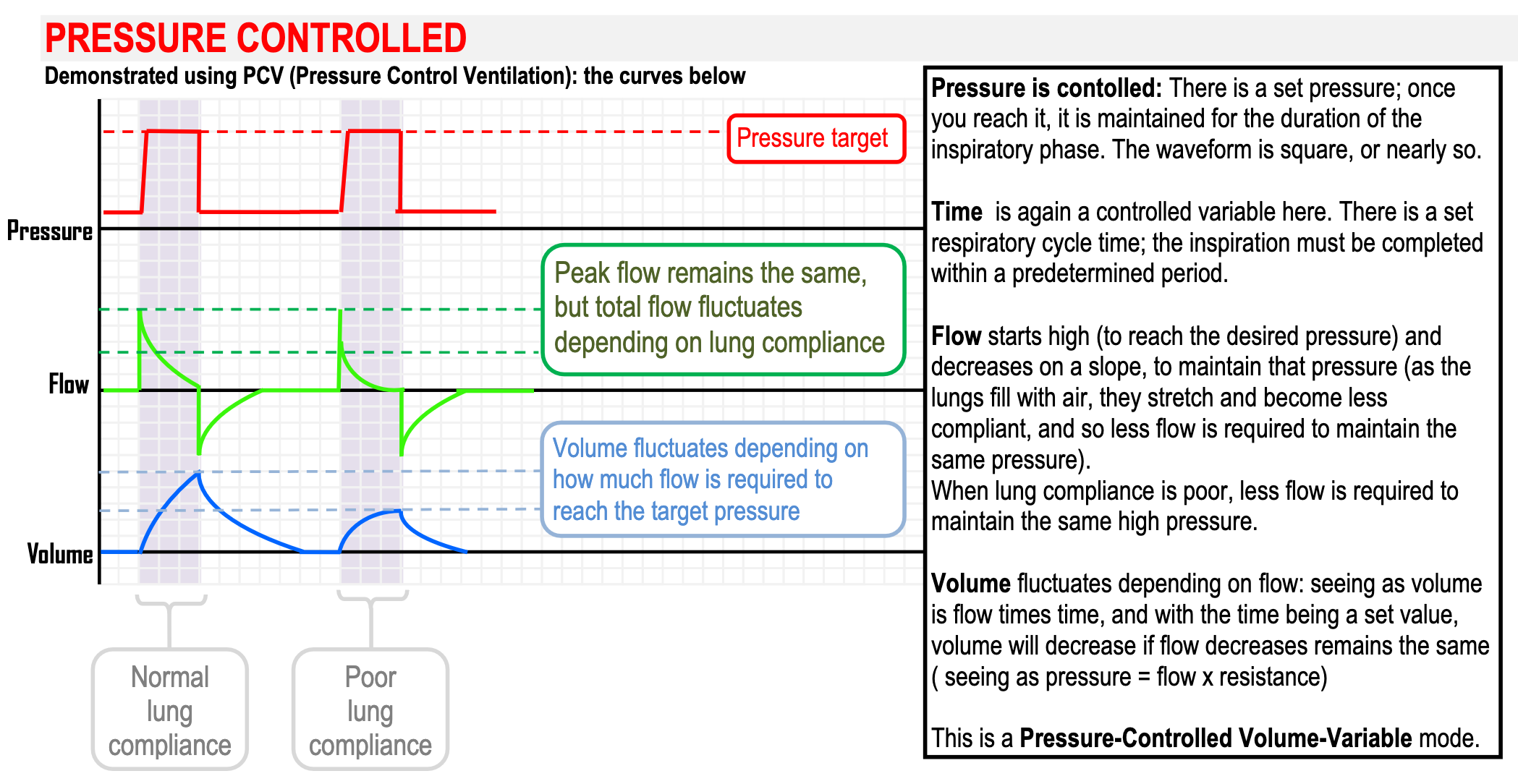
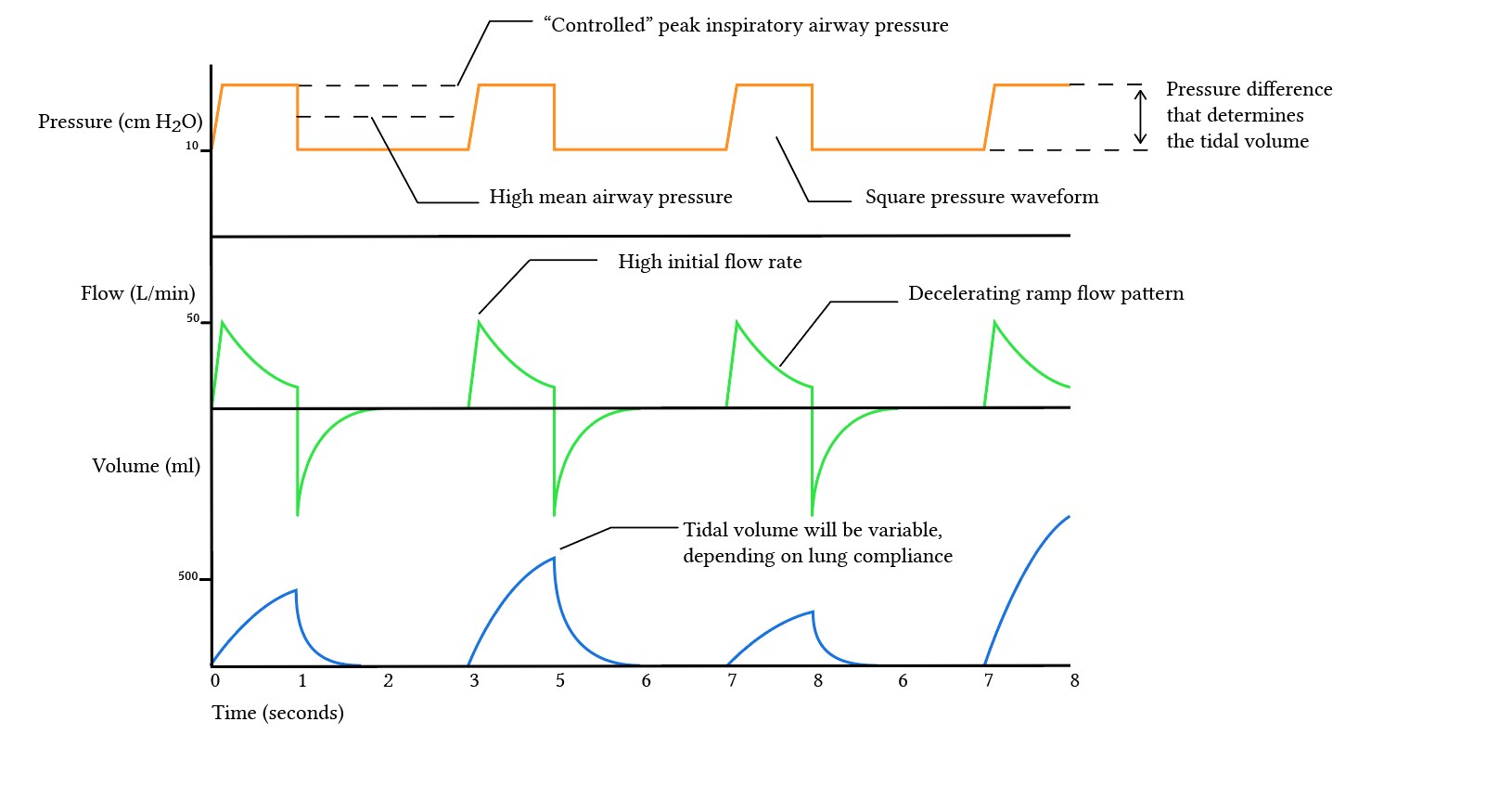
- Pressure control maintains a stable pressure in the face of fluctuating respiratory performance, which prevents lung injury from excess pressure but doesn’t give a consistent minute ventilation
- Advantages
- Increased mean airway pressure ⇒ improves oxygenation
- Increased duration of alveolar recruitment ⇒ square pressure waveform causes alveoli to open earlier and remain open for longer allowing for better gas exchange
- Prevents excessive airway pressures thereby protecting against barotrauma
- Avoids regional alveolar overdistention
- May lead to earlier liberation from mechanical ventilation
- Allows for significant air leak (e.g. during bronchoscopy or bronchopleural fistula)
- Disadvantages
- Tidal volume is variable and dependent on respiratory compliance
- Uncontrolled volume may result in “volutrauma” (overdistension)
- A high early inspiratory flow may breach the pressure limit if airway resistance is high
- Advantages
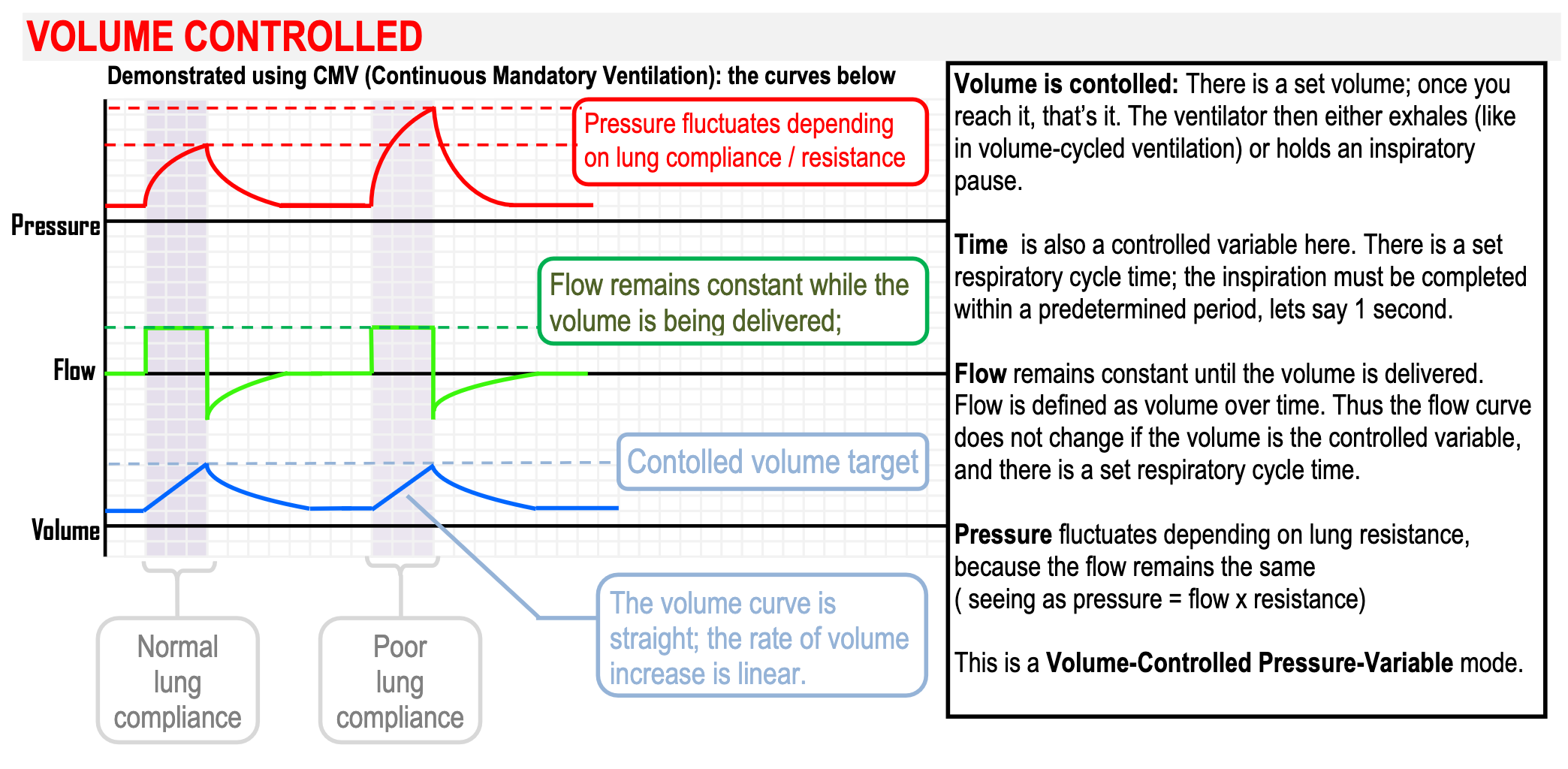
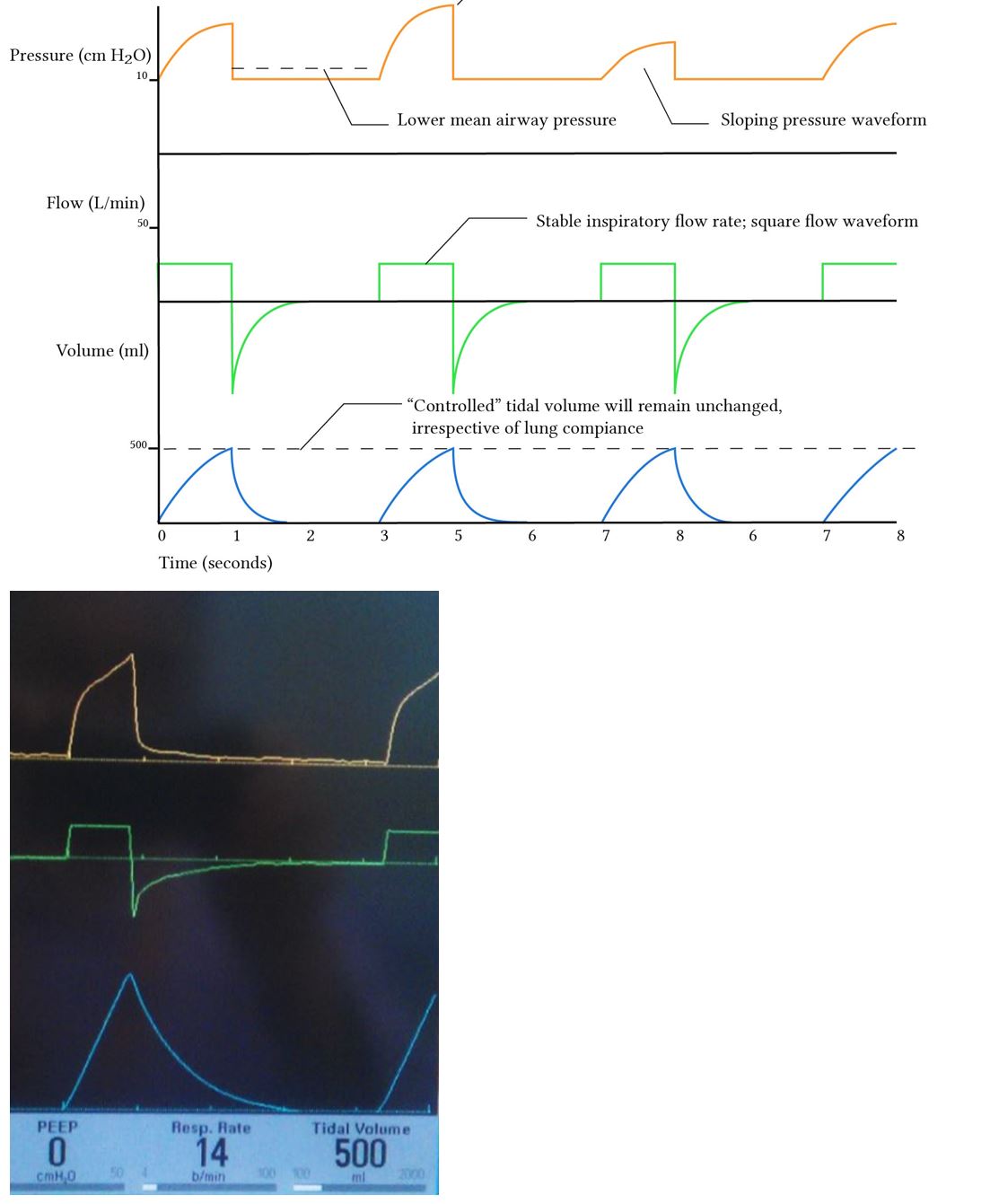
- Volume control gives a more stable minute ventilation, keeping at the desired level
- Advantages:
- Guaranteed tidal volumes produces a more stable minute volume
- The minute volume remains stable over a range of changing pulmonary characteristics
- The initial flow rate is lower than in pressure-controlled modes, avoiding a high resistance-related early pressure peak
- Disadvantages:
- The mean airway pressure is lower with volume control ventilation
- Recruitment may be poorer in lung units with poor compliance
- In the presence of a leak, the mean airway pressure may be unstable
- Insufficient flow may give rise to patient-ventilator dyssynchrony
- Advantages:
Targeting Scheme
- Set point: the ventilator will try to achieve the parameter (control variable chosen)
- Dual targeting: the ventilator switches from targeting one control variable to another in the middle of the breath
- For example a breath may start with a pressure control variable using a decelerating flow waveform, then reach the pressure limit mid breath and change to volume control until the target volume is reached
- Adaptive targeting:
- For example in PRVC, the inspiratory pressure is automatically adjusted to achieve an average tidal volume target; this varies from breath to breath adapting to the changing compliance (guarantees a prescribed volume while maintaining a square pressure waveform)
Phase Variables
Trigger Variable
- Determines when a breath is delivered, distinguishing ‘mandatory’ and ‘spontaneous’ modes of ventilation
- Sensitivity affects:
- Work of breathing
- Patient-ventilator synchrony
Time Triggered
- Mandatory ventilation
- Guarantees a minute volume offering predictable removal and decreased work of breathing
- Less comfortable and sedation requirements are higher
Flow Triggered
- Patient effort changes circuit flow
- Most comfortable but can be over-sensitive leading to dyssynchrony
- Ventilation is triggered when flow is diverted to the patient when the patient begins inspiration
- The exact threshold value can be altered but is generally 1-2 L/min1
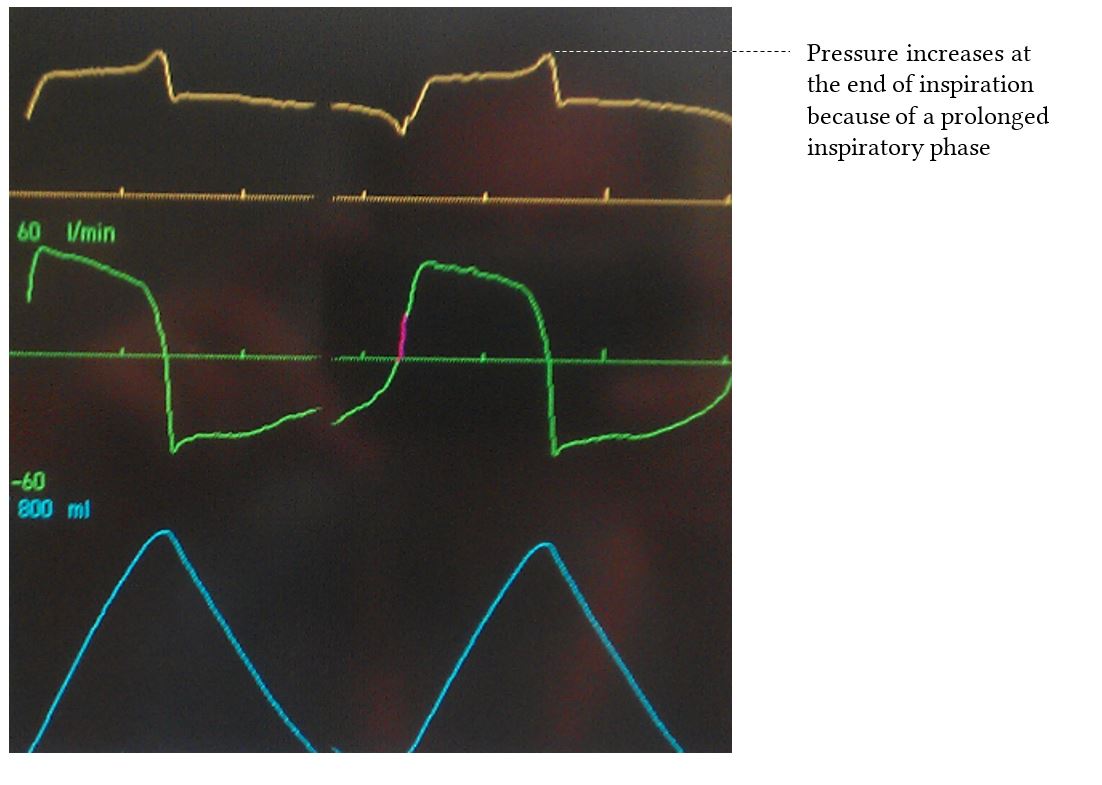
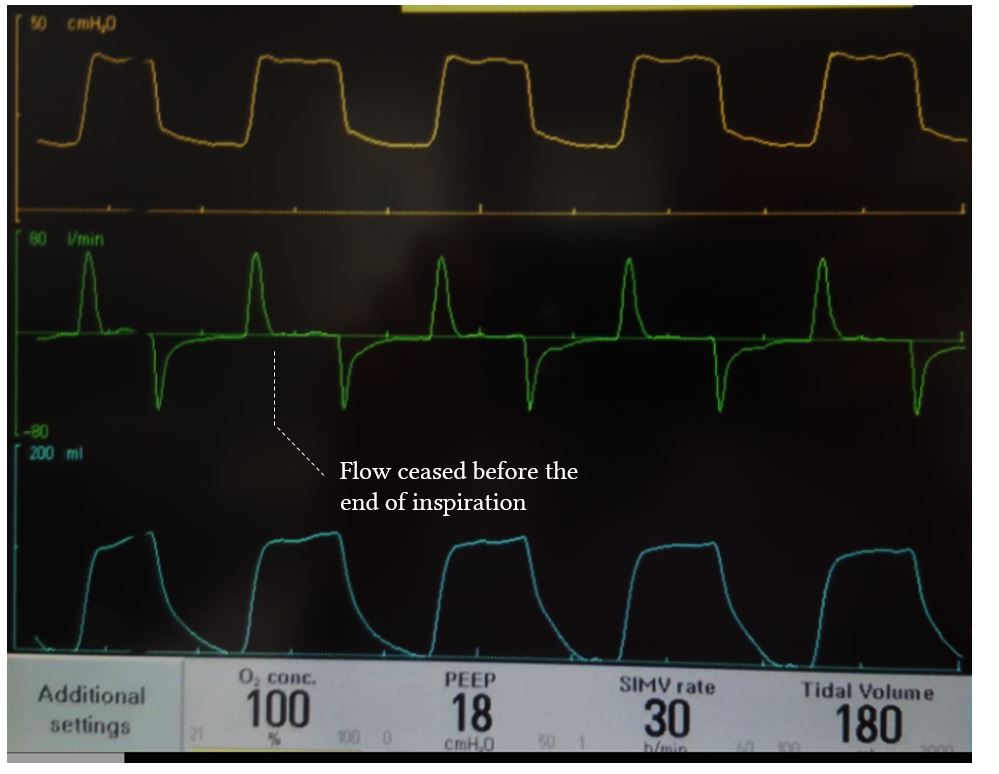
- Some machines indicate spontaneous respiratory effort by colouring the waveform
.jpg)
- Advantages:
- Generally quite sensitive meaning that patient’s work of breathing is not wasted on triggering the ventilator
- Allows the patient to have control over their minute volume
- May decrease the work of breathing
- More comfortable
- Permits a lower level of sedation
- Disadvantages:
- May be too sensitive, giving rise to auto-triggering (this is probably the only use case for pressure trigger)
- Does not guarantee a minute volume — therefore unsuitable for patients with a diminished or unreliable respiratory drive
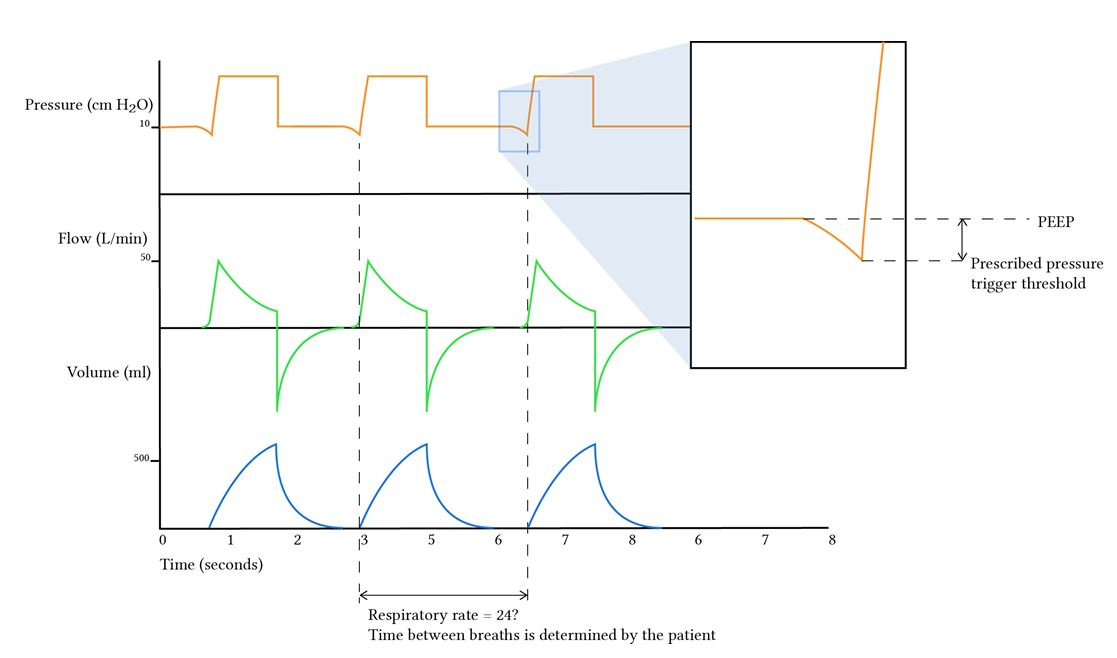
Pressure Triggered
- Patient generates negative pressure
- A typical pressure trigger threshold would be 1 cm
- Disadvantages
- Requires more effort to trigger the ventilator
- Represents a wasted respiratory effort
- Less comfortable for the patient
- Use cases
- Can be used to decrease auto-triggering (e.g. circuit leak, bronchopleural fistula or hyperdynamic circulation)
- Can be used to test the power of respiratory musculature in the context of an assessment of readiness for extubation (e.g. a patient who is able to trigger the ventilator by generating a negative intrathoracic pressure of -20 cm is unlikely to fail extubation due to weakness of their respiratory muscles)
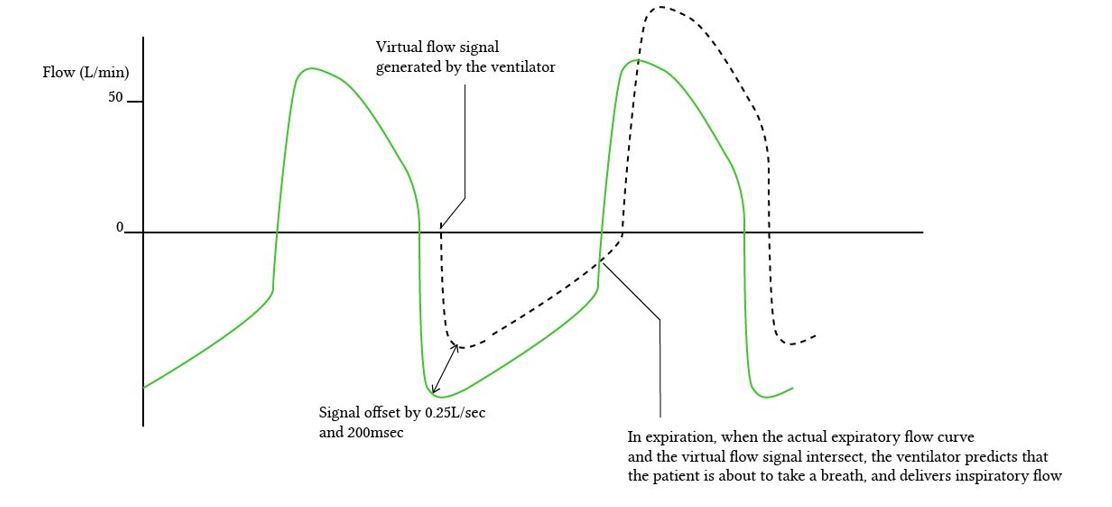
Shape-Signal Triggering
- May decrease wasted effort by “predicting” the next respiratory effort but not widely available
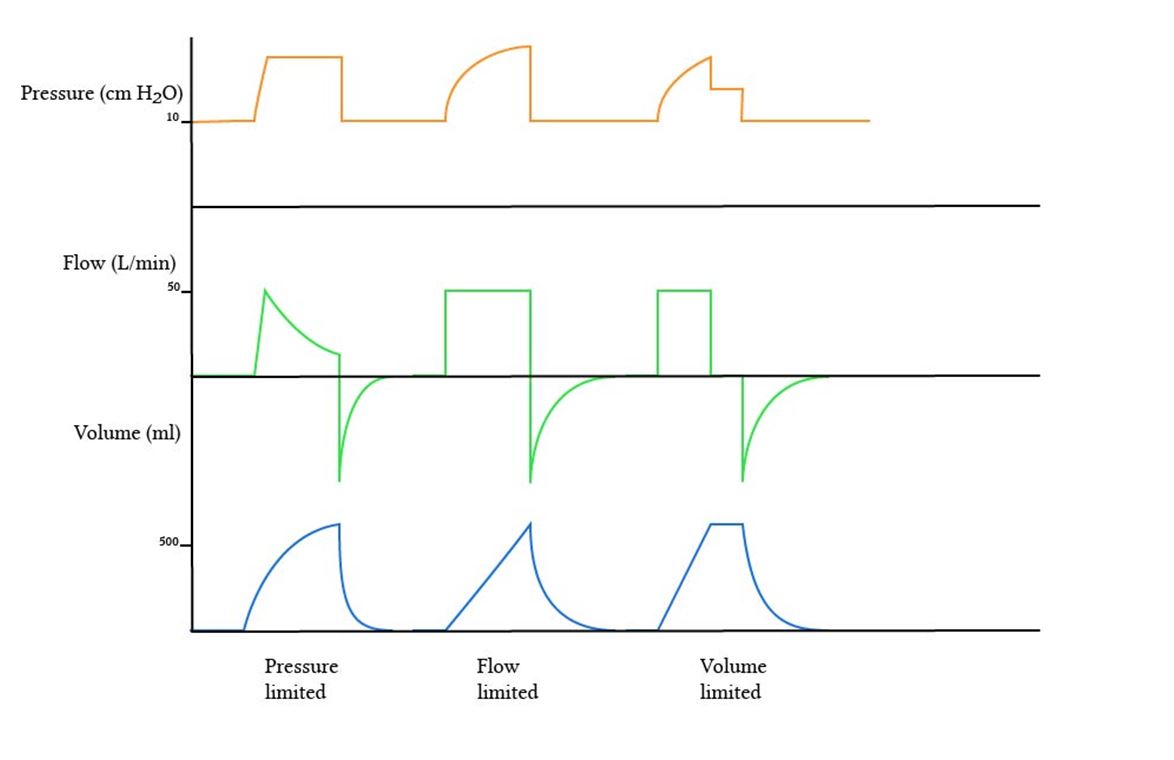
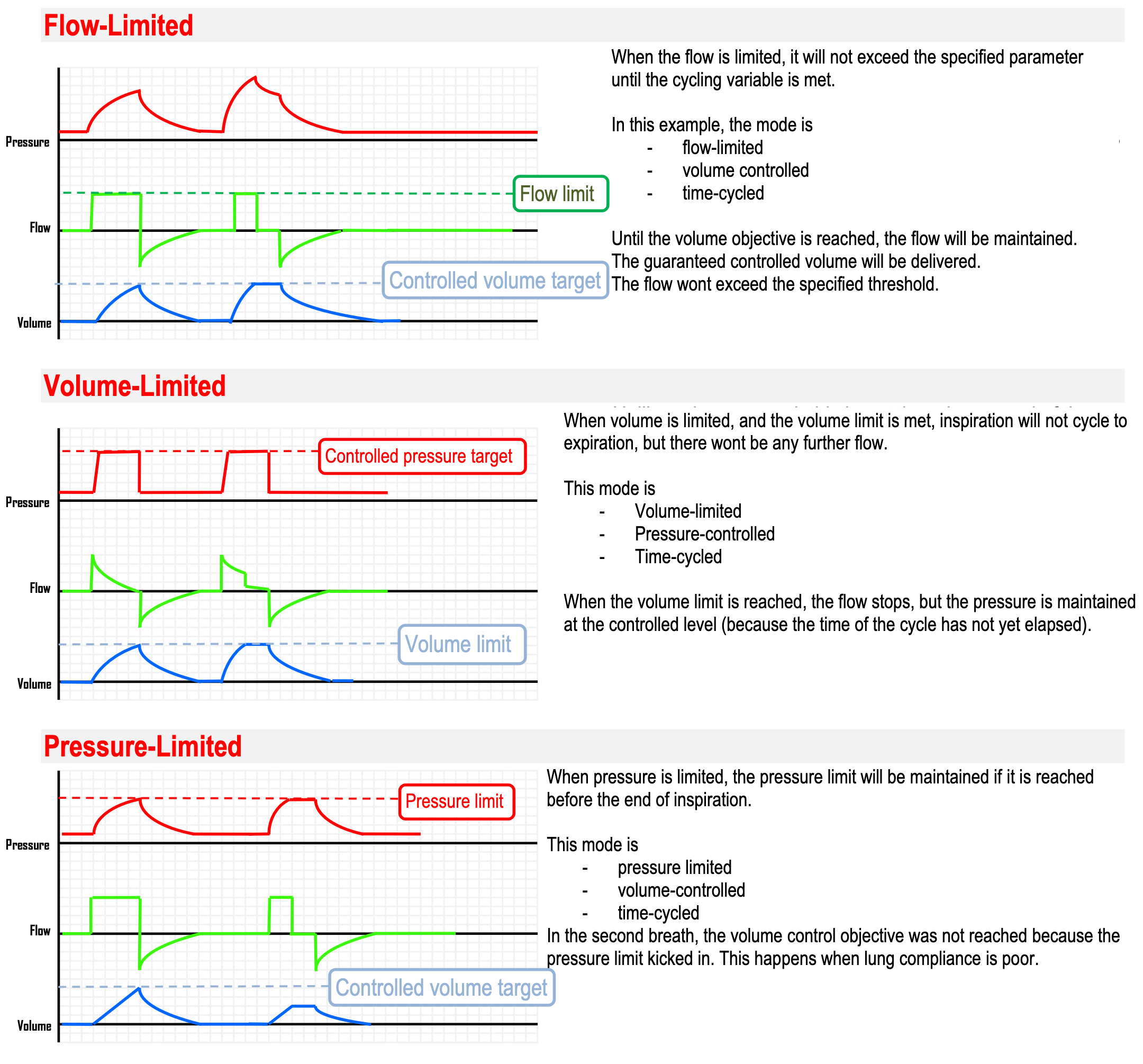
Limit/Target Variable
- Refers to the maximum value a variable can reach during inspiration but importantly, it does not end inspiration
- Common limit variables include pressure, flow and volume
- For example, continue holding this pressure or flow value (don’t exceed it) during the rest of inspiration
Cycling Variable
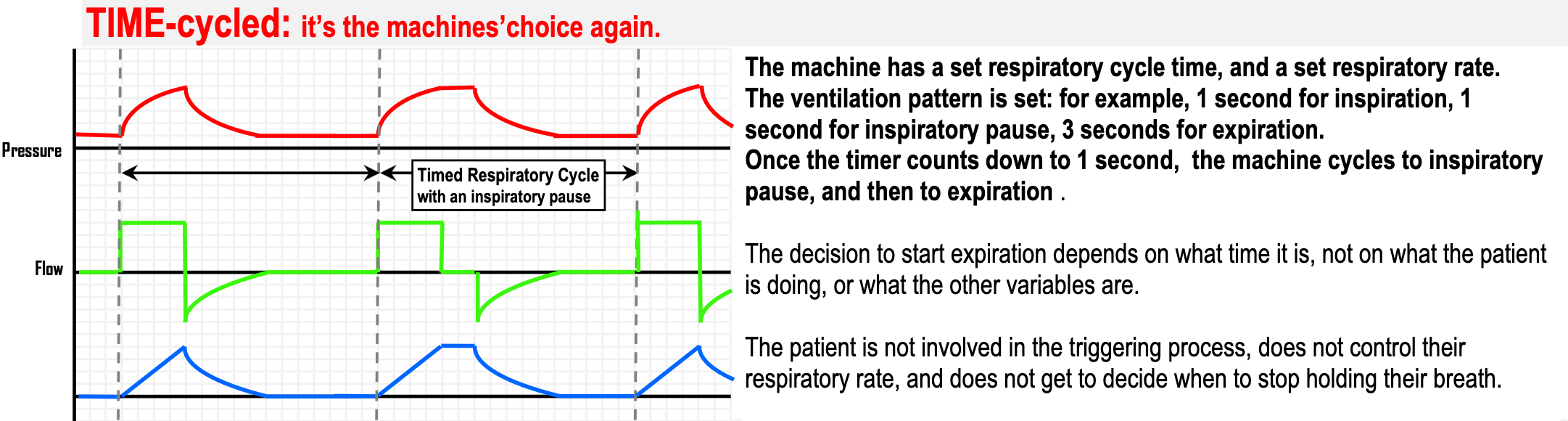
Time-Cycled
- Feature of mandatory modes
- Usually set by setting a respiratory rate and the I:E ratio
- Advantages:
- Careful control of minute volume, with obvious advantages for scenarios where tight PaCO2 control is desirable (e.g. traumatic brain injury)
- Ventilation is unaffected by changes in lung compliance or airway resistance because the timing of the breath is unrelated to any respiratory system parameters
- Minute ventilation is not affected by an unreliable respiratory drive, making this method suitable for paralysed or deeply unconscious patients
- Disadvantages:
- Unsuitable for lightly sedated and awake patients
- May result in patient-ventilator dyssynchrony particularly if the patient tries to exhale before the cycle time runs out
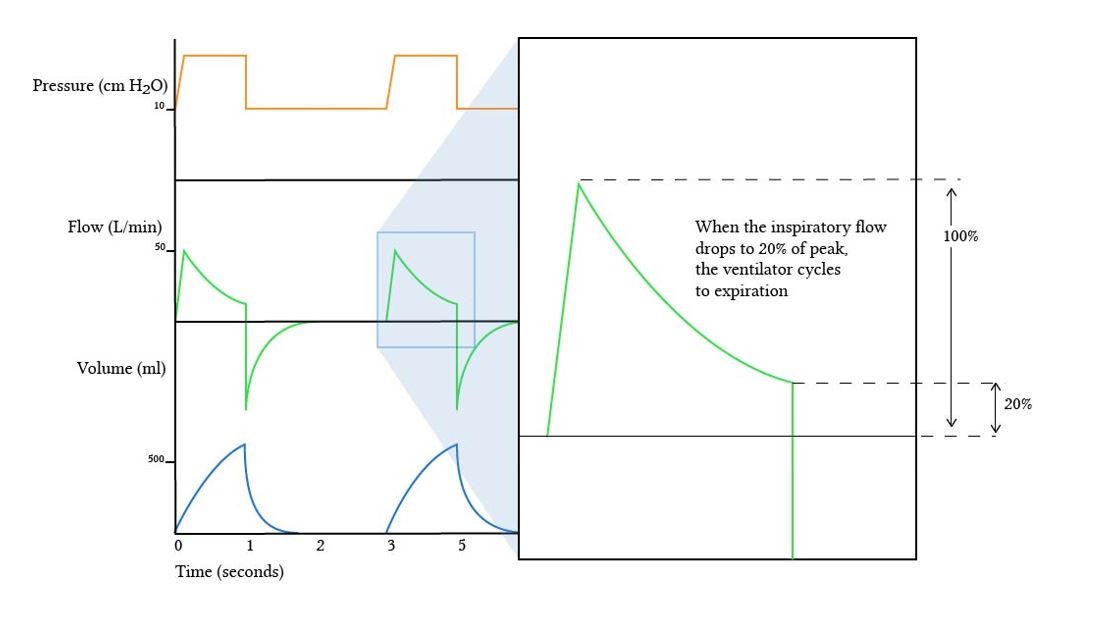
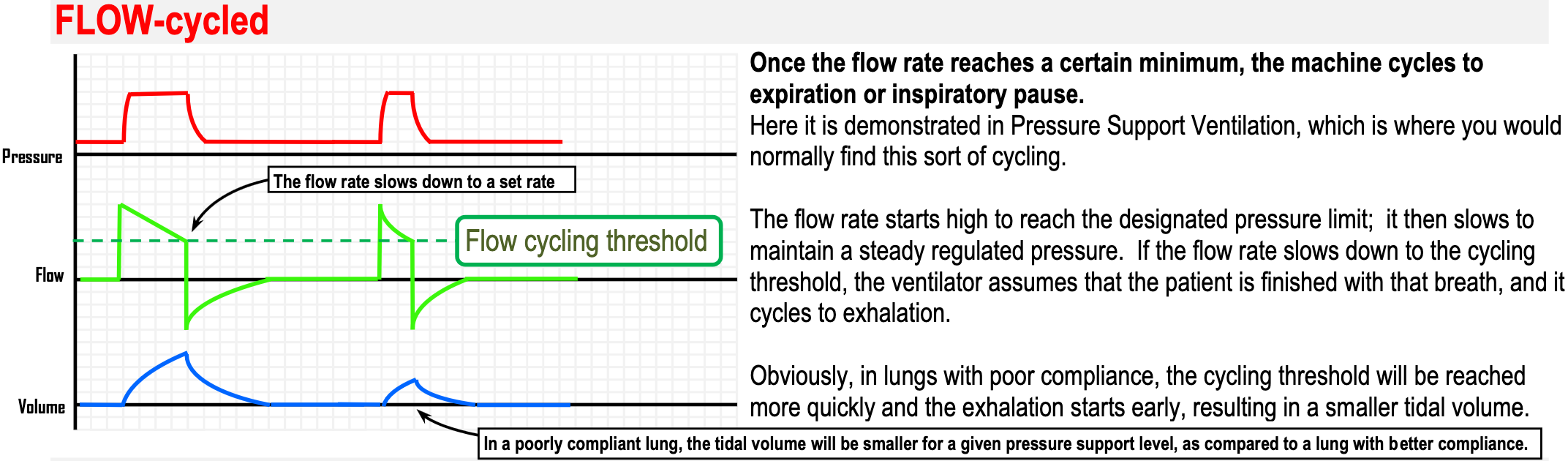
Flow Cycled
- The ventilator cycles into the expiratory phase once the flow has decreased to a predetermined value during inspiration
- Can be expressed as a fixed value in litres per minute or a percentage fraction of the peak flow rate
- In patients with restrictive lung disease (poor compliance), flow rate drops quickly → lower tidal volumes
- In patients with emphysema (high compliance), flow rate drops slowly → higher tidal volumes
- Advantages:
- More comfortable for the patient
- Limited by changes in lung compliance and airway resistance, preventing inadvertent ventilator-induced lung injury
- Disadvantages
- Tidal volumes may be poor in patients with poor lung compliance, resulting in inadequate minute volume
- Patient comfort depends on intelligent settings; inappropriately low or high settings could result in uncomfortably deep inspiration or “double triggering”
Pressure Cycled
- Largely obsolete in the modern era
- Advantages: Safety from pressure-related lung injury; decelerating ramp flow pattern; compliance determines cycling
- Disadvantages: Volume is determined by compliance; respiratory rate may fluctuate; may increase respiratory effort; pressure cannot also be a control variable
Volume Cycled
- Largely obsolete in the modern era
- Inspiratory phase ends when the specified volume has been delivered
- Major disadvantage: propensity to generate high peak airway pressures when lung compliance decreases
Fraction of Inspired Oxygen
- should be titrated to the lowest value which still maintains adequate oxygenation
- In common practice, set at 100% after the patient is first intubated, then titrated downward over one to several hours as indicated by pulse oximetry and/or serial ABGs
- leads to oxygen toxicity; if adequate oxygenation requires , additional strategies are required:
- ↑ PEEP
- Recruitment manoeuvres
- Trial of a different mode
Tidal Volume
- The tidal volume is 7 mL/kg in a normally breathing patient
- Most applicable to volume cycled modes (AC, SIMV)
- Initial values should be weight based:
| Patient | |
|---|---|
| Healthy lungs (e.g. neurological catastrophe, drug overdose) | 10 mL/kg IBW |
| COPD | 8 mL/kg IBW |
| ARDS | 6 mL/kg IBW |
- Higher leads to ↓ , ↑ pH and ↑ and vice versa
Respiratory Rate
- Typical respiratory rate is 10-20 breaths/min in order to provide 7-10 L/min of minute ventilation
- The normal resting minute volume is 70-100 mL/kg/min; therefore to produce tidal volumes of 6-8 mL/kg, a respiratory rate of between 12-16 breaths per minute
- Higher RR leads to ↓ , ↑ pH and higher risk of auto-PEEP and vice versa
Positive End-Expiratory Pressure
- Continuous positive pressure present throughout all of ventilation
- Physiologic effects:
- ↑ oxygenation
- ↑ alveolar recruitment
- ↑ alveolar surface area
- ↑ cardiac output in CHF patients but can ↓ BP in non-CHF patients
- ↓ preload
- ↓ LV afterload
- ↑ RV afterload → ↑ R-L shunts if present
- ↑ oxygenation
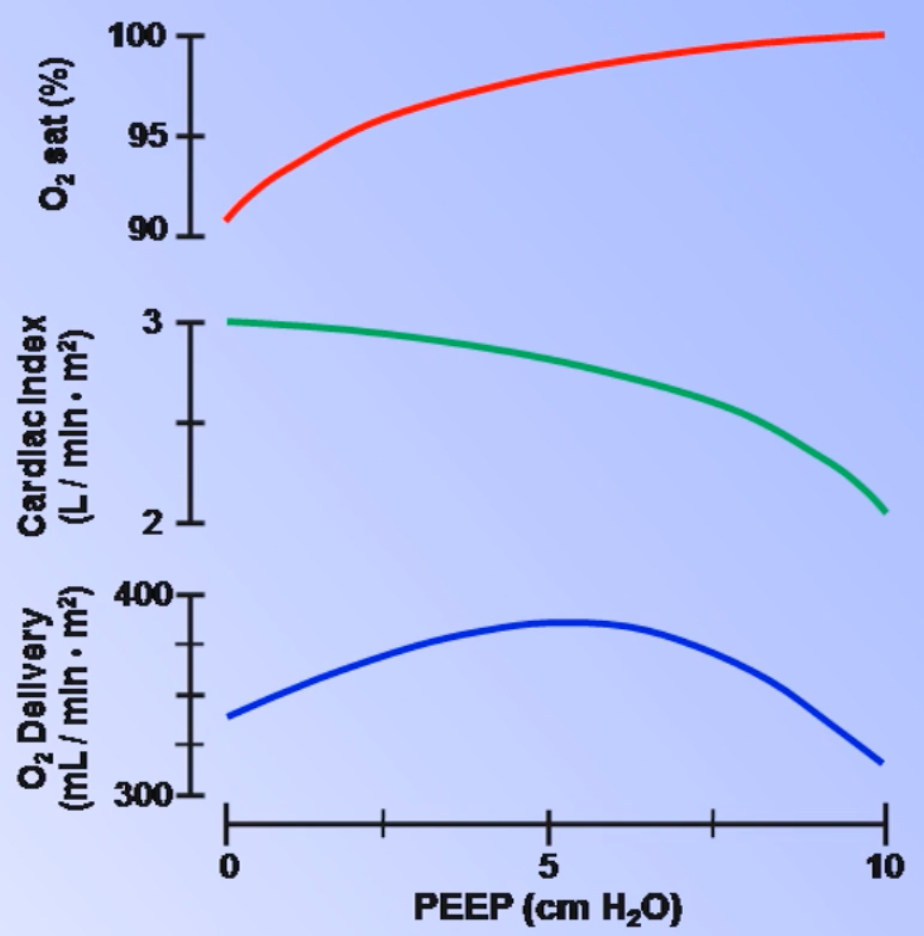
- In clinical practice: PEEP is set to the lowest value that allows to be ≤ 60% with a minimum value of 5 cm of
- The healthy lung should be ventilated with 5-8 cm of of PEEP
- ARDS patients will require higher PEEP (usually > 12 cm of )
- With bronchospasm, low PEEP or zero PEEP (ZEEP) is often warranted (< 5 cm of )
Pressure Support
- Amount of additional positive pressure beyond PEEP that is provided during inspiration. Important in PSV, BiPAP and almost always used in SIMV
- Simple estimate of optimal PS is:
- However in practice, PS is typically set to twice PEEP
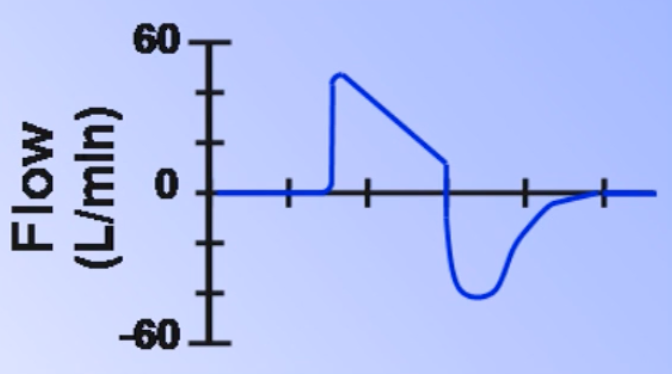
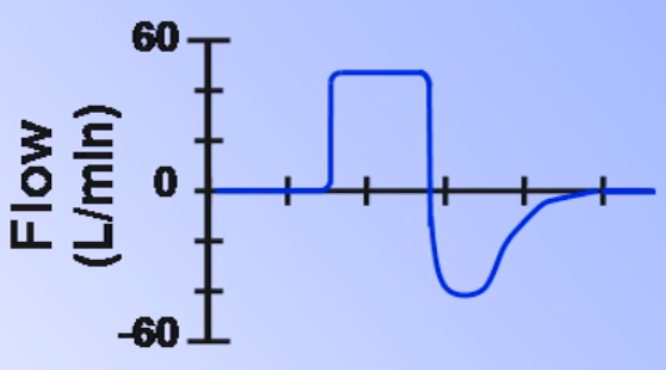
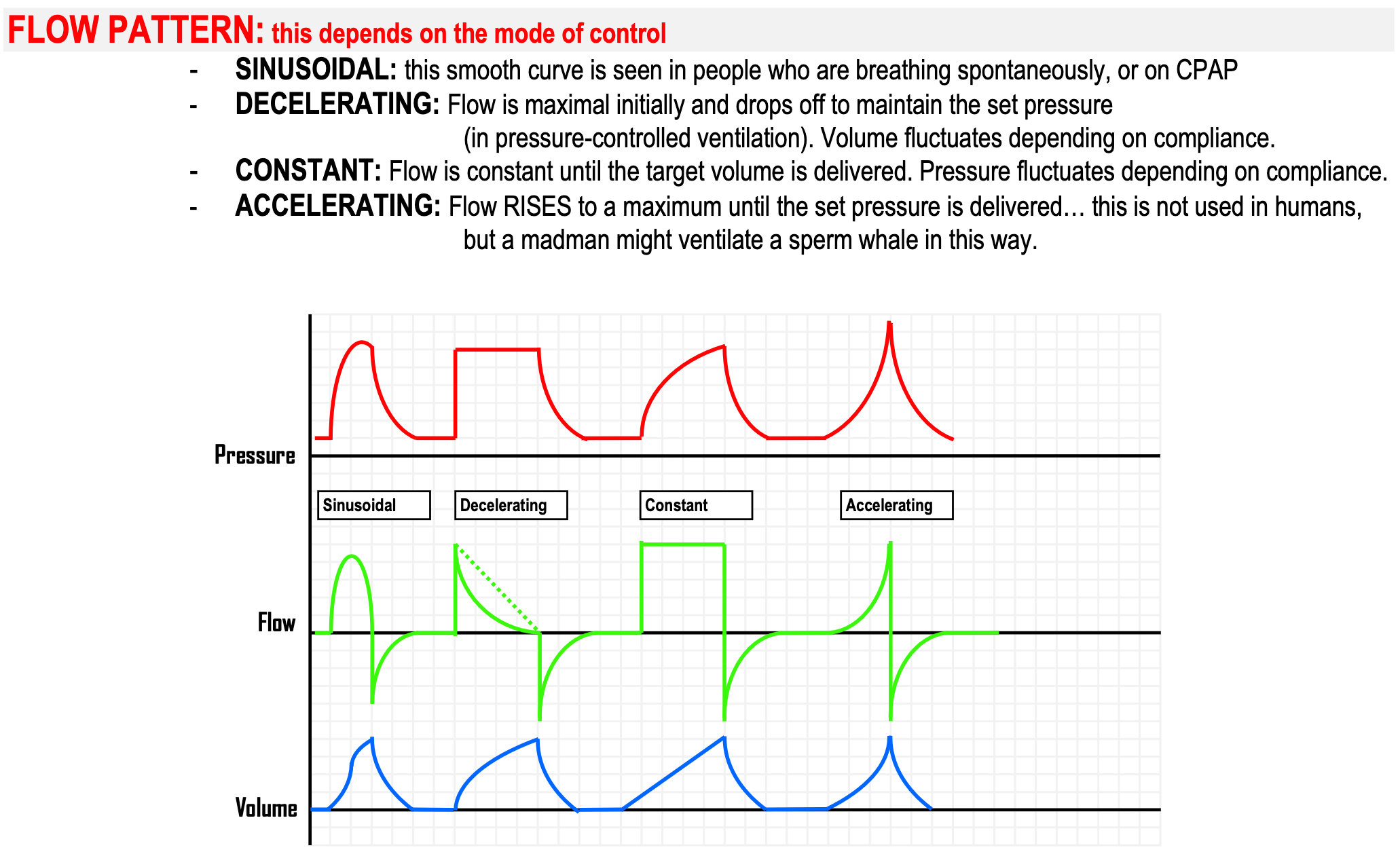
Flow Shape/Contour
- Describes the pattern of airflow during inspiration; set in volume-targeted ventilator modes
- Always decelerating shape in pressure-targeted modes as a consequence of lung mechanics
| Contour | Dead space () | Auto-PEEP | ||
|---|---|---|---|---|
| Decelerating | ↓ | ↑ | ↓ | More |
| Constant | ↑ | ↓ | ↑ | Less |
 |
Inspiratory : Expiratory Ratio
- Ratio between the amount of time spent in inspiration and expiration
- Normal I:E ratio is 1:2; deviations from this are uncomfortable, often requiring deep sedation
| Change | Effects |
|---|---|
| ↑ Inspiratory time | ↑ Mean airway pressure → better oxygenation (but ↓ CO₂ clearance, ↑ haemodynamic instability, ↑ gas trapping) |
| ↑ Expiratory time | ↑ CO₂ clearance → better ventilation (but ↑ probability of atelectasis) |
- In AC and SIMV: usually set indirectly via and flow rate/pattern
- In PCV: usually set directly
- In PSV: generally outside of clinician control
- A higher ratio (higher inspiratory time) results in ↑ and higher risk of auto-PEEP and vice versa
Typical Initial Ventilator Settings
| Option | Typical Settings |
|---|---|
| Mode | Intrinsic hyperventilation → SIMV; No intrinsic hyperventilation → AC or SIMV |
| FiO₂ | Start at 100%; Taper as able to 35–60% to keep >60–80 mmHg |
| Tidal Volume () | ~10 cc/kg normal; ~8 cc/kg COPD; ~6 cc/kg ARDS (Use IBW); Lower if > 30 cm |
| Rate | 10–20 breaths/min to achieve MV of 7–10 L/min; adjust based on pH |
| PEEP | Start at 5 cm ; Titrate up if <60 on >60% FiO₂; May start with no PEEP in pure hypoventilation |
| Pressure Support (n/a for AC) | 5–20 cm ; Optimal ; (Minimum 5 cm PS always to overcome ETT resistance) |
Typical Initial Ventilator Alarm Settings
- High pressure limit: 10–15 cm H₂O above PIP
- Low pressure limit: 5–10 cm H₂O below PIP
- Low PEEP limit: 3–5 cm H₂O below set PEEP
- Low exhaled tidal volume: 100 mL or 50% below set VT
- Low minute ventilation: 2–5 L/min or 50% below baseline
- High minute ventilation: 50% above baseline
- FiO₂ alarm: ±5% from set oxygen concentration
- Temperature alarm: ±2°C from set temperature
- Apnea delay: About 20 seconds
Footnotes
-
Normal mean inspiratory flow rate at rest is around 15 L/min with a peak of around 30-35 L/min ↩