Part of: Mechanical Ventilation
Lung Mechanics
Definitions
- Where:
- is the minute ventilation
- is the tidal volume
- Where:
- is the alveolar ventilation
- is the physiologic dead space
- Where
- is airflow
- is pressure gradient
- is airway resistance
- Where
- Resistive pressure is the pressure required to push airflow through the airways
- Elastic pressure is the pressure required to inflate lungs and chest wall
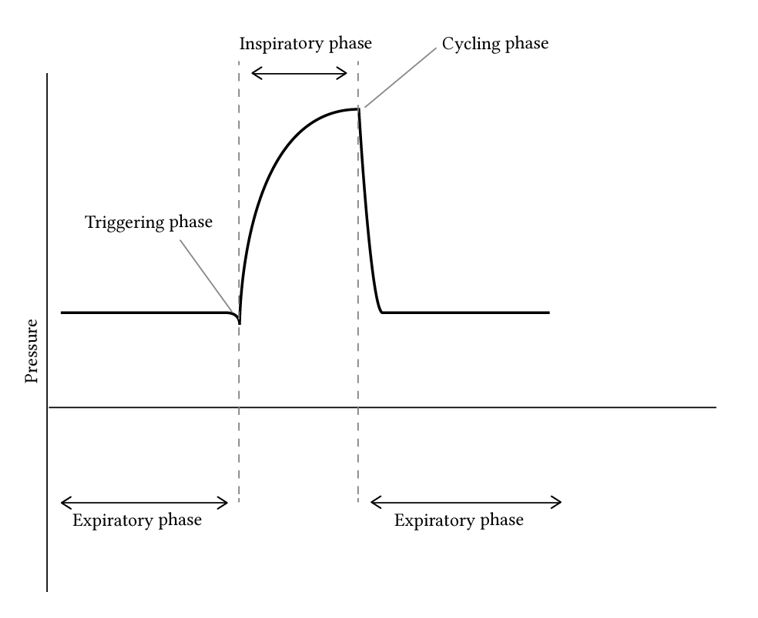
Phases of Mechanical Ventilation
- Four distinct phases, each of which has a governing variable which determines how that phase proceeds:
- Trigger phase: initiate phase controlled by the trigger variable
- Inspiratory phase: controlled by the limit variable
- Cycling phase: controlled by the cycle variable
- Expiratory phase: governed by the PEEP variable; the patient exhales passively
Monitoring
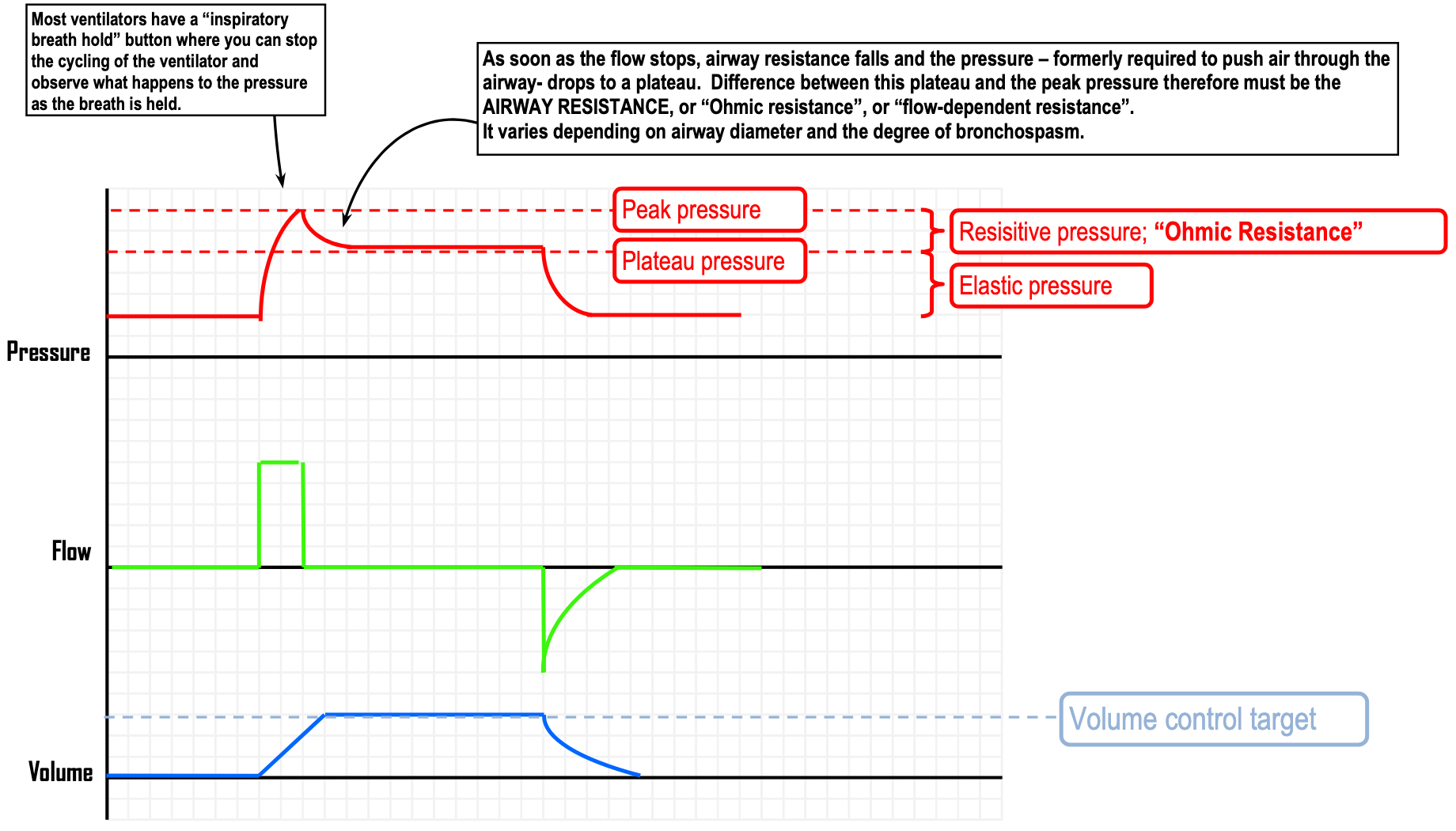
- An increasing in the absence of an increasing suggests airway resistance is increasing (e.g. bronchospasm, excessive secretions, mucous plug, foreign body aspiration, extrinsic airway compression)
- An increasing suggests compliance is decreasing (e.g. pulmonary oedema, pleural effusion, pneumothorax, right mainstem bronchus intubation, ascites or other abdominal distension)
| Likely problem | ||
|---|---|---|
| Increased | Normal | Increased airway resistance |
| Increased | Increased | Decreased lung compliance |
Gas Exchange
Normal Gas Exchange
- Alveolar ventilation equation:
- Where
- is the partial pressure of in arterial blood
- is the rate of systemic production
- is the pressure of inspired air
- is the alveolar ventilation
- Importantly
| Mechanism | Examples |
|---|---|
| VQ mismatch | Pneumonia, PE, pulmonary oedema, COPD |
| Shunt | Congenital heart disease, pulmonary AVM |
| Thickening of the alveolar-capillary membrane | Interstitial lung disease, pulmonary oedema |
| Destruction of the alveolar capillary membrane | Emphysema |
Monitoring
- ABG Interpretation
- Pulse oximetry
- Capnography
- Note that
- However, the gap can be:
- Increased to >5 mmHg in low cardiac output, COPD, PE, advanced age
- Decreased to <2 mmHg in high cardiac output states (e.g. septic shock)
- However, the gap can be:
- Note that
PEEP
Preload
- Increased intrathoracic pressure, thus
- Decreased venous return,
- Thus reduced left ventricular stroke volume
- Thus reduced left ventricular contractility
- Thus reduced left ventricular oxygen demand
- If the left ventricle is decompensating because it is overfilled and overstretched ( “congestive” heart failure) the decreased preload will push it back into the more efficient area of the Frank-Starling curve.
- If the PEEP is causing hemodynamic instability, the patient needs more fluid.
RV Afterload
- ↑ Intrathoracic pressure ⇒ ↑ pulmonary artery pressure
- ↑ RV afterload
- Increased right ventricular work and oxygen demand