Part of: Mechanical Ventilation
Ventilation alarms should be treated with great attention — often demanding the same attention as a code blue.
Crashing Patient on the Ventilator
- Call for help, airway cart, ultrasound and scalpel
- If patient arrests, start CPR, delegate two staff members to chest compressions and continue to seek underlying cause
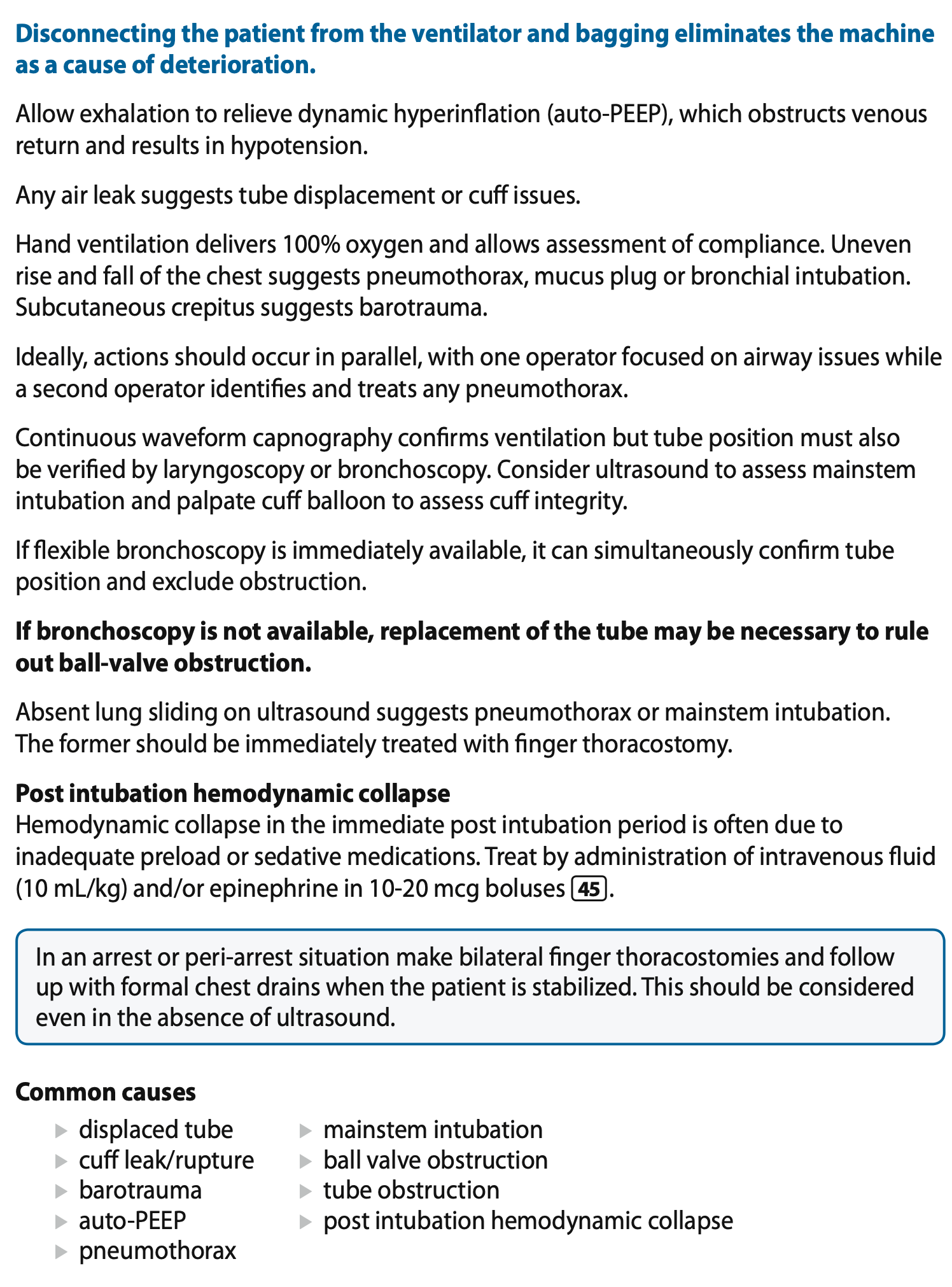
- Disconnect patient from ventilator and allow exhalation
- BMV 100% oxygen with PEEP valve at 10 breaths/min (if PEEP valve available)
- Confirm endotracheal tube position with waveform capnography
- Listen for any air leak from the mouth or neck
- Pass a bronchoscope, tube exchanger, bougie or suction catheter to exclude obstruction
- Consider re-intubation unless a patent, correctly positioned tube is directly visualised
- Use bedside ultrasound to diagnose pneumothorax and if confirmed, treat with finger thoracostomy
- If no pneumothorax, review the list of common causes
DOPES Mnemonic
| Letter | Problem | Action |
|---|---|---|
| D | Dislodged or displaced ETT | Confirm position; re-intubate if necessary |
| O | Obstructed ETT (mucous, blood, kinking) | Pass suction catheter, bougie or bronchoscope |
| P | Pneumothorax | USS → finger thoracostomy if confirmed |
| E | Equipment failure | Disconnect from ventilator → try BMV |
| S | Stacked breathing (auto-PEEP) | Disconnect and allow full exhalation |
COPD on the Ventilator
- Increase inspiratory flow rate to 80-100 L/min to shorten the inspiratory time
- Avoid increasing respiratory rate
- Ensure adequate bronchodilators
- Ensure flow is returning to 0 before next inspiration
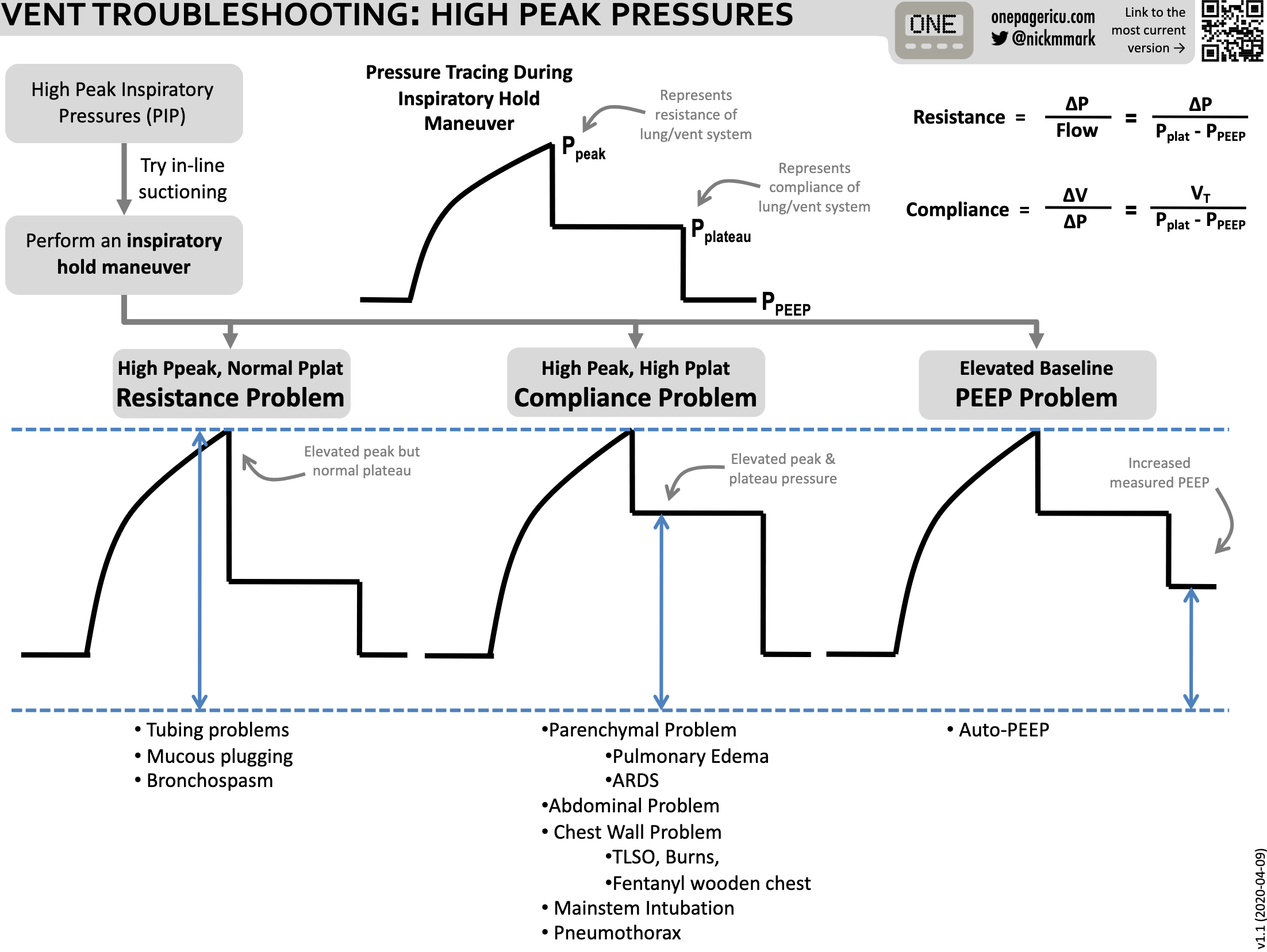
High Pressure Alarm
Common causes:
- ↑ Airway resistance (secretions, bronchospasm, biting on ETT, obstruction of exhalation valve, ETT too small)
- ↓ Lung compliance (pulmonary oedema, pneumonia, ARDS, pneumothorax, haemothorax, abdominal distension, chest wall rigidity)
- Patient-related (coughing, patient-ventilator dyssynchrony)
Troubleshooting:
- If low or falling → crashing on the ventilator
- Assess the patient: respiratory distress, cyanosis, agitation, ↓ SpO₂
- Check for capnograph waveform
- Check the airway — inspect ETT for obstruction, kinking, displacement; suction if secretions present
- Inspect circuit for kinks, water accumulation or disconnections
- Change tidal volume to ≤ 8 mL/kg predicted body weight
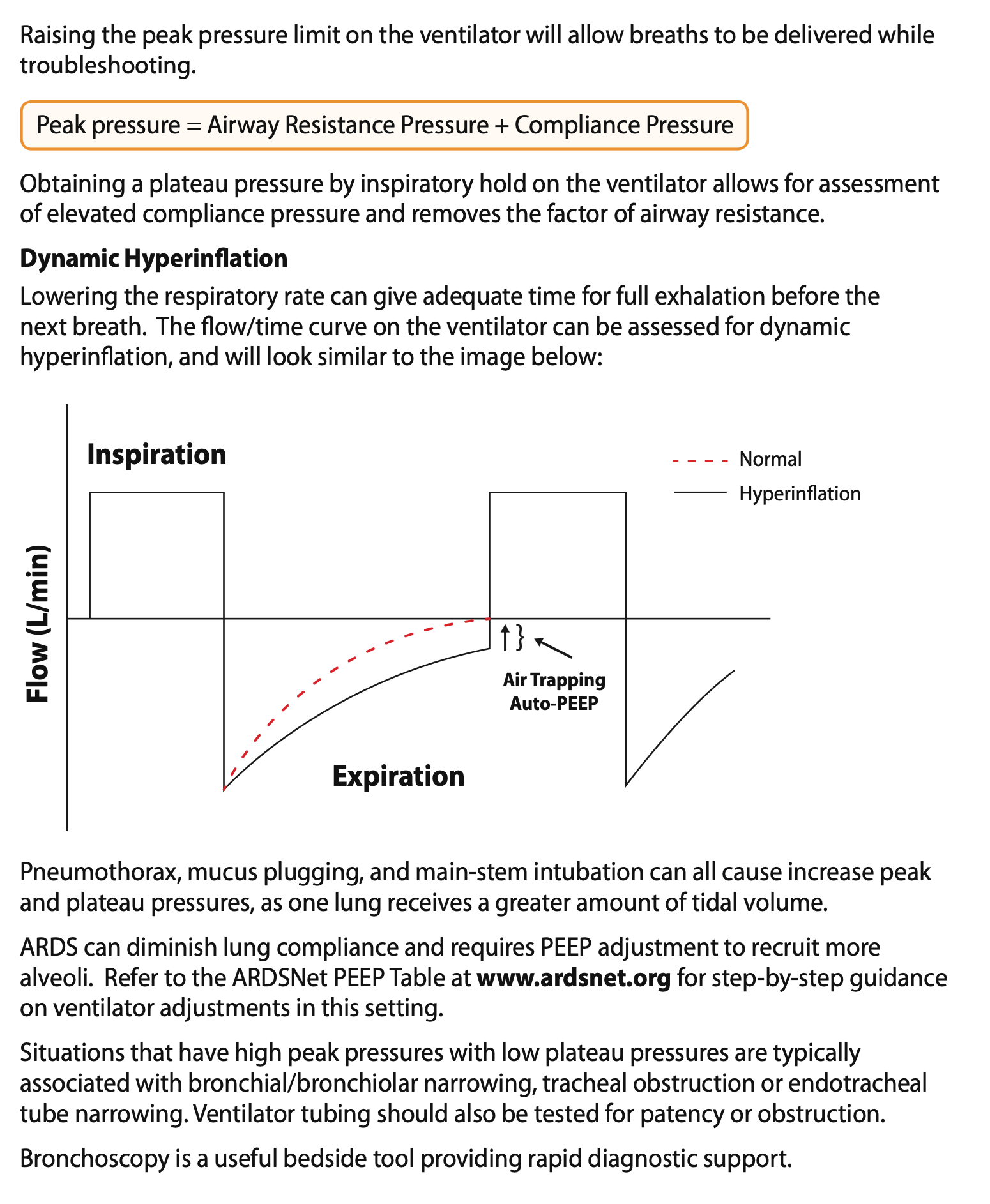
- Increase the ventilator peak pressure alarm limit until entire set volume is delivered without triggering
- Perform inspiratory hold on ventilator to assess plateau pressure:
P_peak - P_plateau < 5 cmH₂O (↑ plateau)?
→ Rule out dynamic hyperinflation (lower RR or disconnect)
→ If no dynamic hyperinflation: USS/CXR to exclude pneumothorax and mainstem intubation
→ Consider atelectasis, pneumonia, mucous plugging or ARDS
→ Reduce VT until Pplateau < 30 cmH₂O
P_peak - P_plateau > 5 cmH₂O (↑ peak only)?
→ Auscultate: bronchodilators if obstructive disease
→ Check each piece of circuit for obstruction
→ OK to leave peak pressure limit high if Pplateau remains < 30 cmH₂O
Low Pressure Alarm
Common causes:
- Circuit disconnection (ventilator tubing, loose humidifier, disconnected exhalation valve)
- Airway leaks (ETT cuff leak, deflated cuff, improperly positioned ETT)
- System failure (loss of gas supply, power failure, air compressor malfunction)
- Incorrect ventilator settings (pressure limit set too high, VT set too low, excessively sensitive trigger)
Troubleshooting:
- Consider manual ventilation with resuscitation bag while troubleshooting
- Check for circuit disconnection
- Inspect all ventilator tubing and connections
- Examine the ETT cuff for leaks
- Confirm that the ETT is correctly positioned
- Ensure the ventilator is receiving adequate gas supply and power
Low Alarm
Common causes:
- Leaks in system
- Patient disconnection
- Airway problems (malpositioned ETT, partial extubation, deflated cuff, tracheostomy tube leak)
- Inadequate ventilator settings (VT set too low, premature cycling, inappropriate inspiratory time, excessive respiratory demand)
Troubleshooting:
- Assess patient: chest movement, SpO₂, overall stability — if inadequate or crashing → crashing patient
- Inspect for disconnection — entire circuit from ventilator to patient
- Check for leaks — evaluate cuff pressure, inspect for air leaks around ETT or tracheostomy tube
- Confirm airway position
- Evaluate ventilator settings and mode
High Frequency Alarm
Common causes:
- Respiratory distress (hypoxaemia, pain, fever, metabolic acidosis, inadequate pressure support)
- Airway narrowing (secretions, mucous plugging, bronchospasm)
- Auto-triggering (sensitivity set too high, circuit leaks, water in tubing, cardiac oscillations, external movement)
Troubleshooting:
- Assess the patient: accessory muscle use, low SpO₂, diaphoresis, increased WOB
- Evaluate oxygenation and ventilation (review recent blood gas results)
- Check the airway for bronchospasm, mucous plugging; suction if indicated
- Review ventilator sensitivity if auto-triggering is suspected
- Optimise support: ↑ , inspiratory flow, pressure support; treat pain/anxiety; correct acid-base disorders
Apnoea Alarm
Common causes:
- Circuit disconnection
- Depressed respiratory drive
- Fatigue or neuromuscular weakness
- Inadequate sensitivity
Troubleshooting:
- Assess the patient: chest rise, respiratory effort, SpO₂, signs of instability
- Confirm circuit integrity: disconnection, loose tubing or major leaks
- Provide manual ventilation while identifying the source of the problem
- Evaluate sedation and respiratory drive; consider contributing medications
- Review trigger settings and backup ventilation
High PEEP Alarm
Common causes:
- Auto-PEEP / air trapping
- High respiratory rate
- Short expiratory time
- Insufficient inspiratory flow (prolonged inspiratory time)
- Obstructive lung disease / bronchospasm
- Excessive tidal volume
- Inappropriate I:E ratio
Troubleshooting:
- Prolong expiratory time
- Reduce respiratory rate
- Reduce tidal volume
- Increase inspiratory flow to shorten inspiratory time
- Treat bronchospasm with bronchodilators
- Suction retained secretions if indicated
- Reassess the set PEEP level
Low PEEP Alarm
Common causes:
- Leak in the ventilator circuit
- Loose tubing connection
- ETT cuff leak
- Leak around tracheostomy tube
- Faulty valve or humidifier connection
- Strong patient inspiratory effort
Troubleshooting:
- Inspect the circuit for leaks or loose connections
- Evaluate cuff inflation and airway integrity
- Confirm that the ventilator valves are functioning properly
- Assess inspiratory flow settings
- Adjust settings to better match patient demand if needed
Low Oxygen Alarm
Common causes:
- Circuit disconnect
- Incorrect gases
- Sensor malfunction