Part of: Mechanical Ventilation
- Everyday someone is on the ventilator, assess for liberation unless patient is on , patient is unstable, or on high amounts of vasopressors:
- Lifting sedation
- Weaning/liberation trial
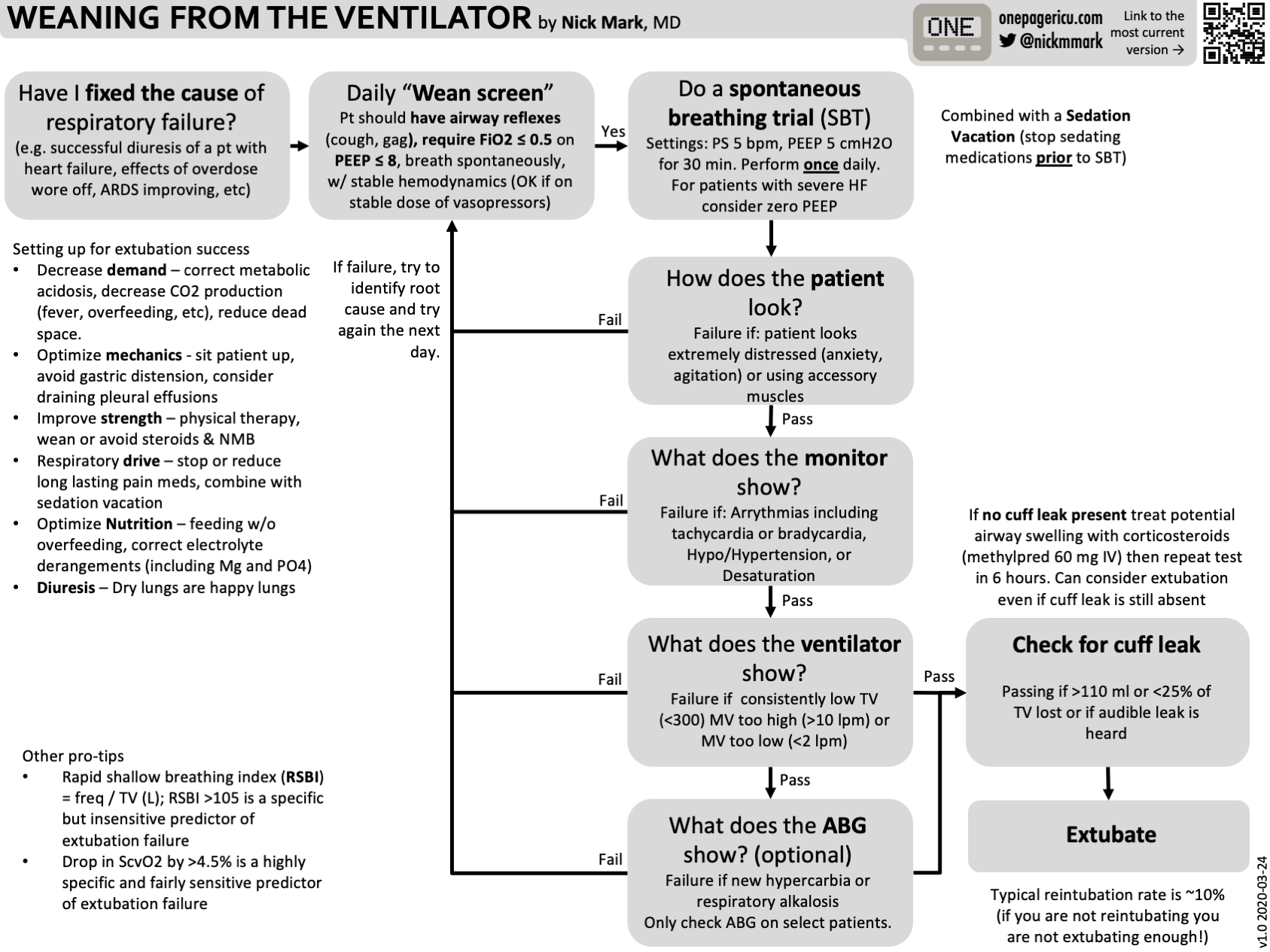
Spontaneous Breathing Trial (SBT)
Readiness Criteria
| System | Criteria |
|---|---|
| Respiratory | < 50% with PEEP ≤ 10 cm (higher PEEPs may be acceptable in obese patients); or is normal or close to baseline for patients with chronic hypercapnoea |
| Cardiovascular | No ongoing myocardial ischaemia; HR <140; Not on high-level vasopressors |
| Neurological | Patient is arousable and ideally following commands |
| Renal | No uncontrolled acid-base disturbances |
SBT Settings
- Pressure support ventilation with 5 cm PS and 5 cm PEEP (PSV 5/5)
- If a patient can tolerate the above settings for 30 minutes, they are likely ready for extubation
Passing Criteria
- Adequate oxygenation: saturating >88% without requiring more than ~50%
- Adequate ventilation: no ↓ in minute ventilation, no ↓ in tidal volume, does not increase by >10 mmHg
- No signs of severe fatigue:
- Agitation, diaphoresis, use of accessory muscles
- RSBI () <1051
- No obvious complications (arrhythmia, hypotension, severe hypertension)
- Complete an ABG:
- pH > 7.35 and and → likely to succeed extubation
If Apnoea Develops During SBT
Causes:
- Patient was hyperventilated prior to the trial → place back on standard ventilator mode, decrease backup rate to stimulate spontaneous breaths, then repeat SBT
- Cheyne-Stokes breathing pattern
- Over-sedated
On Failing a SBT
If a patient fails a SBT
- Place the patient back on full ventilator support immediately
- Repeat SBT later in the day only if something easily manipulable can be corrected (e.g. sedation), otherwise repeat the following morning
Causes of failing a SBT:
| Category | Causes |
|---|---|
| Pulmonary | Volume overload/pulmonary oedema, bronchospasm, pleural effusion, VAP, atelectasis/mucous plugging, small ETT, occult ETT occlusion |
| Cardiovascular | Angina, pulmonary embolism |
| Neurological/Psychiatric | Anxiety, chronic tachypnoea |
| Metabolic | Metabolic acidosis, elimination of chronic compensatory metabolic alkalosis (e.g. COPD), electrolyte abnormalities (especially hypophosphataemia) |
| Ventilator | Dyssynchrony or inadequate ventilator support |
Investigations to consider:
- Electrolytes including CMP
- Review of fluid balance and examination for volume overload
- Chest imaging (CXR, POCUS)
- Review acid-base status and compare to baseline bicarbonate
- CT angiography if considering PE
On Passing a SBT
Passing means the patient is strong enough to sustain the work of breathing, but also consider:
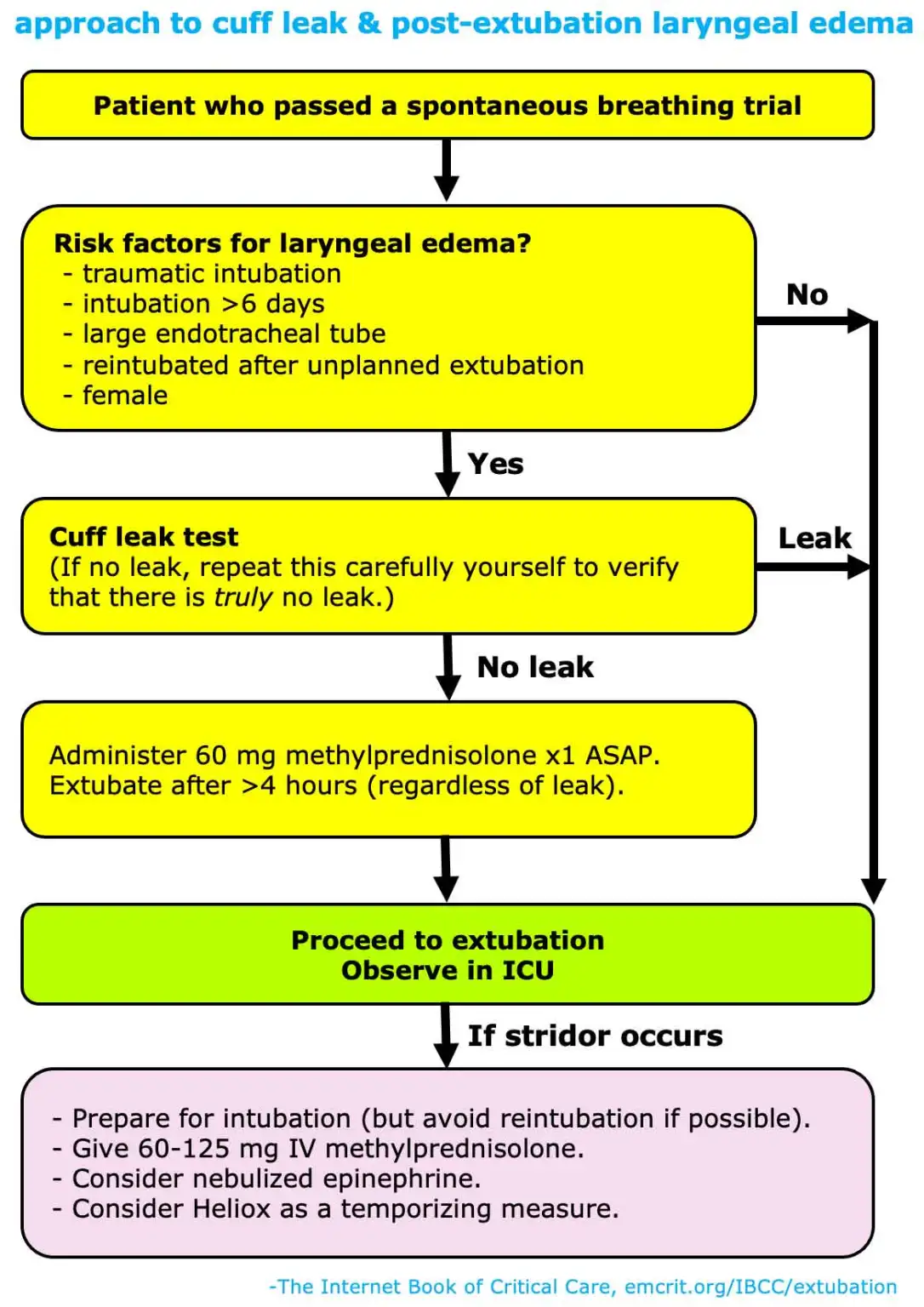
- Risk of post-extubation laryngeal oedema
- Will the patient be able to maintain their airway
Assessment of ability to maintain airway is based on four factors (subjective):
- Patient’s mental status
- Is the patient producing plenty of secretions (e.g. requiring suctioning < q2hrly)?
- Does the patient have a history of hypercapnoea?
- Does the patient have a strong cough (assessed while suctioning)?
Extubation
Checklist for Extubation
- Optimise sedation
- Ideal target: following commands, mildly distressed by ETT when sedation held
- Consider cross-tapering from propofol onto dexmedetomidine
- Optimise volume status
- Extubation increases preload and blood pressure
- Examine fluid charts for fluid overload; consider diuresis before extubation if required
- Optimise acid-base status
- Treat metabolic acidosis prior to extubation (patient compensates with respiratory alkalosis)
- Patients with chronic hypercapnoea and chronic compensatory respiratory alkalosis should ideally be restored to their baseline bicarbonate level prior to extubation
- Review chest X-ray
- Observe for any treatable disease process (e.g. pleural effusion)
- Review insulin regimen and glycaemic control
- Extubation often involves discontinuation of enteral nutrition
- Other considerations
- Suction stomach
- Check for cuff leak if indicated; air leak on deflation of ETT cuff suggests absence of tracheal swelling
Post-Extubation Support
- Most patients can go from extubation to high flow nasal prongs (HFNP); however BiPAP can be considered in patients with heart failure or COPD
- For HFNP to be effective:
- HFNP needs to be continued for a substantial amount of time (24-48 hours) unless the patient is already on night-time BiPAP
- The flow rate should be increased as high as can be tolerated by the patient (ideally 50-60 L/min)
Unplanned Extubation
- Accidental extubation (e.g. while turning or transporting patient) → generally requires re-intubation
- Self-extubation (patient intentionally removes their own ETT):
- Stop all sedative infusions
- Place the patient on BiPAP
- Observe
- Re-intubate if clinically indicated
Footnotes
-
RSBI has a specificity of 44% predicting extubation failure. Should be considered a red flag, yet some patients can still be extubated despite a high RSBI (e.g. in patients with interstitial lung disease who have chronic tachypnoea) ↩