Classification
Can be classified by aetiology:
- Primary ⇒ autoimmune disorder characterised by isolated thrombocytopenia (most common)
- Secondary ⇒ secondary to identifiable trigger:
- Autoimmune disorders → antiphospholipid syndrome
- Malignancy → Lymphoma, Leukaemia (particularly CLL)
- Infection → HIV, HCV
- Drugs → many check AMH
- Can be classified by chronicity:
- Newly diagnosed ITP ⇒ all cases <3 months of diagnosis
- Persistent ITP ⇒ ITP lasting 3-12 months
- Chronic ITP ⇒ ITP lasting >12 months
Epidemiology
- US Statistics:
- Females affected more than males
- Children :: highest prevalence <5 years old; typically self-limiting after viral infection; 80% resolve in 12 months
- Adults :: highest prevalence in >55 years old; often incidental finding on routine CBC
Pathophysiology
- Antiplatelet antibodies (mostly IgG directed against GpIIb/IIIa, GpIb/IX, bind to surface proteins on platelets → sequestration by spleen and liver → ↓ platelet count → ↑ bone marrow megakaryocytes and platelet production)
Clinical Features
- Splenomegaly is typically absent in patients with ITP
- Clinical features can correlate with platelet count; but most patients are asymptomatic:
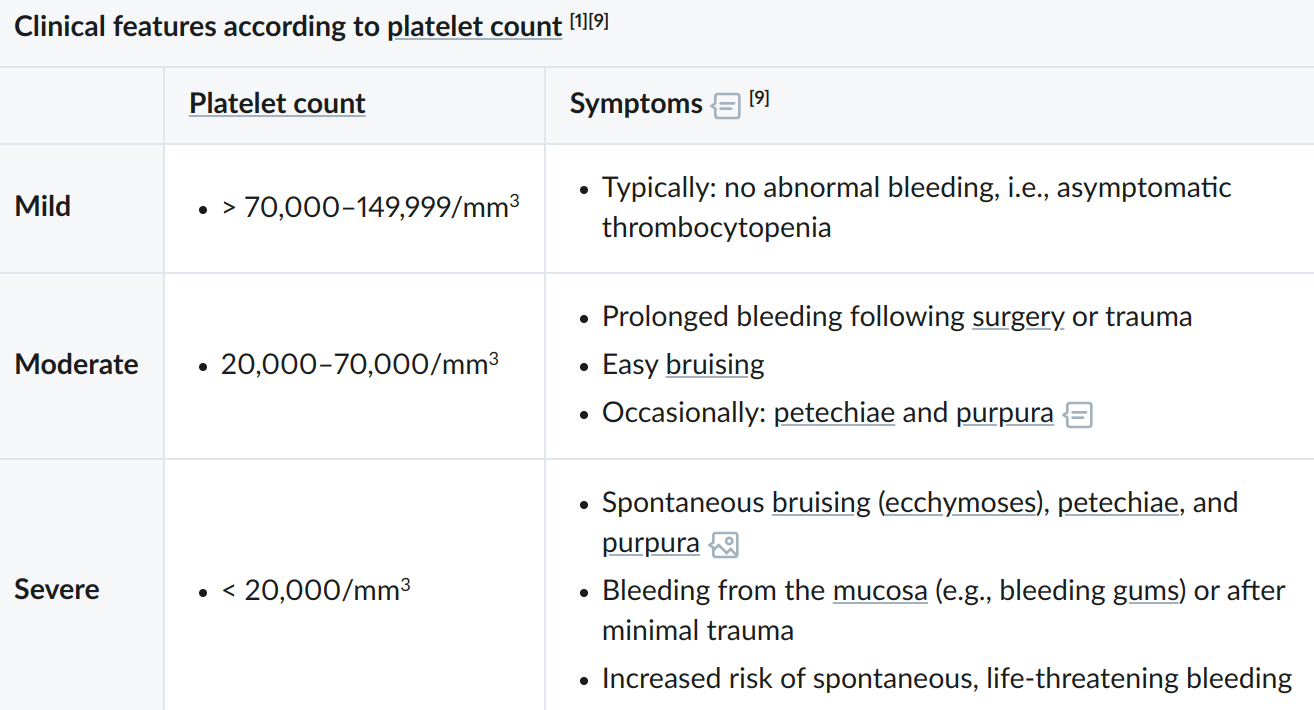
- Minor mucocutaneous bleeding is possible:
- Subcutaneous bleeding (e.g. bruising, petechiae, purpura)
- Mucosal bleeding (e.g. mild epistaxis, gingival bleeding)
Investigations
- CBC: typically
- Coagulation panel is usually normal (unless secondary ITP)
- Bleeding time may be ↑
Diagnosis
- ITP is often a diagnosis of exclusion in patients who have thrombocytopenia with no other abnormalities
Management
- In all patients stop medications that impair platelet function (e.g. NSAIDs)
Emergency Treatment
- Indicated for patients with:
- Life threatening bleeding (typically at platelet )
- Acute neurological features (i.e. intracranial bleed)
- Anticipated urgent surgery or invasive procedure
Emergency Management:
- Haemostatic control of bleeding (if present)
- Start combination therapy with:
- Corticosteroids (e.g. methylprednisolone)
-
- IV immunoglobulin
-
- Platelet transfusions as needed
- If ⌀ response consider thrombopoietin receptor agonist (TPO-RA) e.g. romiplostim
Conservative Managmenet
- Indicated for asymptomatic or minor mucutaneous bleeding only patients with:
- Adults with a platelet count
- Children with any platelet count
- Remember to refer to haematology and counsel on bleeding risks1
First Line Medical Therapy
- Indicated for:
- Adults with platelet count
- Patients with significant non-life-threatening mucosal bleeding (e.g. severe epistaxis)
- Symptoms impacting quality of life
- Therapy:
- Corticosteroids (e.g. dexamethasone or prednisone)
- If contraindicated or not tolerated: IVIG or anti-Rho(D) immunoglobulin
Therapy for ITP Refractory to First-Line or Persistent/Chronic ITP
- TPO-RAs (e.g. Romiplostim, Eltrombopag)
- Rituximab
- Splenectomy
- Indications:
- Treatment resistent thrombocytopenia lasting >12 months
- Severe bleeding refractory to other treatment
- Spleen should be confirmed as primary site of platelet breakdown using radioactively labeled thrombocytes if possible
- Indications:
Additional Flashcards
Suspect {{c1::ITP}} in a child with thrombocytpoenia and petechiae following a viral illness
- What is the emergency management for ITP once haemostatic control is achieved?
{{c1::Corticosteroids}}
{{c1::IVIG}}
{{c1::Platelet transfusions as needed}}
First line therapy for ITP is with {{c1::corticosteroids (e.g. dexamethasone or prednisone)}}
Indicated for:
- Adults with platelet count $<\pu{30,000 count // mm3}$
- Patients with significant non-life-threatening mucosal bleeding (e.g. severe epistaxis)
- Symptoms impacting quality of life
Footnotes
Footnotes
-
Advised to avoid contact sports and other high-risk activities ↩