Common Causes (Corridor Thoughts)
- Otological causes (primary)
- Otitis Media and its subtypes
- Acute otitis media
- Otitis media with Effusion
- Chronic suppurative otitis media
- Otitis Externa
- Perforation
- Foreign body in ear (younger children, pain, hearing loss ± foul-smelling discharge)
- Cerumen impaction
- Otitis Media and its subtypes
- Referred pain
- Dental causes: teething, dental caries
- Pharyngitis/tonsilitis (always examine ENT)
- Cervical lymphadenopathy
- Other important
- Acute Mastoiditis
- Tumours (consider in those with recurrent otitis media, unilateral hearing loss)
- Can consider other things like ramsay hunt
Assessment
- A→E Assessment including vitals (temperature)
- Your main concern here is whether there is any concern for sepsis; consider if the patient is active and playful or floppy and unengaged
- In Infants, especially <6 months old, the diagnosis of AOM and OME can be inaccurate; consider other causes of the febrile child
Examinations
- General paediatrics exams
- Examine skin for any rashes
- Listen to chest sounds for any signs of respiratory tract involvement
- ENT
- Oropharynx, teeth, jaw and lymph nodes
- Inspection of pinna, tragus and external auditory canal and palpation of the tragus
- Pain with manipulation of the tragus ⇒ Otitis Externa
- Examine the mastoid process for swelling, erythema and tenderness ⇒ mastoiditis
- If able to perform the weber and rinne test: show show conductive hearing loss (2° to effusion)
- Weber localised to the affected ear
- Rinne test: air conduction impaired in the affected ear
- Otoscopy
- Sit the child on the parent’s lap with the head immbolised against the parent’s chest
- Pull posteriorly and look anteriorly and superiorly for the tympanic membrane
- Assess the tympanic membrane for:
- Translucency: translucent/opaque/partly opaque
- Colour: clear/grey/white/amber/red
- Position: normal/retracted/bulging
- mobility: normal/decreased or absent
- Middle ear effusion is suggested by:
- Obscuring of the bony landmark
- Air fluid levels or bubbles behind the TM
- Bulging tympanic membrane
- Otorrhoea
- Otitis media with effusion is suggested by:
- Normal or retracted tympanic membrane, clear or amber in colour
- Acute otitis media is suggested by:
- Bulging tympanic membrane, purulent effusion and distinct erythema of the tympanic membrane
- Note that a red tympanic membrane may occur with fever or crying
- Also differentiate between distinct erythema of the tympanic membrane itself and increased vascularity with red appearance only in areas of blood vessels
- Sit the child on the parent’s lap with the head immbolised against the parent’s chest
- Other
- Assess facial nerve function especially in chronic suppurative otitis media

| Otoscopy Appearance | Notes |
|---|---|
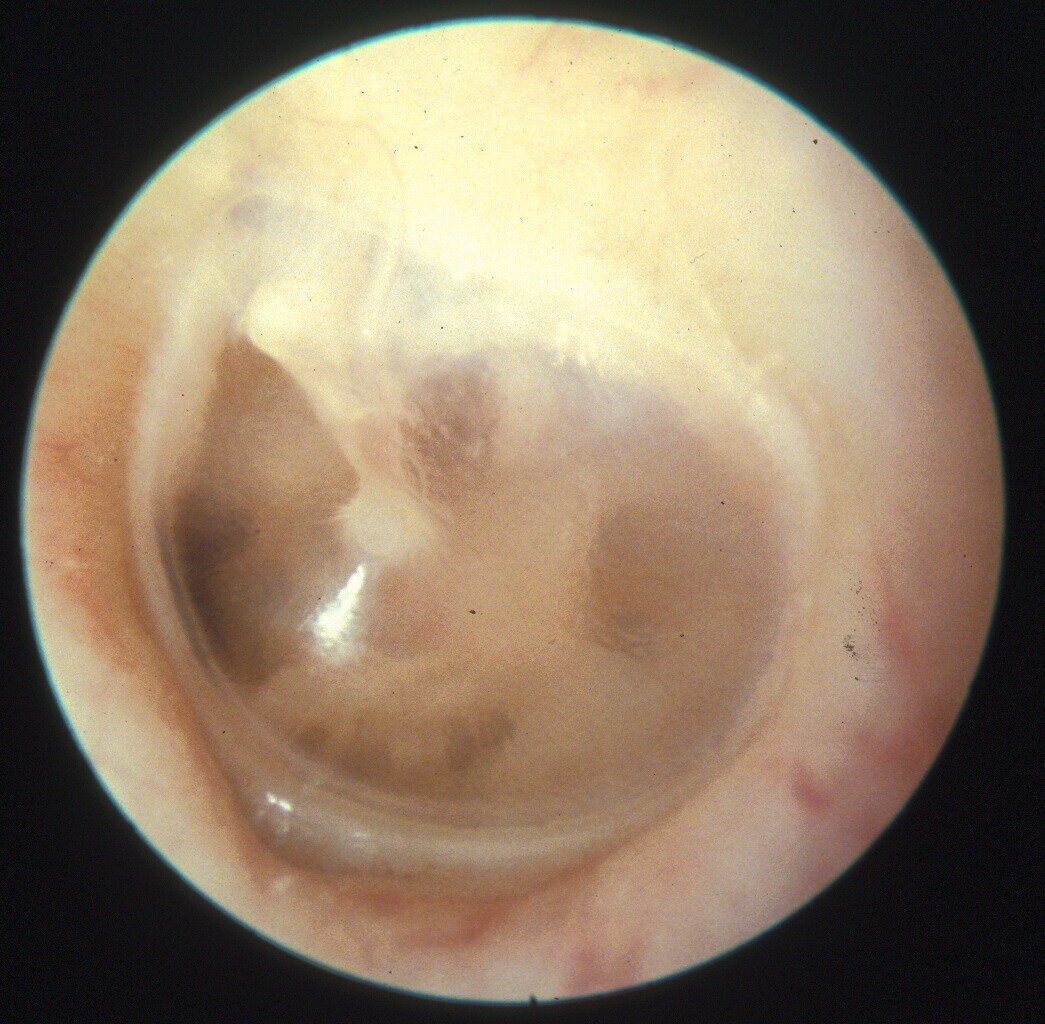
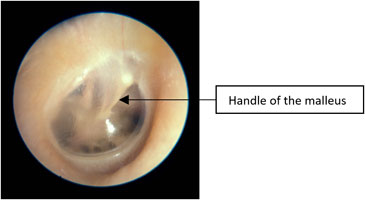 | Normal Tympanic Membrane TM is translucent Handle of the malleus is vertical No erythema |
 | Injected Tympanic Membrane Pink/red tympanic membrane Often seen with fever, eustachian tube obstruction or viral URTI Tympanic membrane is transparent (no effusion) The handle of the malleus is visible and more horizontal |
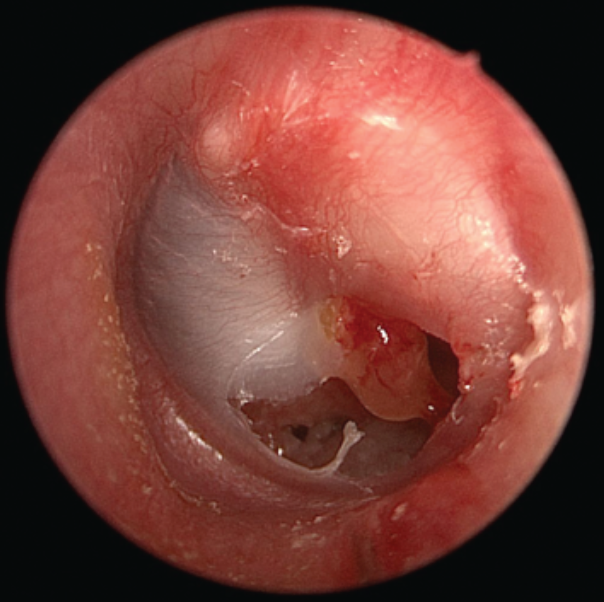
    | Acute Otitis Media Loss of the tympanic membrane landmarks (esp. handle of the malleus) Tympanic membrane is opaque either completely red (inflammation) or white (pus in middle ear) |
 | Bullous myringitis (type of AOM) Can be mistaken for herpes zoster oticus (Ramsay Hunt) The tympanic membrane shows erythematous changes with visible isolated hemorrhagic infiltrates (dark spots) |
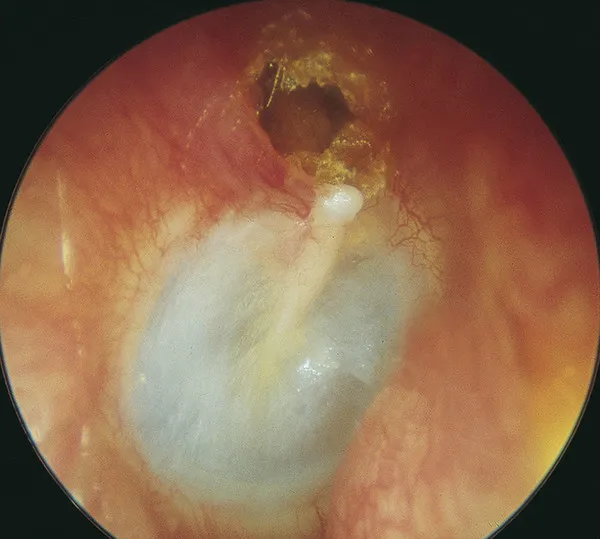
 | Acute Otitis Media with Perforation Lies on the same spectrum as chronic chronic suppurative otitis media except it is the initial appearance. Accompanied often by pain and other features of AOM |
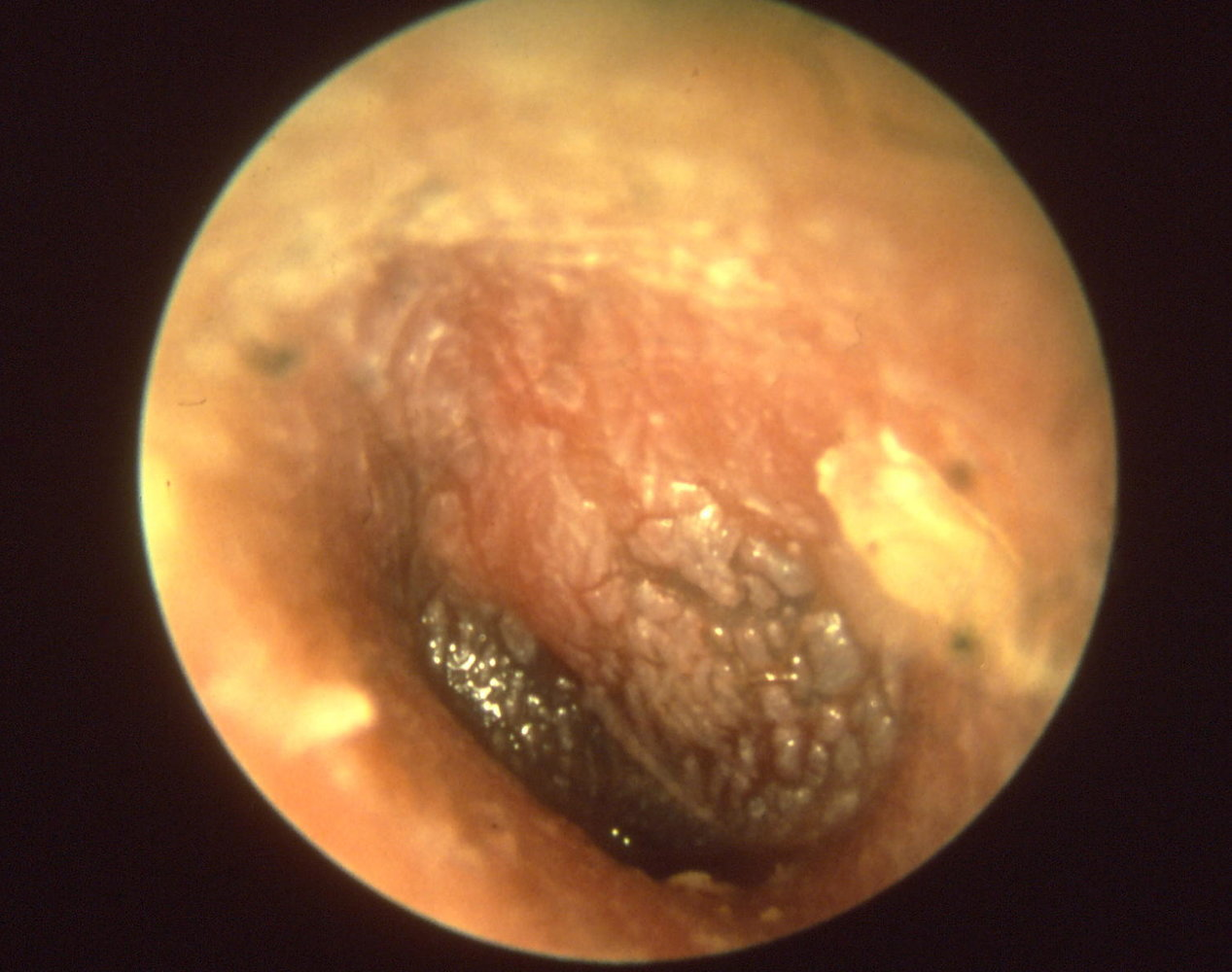
  | Chronic Suppurative Otitis Media Also known as chronic mucosal otitis media. Differs from AOM by duration (>6 weeks) |
 | Chronic Squamous Otitis Media secondary to cholesteatoma |
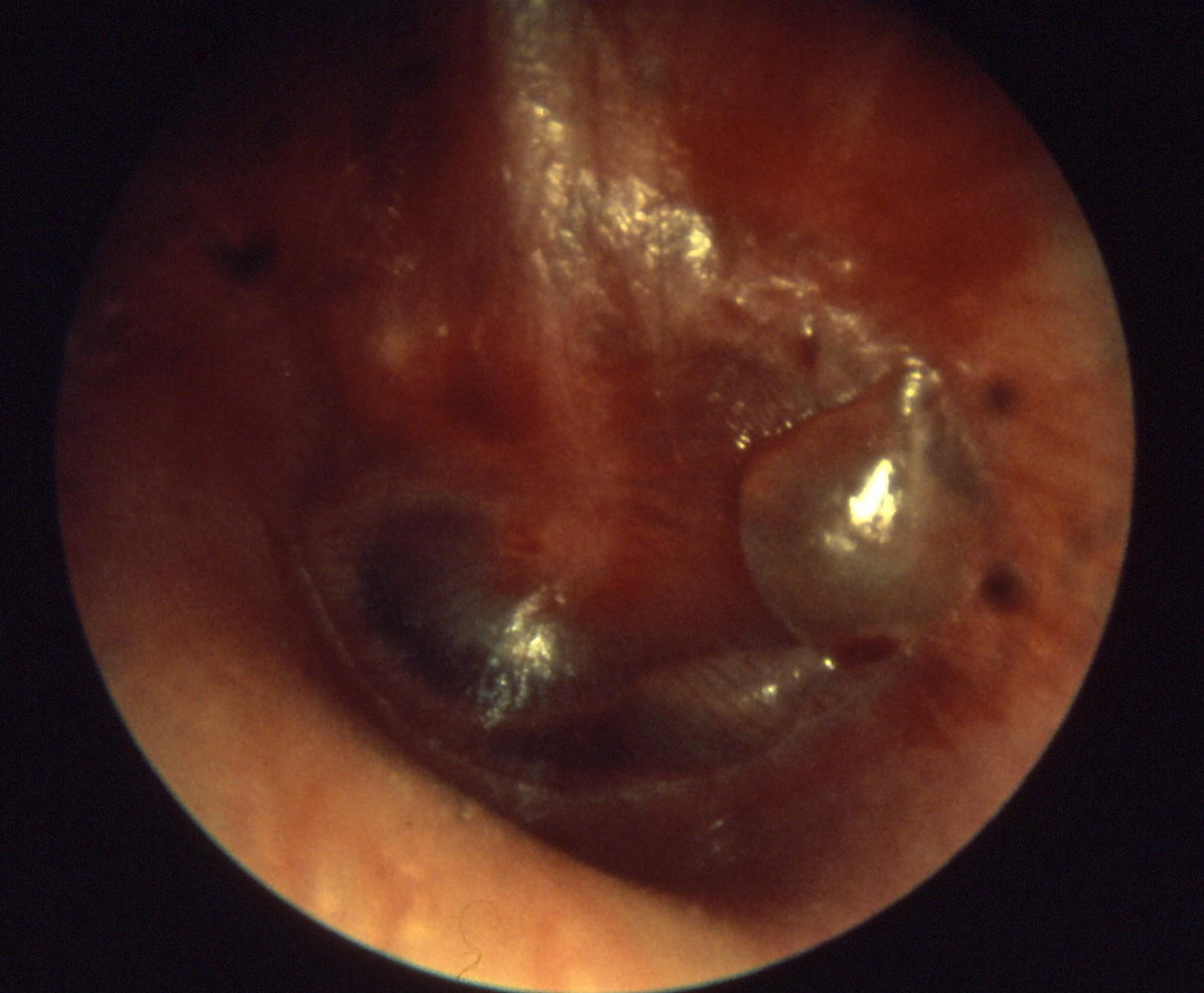
  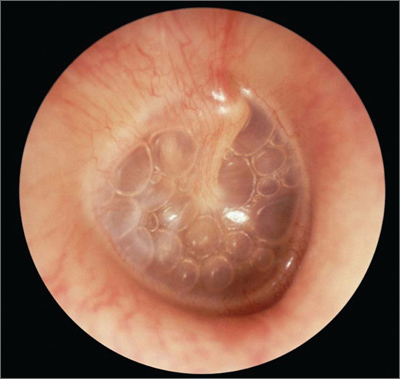  | Otitis Media with Effusion Tympanic membrane is retracted with prominence of handle of malleus which is more horizontal Tympanic membrane may be bulging or have air fluid level behind Yellow/amber appearance Light reflex apparent |
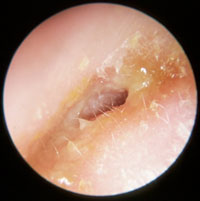 | Otitis Externa Ear is tender to examine; not recommended to perform otoscopy Skin of external ear canal is swollen and often a thin layer of pus |
| ^otoscopy-table |
Warning
Patients with an attic perforation (squamous chronic otitis media) or persistent crusting or granulation (above the malleus, in the top part of the TM) should be referred to an ENT surgeon immediately to exclude cholesteatoma
Investigations
- None regularly performed
- Imaging:
- Consider CT head if there is concern for mastoiditis or other intracranial complications
Management
- Symptomatic management
- Admission/Disposition and Scoring Criteria
- Only children with complications of acute otitis media such as mastoiditis or other intracranial complications require hospitalisation
- Dicharge
- If using wait-and-see approach patients should be instructed to follow up with GP if symptoms do not improve in 48-72 hours or earlier if symptoms worsen or signs or symptoms of complications of AOM
- Referral
- Management (specific)