Importantly for patients with BMI<35 measure their waist-to-height ratio to assess central adiposity - NICE guidelines
Patients from Asian, Middle Eastern, Black African or African-Caribbean family background are more prone to central adiposity so use lower thresholds ⇒ reduce thresholds by 2.5 (i.e. overweight: 22.5 - 27.4) - NICE guidelines
Can also just measure waist circumference directly (same procedure as waist-to-height ratio)
Increased risk in ♂ at 94cm (Asians 90cm) and in ♀ at 80cm
Substantially increased risk in ♂ at 102cm and in ♀ at 88cm
Other defintiions:
Patients with a BMI <35 should be encouraged to measure their own waist-to-height ratio to assess central adiposity
Management
Non Pharmacological Measures
Set /achievable/ goals (e.g. maintenance of 5 to 10% loss of initial body weight, reduction in waist circumference, reduced BP) and record progress. Consider referral to other health professionals (eg dietitian, exercise physiologist, psychologist) or a multidisciplinary obesity clinic for expert advice.
Shift the energy balance: reduce energy intake via improved eating habits and increase energy expenditure by reducing sedentary behaviour and increased physical activity
Can explain to patient as a sea-saw and you have to tip the balance
For OSCE purposes can break down into:
Set goal: 5-10% of body weight with tracking
MDT referral
Diets
Exercise
Behavioural change
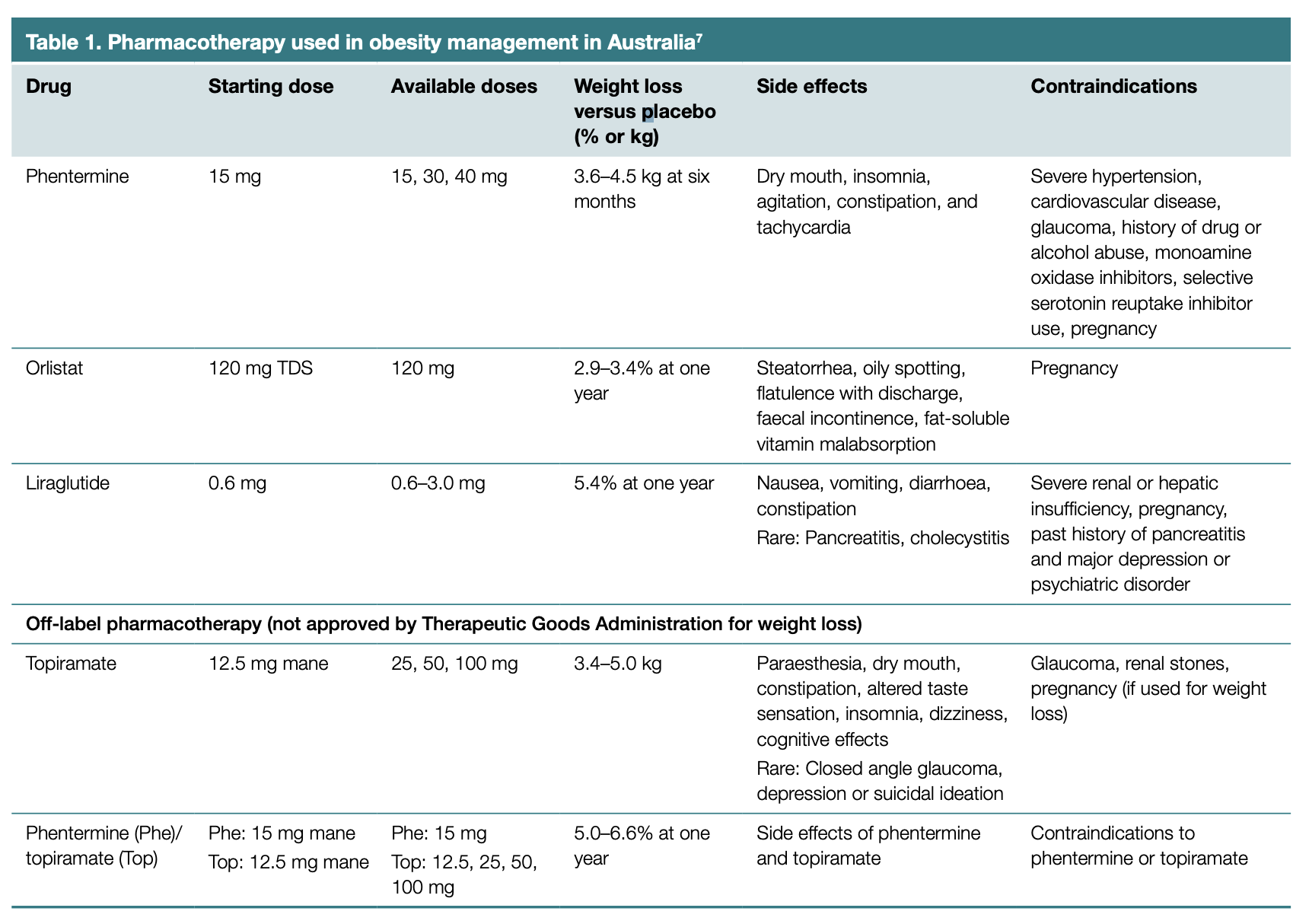
Pharmacological Measures
Pharmacotherapy for weight management should be seen as an adjunct to lifestyle intervention, just as it is for managing hypertension, diabetes and cardiovascular disease, not as a replacement because of the benefits that lifestyle intervention provides beyond weight reduction.
Weight loss pharmacotherapy should be considerd for patients with BMI>30 or those with BMI 27-30 with obesity related complications.
Only orlistat, phentermine and liraglutide are approved by TGA for weight reduction (RACGP article from 2017).
Sympathomimetics
Work by supressing appetitie
Examples include phentermine, topiramate
Should not be used in patients with a history of cardiovascular disease (see image above for other contraindications)
Lipase Inhibitors
Works by leading to fat malapsorption (does not work systemically so blocks lipase in the bowel)
Examples include orlistat
Particularly useful for patients with diabetes and dyslipiedemia
GLP-1 Agonists
Examples include drugs ending in -glutide
Particularly beneficial for patients with diabetes
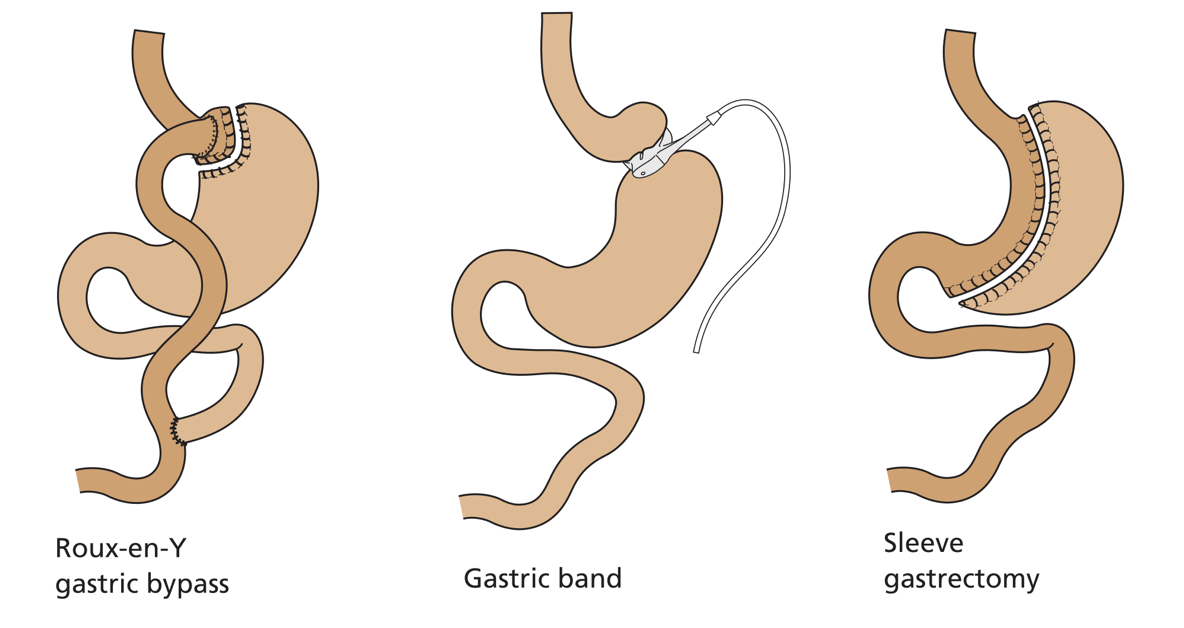
Restrictive procedures which reduce stomach veolume and limit oral intake; examples include sleeve gastrectomy (most common), adjustable gastric banding
Malabsorptive procedures (often performed in conjunction with restrictive) which bypass portions of the small intestine; thereby impairing absorption of macronutrients; examples include Roux-en-Y gastric bypass
The smaller gastric remnant works to produce a sensatino of satiety
Gastroplasty and bypass procedures have nutritional complications, in particular producing deficiencies of iron, vitamin B12, folate, vitamin D, calcium, copper and zinc
Roux-en-Y Gastric Bypass
Weight loss of 25-30% occurs within the first 2 years
Morbidity up to 15% at 1 year
Gastric Band
A plastic band is placed around the stomach 1-2cm below the GOJ
Weight loss of 20-30% is achieved gradually (2-3 years)
Morbidity is low (5%)
Sleeve Gastrectomy
The greater curve of the stomach is resected leaving a tube of stomach along the lesser curve
Weight loss of 20-30% is ahevable withinin the first 2 years
Morbidity is around 11%
Complications
General complications: anastomatic leaks, strictures, internal hernias
Specific
Oesophagitis and acid reflux in sleeve gastrectomy
Marginal ulceration, gstrogastric fistula, dumping syndrome and choledocholithiasis in Roux-en-Y bypass
Oesophageal or gastric perforation and band slippage in gastric banding
Importantly do not attempt NG tube insertion without consulting the surgical team