Aetiology
- Most common causes:
- Primary hyperparathyroidism ⇒ rarely causes severe hypercalcaemia
- Malignancy ⇒ more common cause of severe hypercalcaemia
- PTHrP e.g. in squamous cell lung cancer
- Bone metastases
- Myeloma
- Other causes
- Sarcoidosis
- Vitamin D intoxication
- Acromegaly
- Thyrotoxicosis
- Milk-alkali syndrome
- Typically occurs in patients with chronic kidney disease who are on calcium supplementation and vitamin D supplementation for treatment of osteoporosis
- Drugs
- Thiazides
- Calcium-containing antacids
- Dehydration
- Addison disease
- Paget’s disease of the bone with prolonged immobolisation
Mnemonic
- C: Cancer (PTHrP, mets, myeloma)
- H: Hyperparathyroidism
- A: Addison’s disease, Acromegaly
- M: Milk-alkali syndrome, Medications (thiazides, Ca-antacids)
- P: Paget’s disease (immobilisation-related)
- S: Sarcoidosis & other granulomas (TB, histoplasmosis)
- D: Dehydration
- VIT: Vitamin A or D toxicity, thyrotoxicosis
Physiology of Calcium Homeostasis
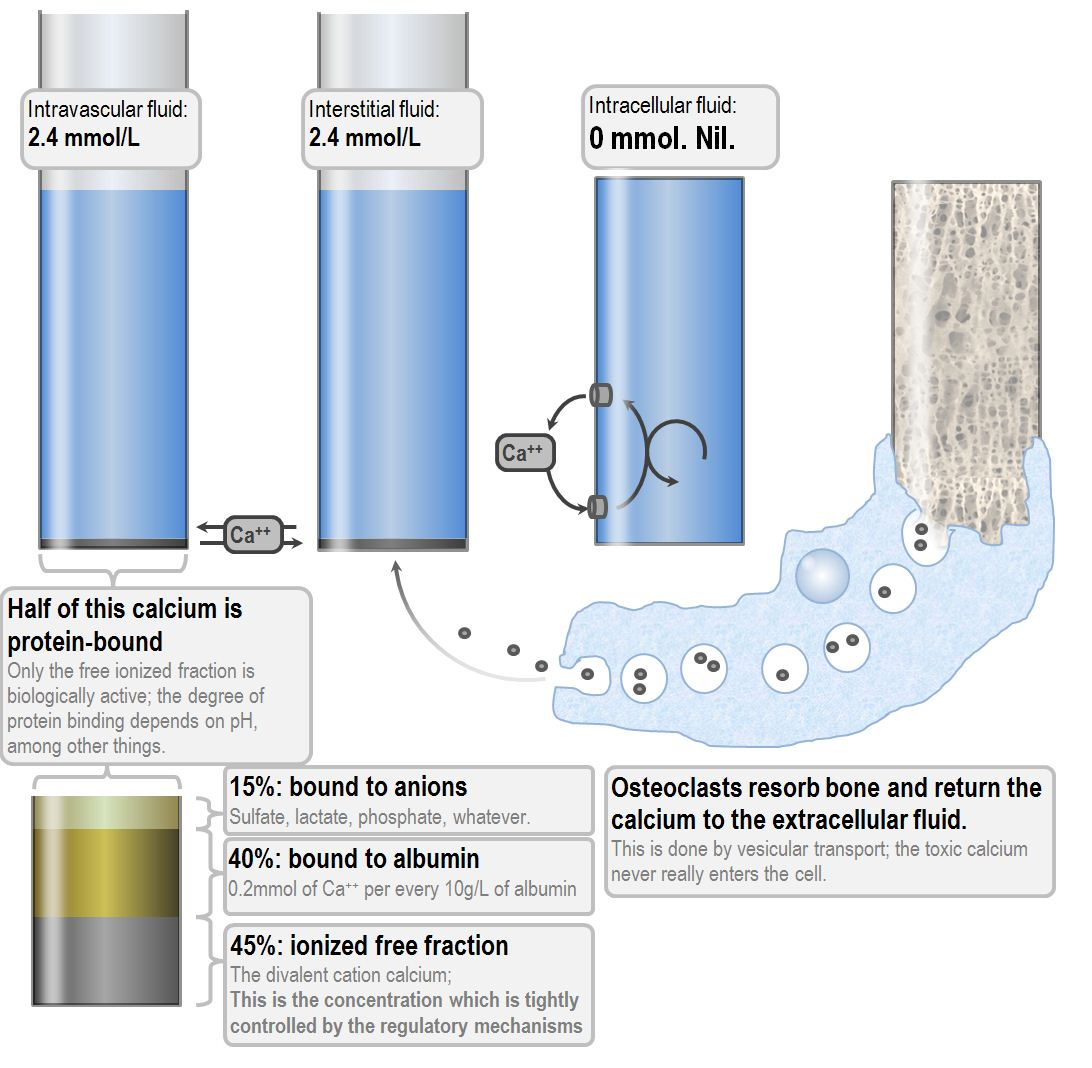
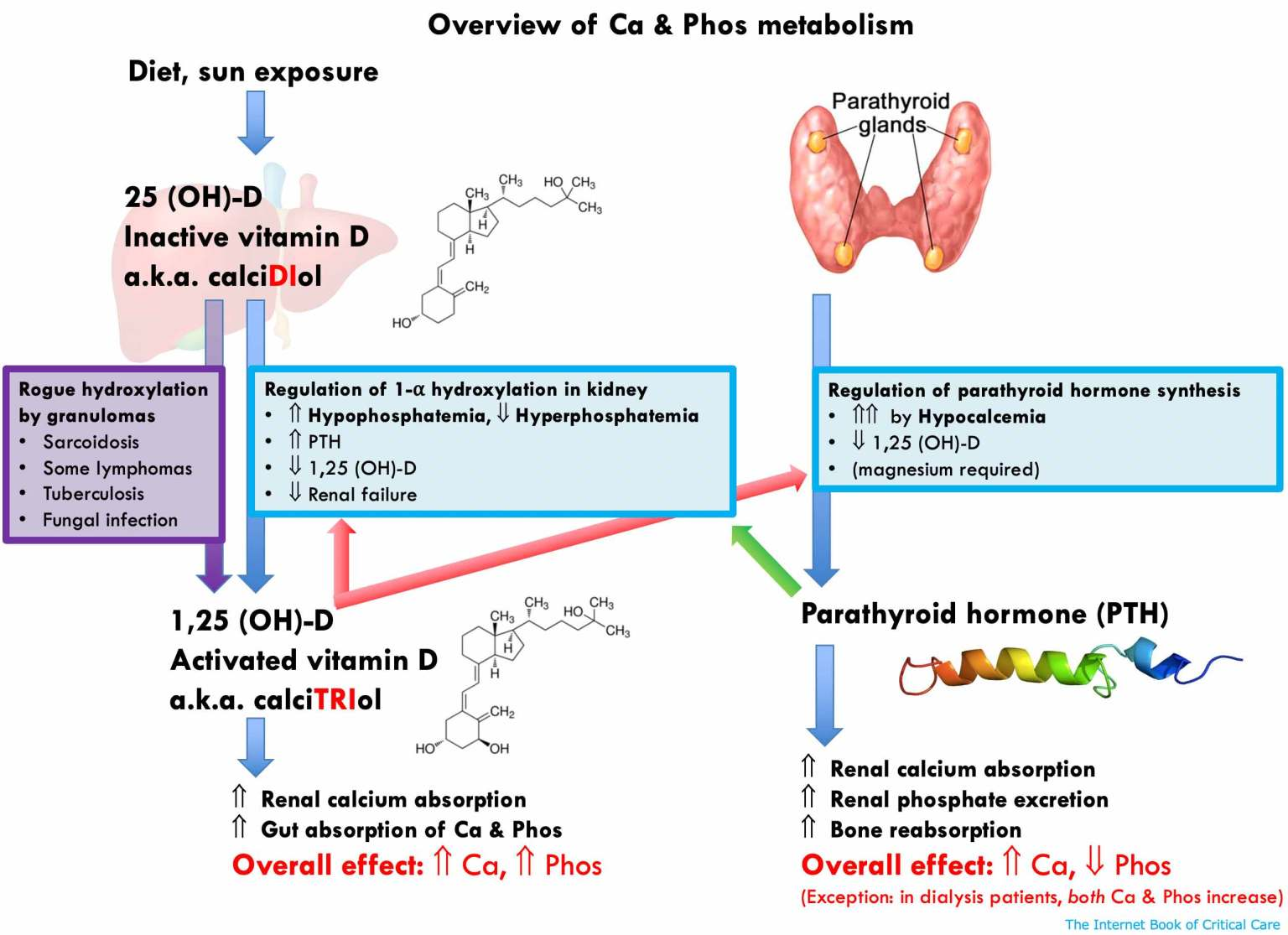
Parathyroid Hormone
- Secreted by chief cells of the parathyroid glands
- Most regulatory influences on PTH are inhibitory influences (inorganic phosphate is the only proper stimulatory release factor)
- Calcium level and PTH secretion relation is not linear; high calcium can never completely suppress PTH secretion and PTH secretion reaches a peak at calcium concentration of around 0.90 mmol/L
- Effects of PTH
- Osteoclastic:
- Direct effect on decreasing osteoblast activity
- Increased osteoclast activity
- Thus, increased release of calcium and phosphate from bone, and decreased bone deposition
- Renal:
- Decreased reabsorption of inorganic phosphate at the proximal tubule
- Increased reabsorption of calcium at the thick ascending limb of the loop of Henle
- Increased production of production of calcitriol in the kidney, through the stimulation of renal 1α-hydroxylase.
- Osteoclastic:
Calcitonin
- Secreted from parafollicular cells of the thyroid gland
- Osteoclastic:
- Direct effect on decreasing osteoclast activity1
- This decreases the resorption of bone, and therefore limits the entry of bone calcium and phosphate into the blood
- Renal:
- Calcitonin acts as a weak diuretic, increasing the elimination of sodium, chloride, phosphate and calcium. The effect on calcium is mainly due to inhibited reabsorption.
- It also increases production of production of calcitriol in the kidney, through the stimulation of renal 1α-hydroxylase.
- Intestinal:
- Calcitonin increases gastric acid and pepsin secretion and decreases pancreatic amylase secretion.
- It has no direct effect on calcium absorption in the intestine, but it can increase it indirectly by stimulating renal calcitriol synthesis
- Osteoclastic:
Action of Biphosphonates
- Inhibition of osteoclast and osteoblast activity
- Osteoclasts:
- Inhibition of osteoclast recruitment and adhesion
- Shortening of the life span of osteoclasts
- Inhibition of osteoclast activity by inhibiting several essential parts of the cholesterol synthesis pathway
- Inhibition of calcification by inhibiting the formation of calcium phosphate salts
- Mainly seen in high doses
- A totally physicochemical effect: they bind to the calcium of calcium phosphate
- The result is inhibition of formation and aggregation of calcium phosphate crystals and inhibition of the transformation of amorphous calcium phosphate into hydroxyapatite.
- Osteoclasts:
Presentation
- Stones, bones, groans and psychic moans
- GI symptoms of smooth muscle relaxation: constipation, anorexia, nausea and vomiting
- Neuro: Lethargy, hypotonia, confusion, coma
- Renal: Polyuria, dehydration, stones
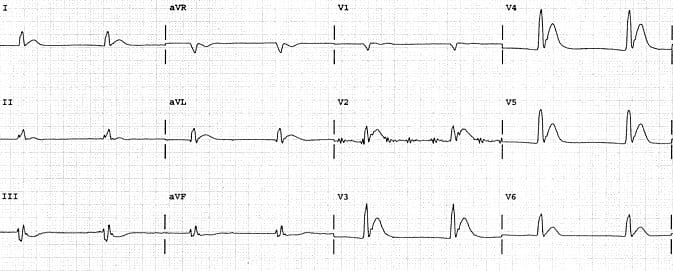
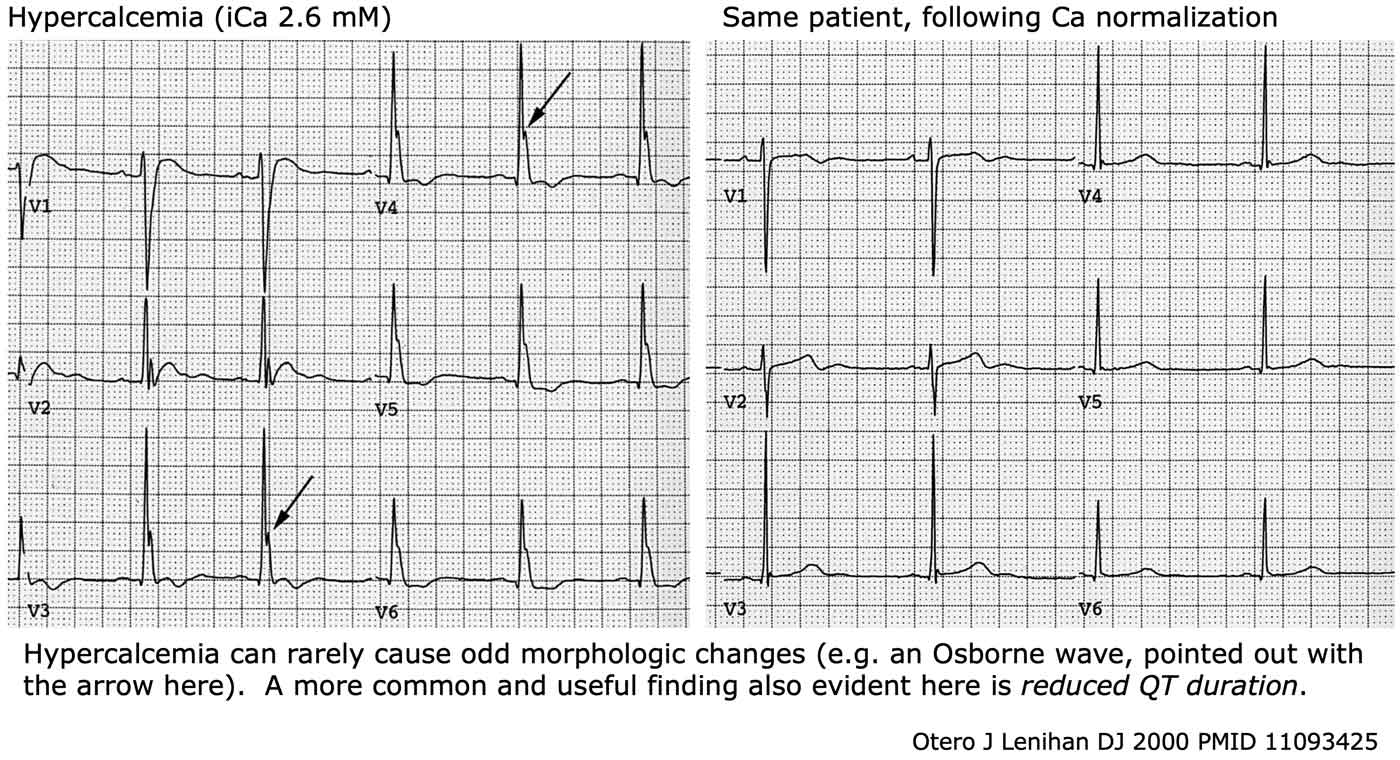
- ECG Changes
- Shortened QT interval
- Osborne J waves
- Shortened QT interval
Investigations
- Parathyroid hormone
- Review FBC and film for bone marrow malignancies and metastases
- TSH
- Vitamin D (25-hydroxy) level
- Vitamin A level
- Malignancy related tests
- Parathyroid hormone related protein
- Serum protein electrophoresis
- Prostate specific antigen
- Skeletal survey
- Alkaline phosphoatase
- Calcium urine for familial hypocalciuric hypercalcaemia
- Correcting for albumin, however evidence demonstrates that formulas actually perform worse than uncorrected calcium levels
Management
- Rehydration therapy with sodium chloride 0.9% 4-6 L by IV infusion over 24 hours
- IV furosemide can be used to treat fluid overload following rehydration but routine use has not been proved as beneficial
- Avoid hartmann’s solution, thiazide diuretics
- Plasmalyte is often preferred to sodium chloride 0.9% because it causes acidosis and patients with hypercalcaemia often have pre-existing acidosis
- Aim for urine output of 150-200 mL/hour, but importantly the ongoing infusion of fluid must be balanced to the urine output
- In acute life-threatening hypercalcaemia consider parenteral calcitonin salmon (salcatonin) in addition to biphosphonates to achieve a rapid effect
- Note that calcitonin causes a temporary reduction in calcium (effect does not work after ~2 days)
- If persisting severe hypercalcaemia after rehydration consider biphosphonate infusion
- Do not give in milk-alkali syndrome (should resolve without biphosphonate therapy) and pre-menopausal women
- Zoledronic acid is usually preferred dose-reduced in renal failure
- Takes time to take effect, hence calcitonin and biphosphonates are oten started simultaneously
- Hypercalcaemia caused by vitamin D toxicity, sarcoidosis or other granulomatous disease consider oral prednisolone
- Galium nitrate can also be considered but requires expert opinion
Sources
- Derranged physiology
- Passmedicine high yield textbook: Hypercalcaemia pages
- eTG articles: Calcium and phosphate imbalance → Hyperlcalcaemia
- LITFL
- Hypercalcaemia: https://litfl.com/hypercalcaemia/
- Hypercalcaemia DDx: https://litfl.com/hypercalcaemia-ddx/
- Hypercalcaemia ECG changes: https://litfl.com/hypercalcaemia-ecg-library/
- IBCC Textbook: https://emcrit.org/ibcc/hypercalcemia/
Footnotes
-
Their motility is affected within one minute, which is followed by a more gradual retraction ↩