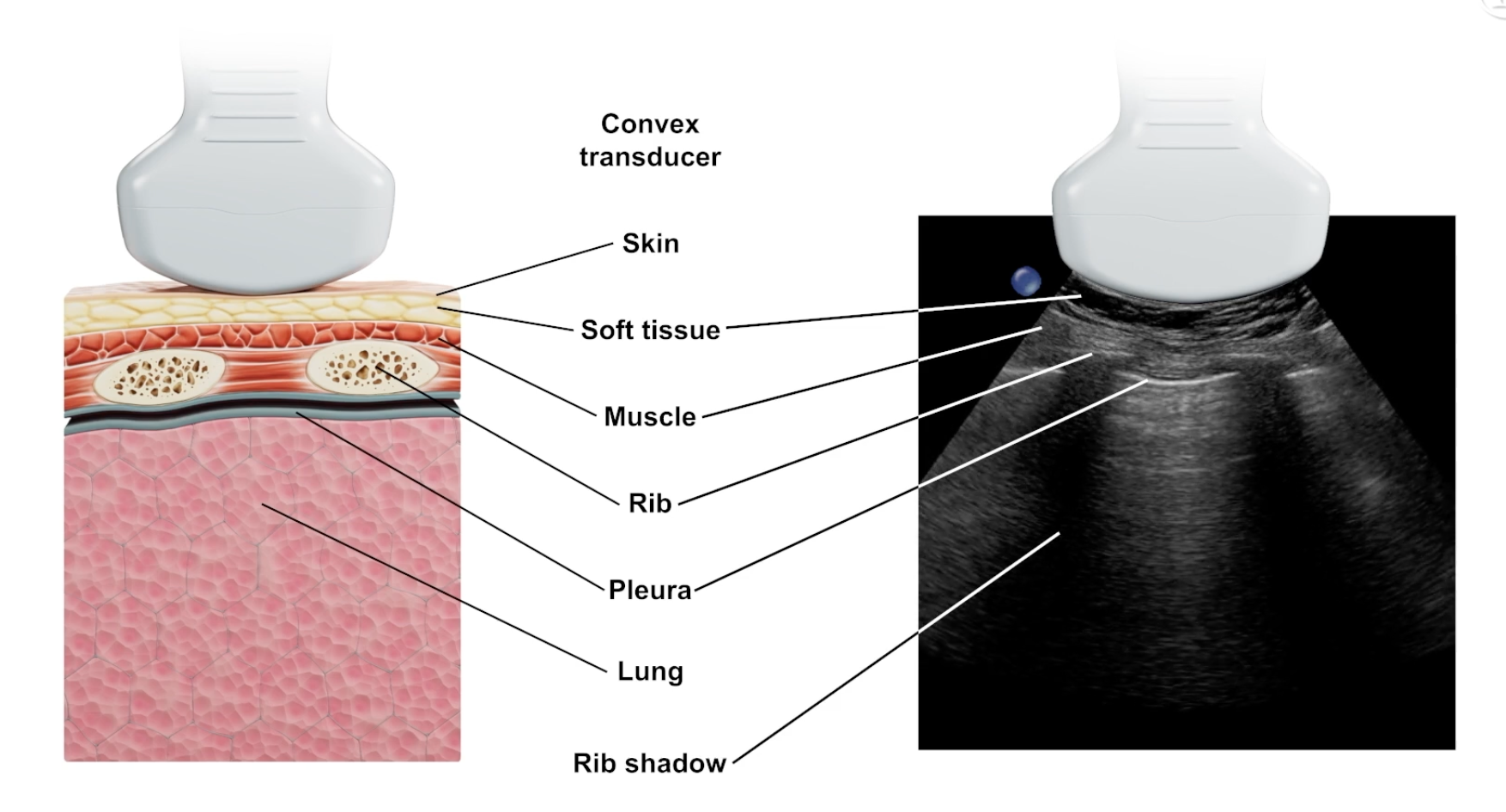
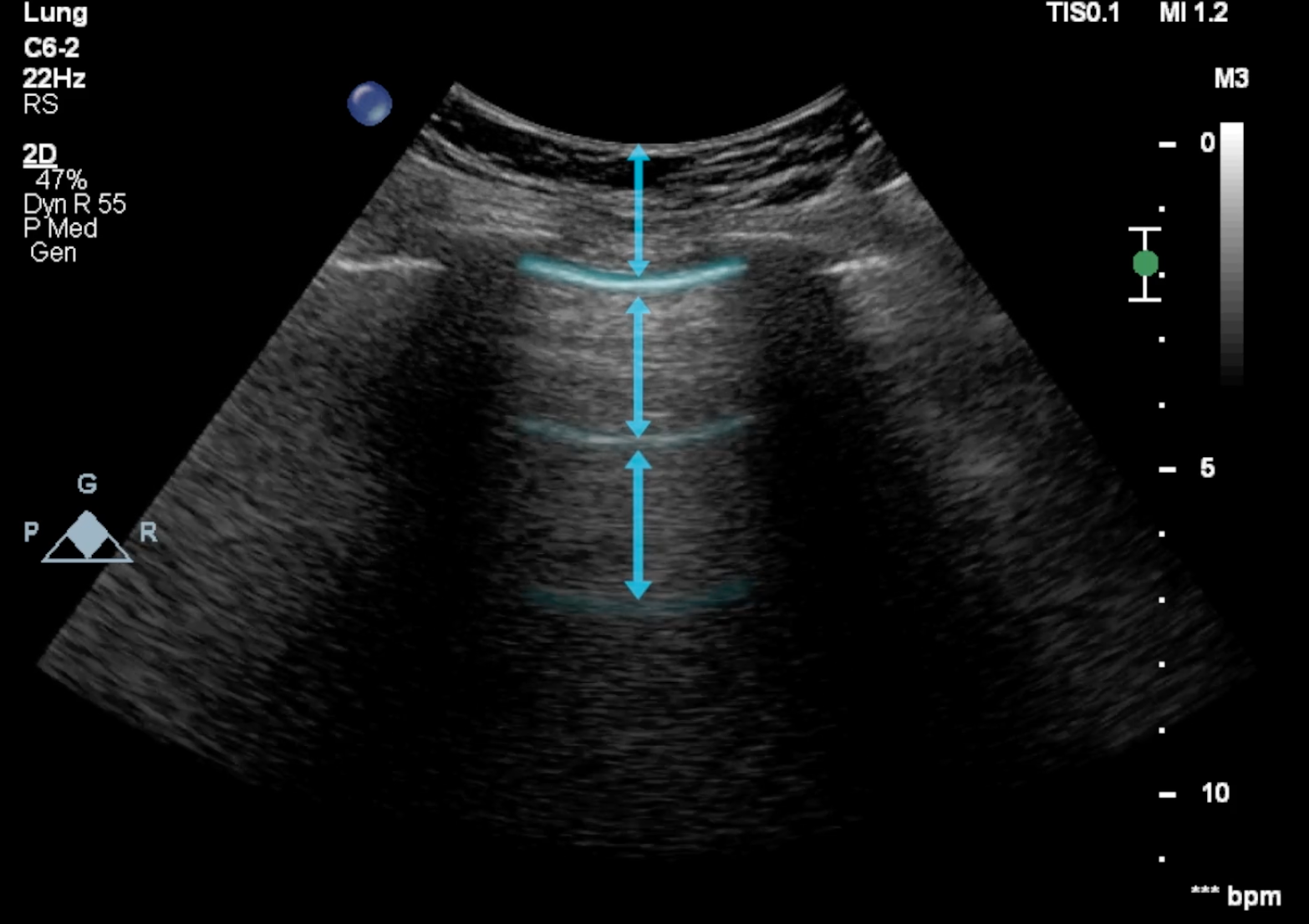
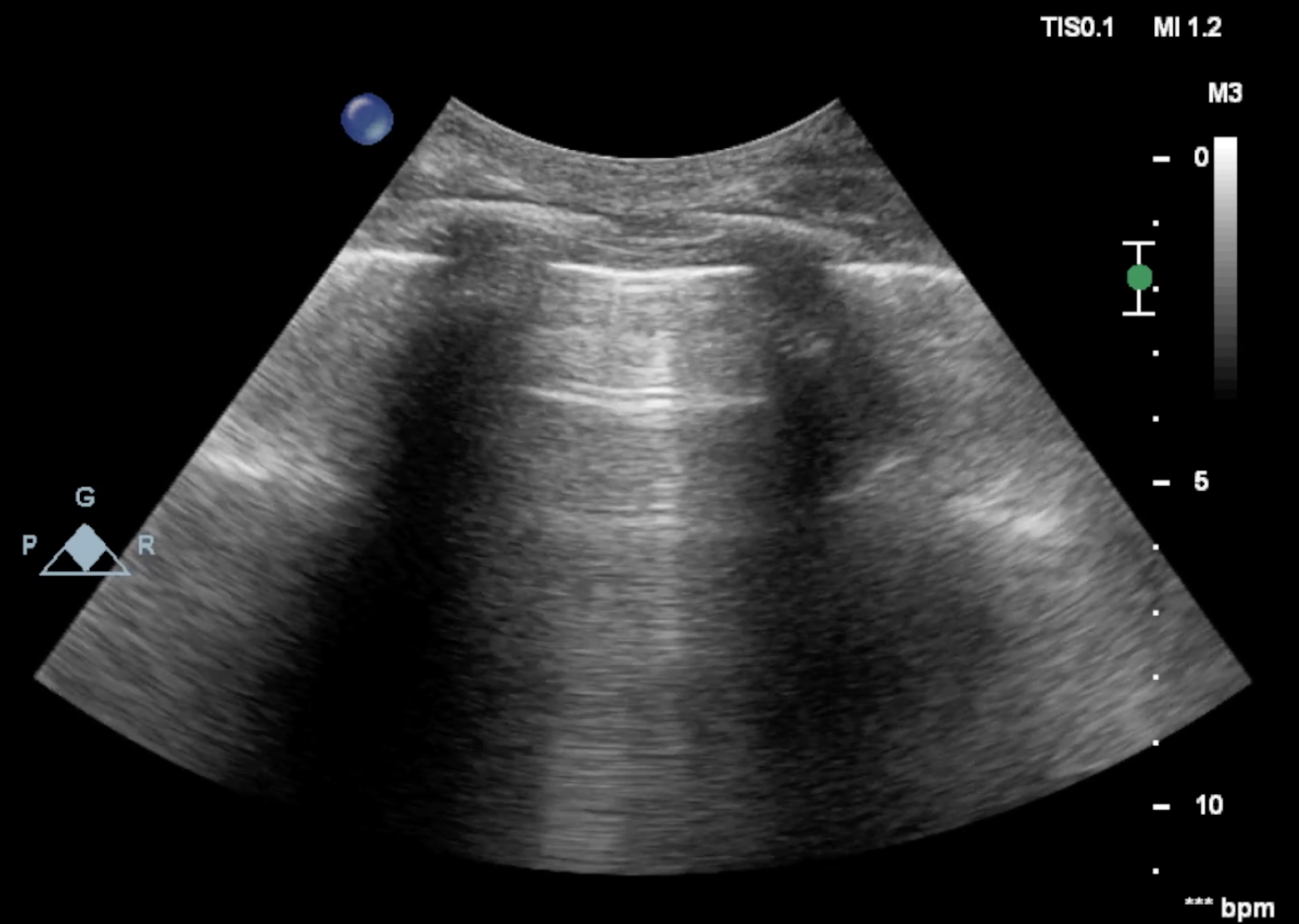
Characteristics of the Normal or Fully Aerated Lung
- Lung sliding: The visible, respiration-dependent movement of the pleural line
- Smooth pleural line
- A-lines: Horizontal artifacts caused by the reflection of air at the tissue boundary. They appear at perfectly equal distances from one another. The distance between the pleural line and the first A line is exactly equal to the distance between the pleura and the transducer
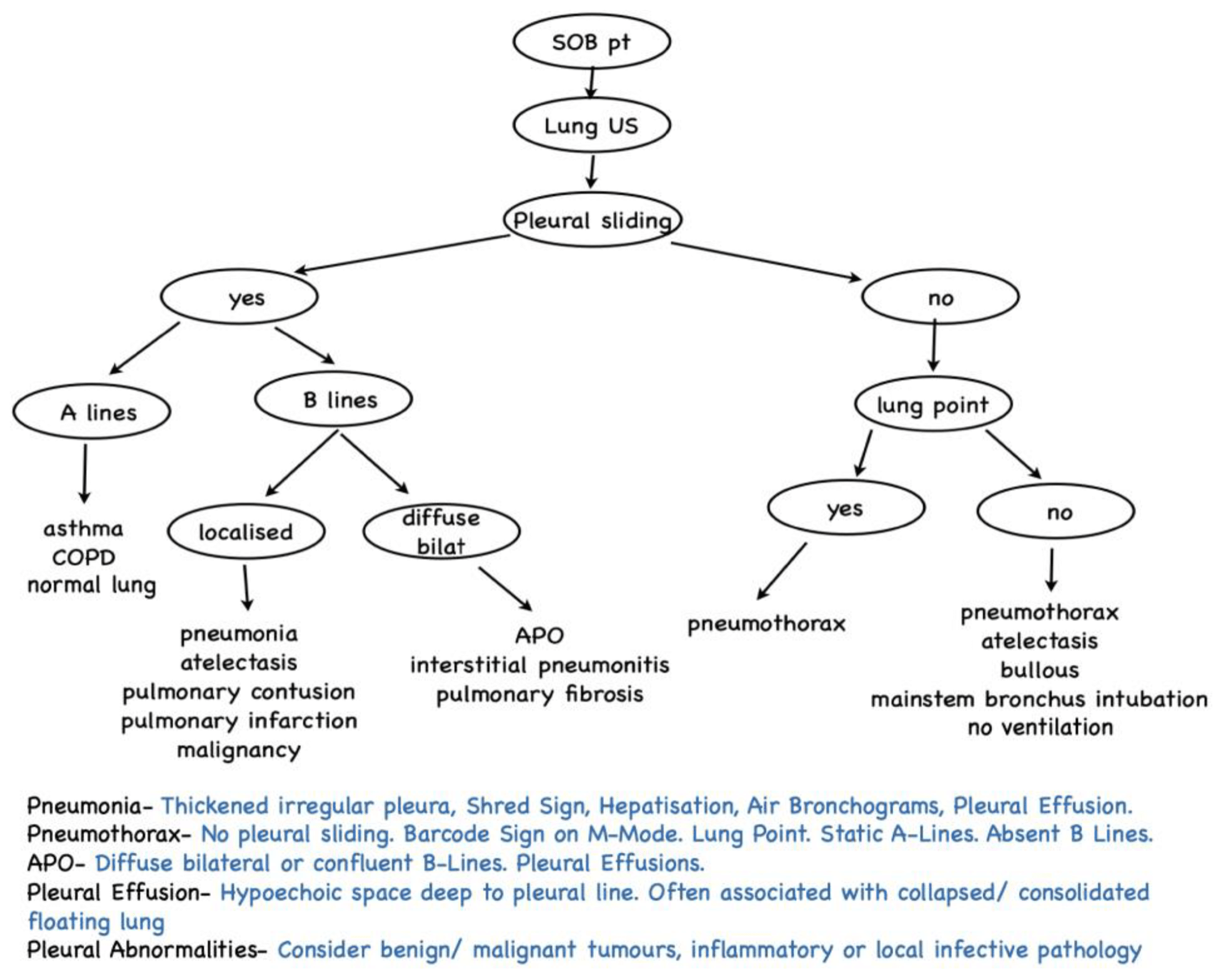
Ultrasound Features of Lung Pathologies
| Condition | Common Ultrasound Findings | Distribution / Behavior |
|---|---|---|
| Community-Acquired Pneumonia | Focal pleural-line abnormalities, multiple/confluent B lines (white lung), subpleural or lobular/segmental consolidations, air or fluid bronchograms. | Asymmetric and initially localized to specific lung areas. |
| Interstitial Pneumonia | Focal pleural-line abnormalities, multifocal B lines, white lung, multifocal subpleural consolidations. | Typically bilateral and inhomogeneous. Inflamed areas are often separated by fully aerated “spared areas”. |
| Pulmonary Edema | B lines that can progress to a white lung pattern. | Symmetric distribution, typically localized at the lowest points of the lungs due to gravity. Symmetric involvement of the 4 lower chest quadrants is pathognomonic for cardiogenic edema. |
| Pleural Effusion | Fluid collection in the pleural cavity. Relies on identifying the pleural cavity, diaphragm, and an abdominal organ (liver/spleen). The “spine sign” (visualizing the thoracic spine) indirectly indicates fluid. | Located at the lowest points due to gravity. Best assessed in a semirecumbent position. Can detect as little as 20 ml of fluid. Volume Estimation: . |
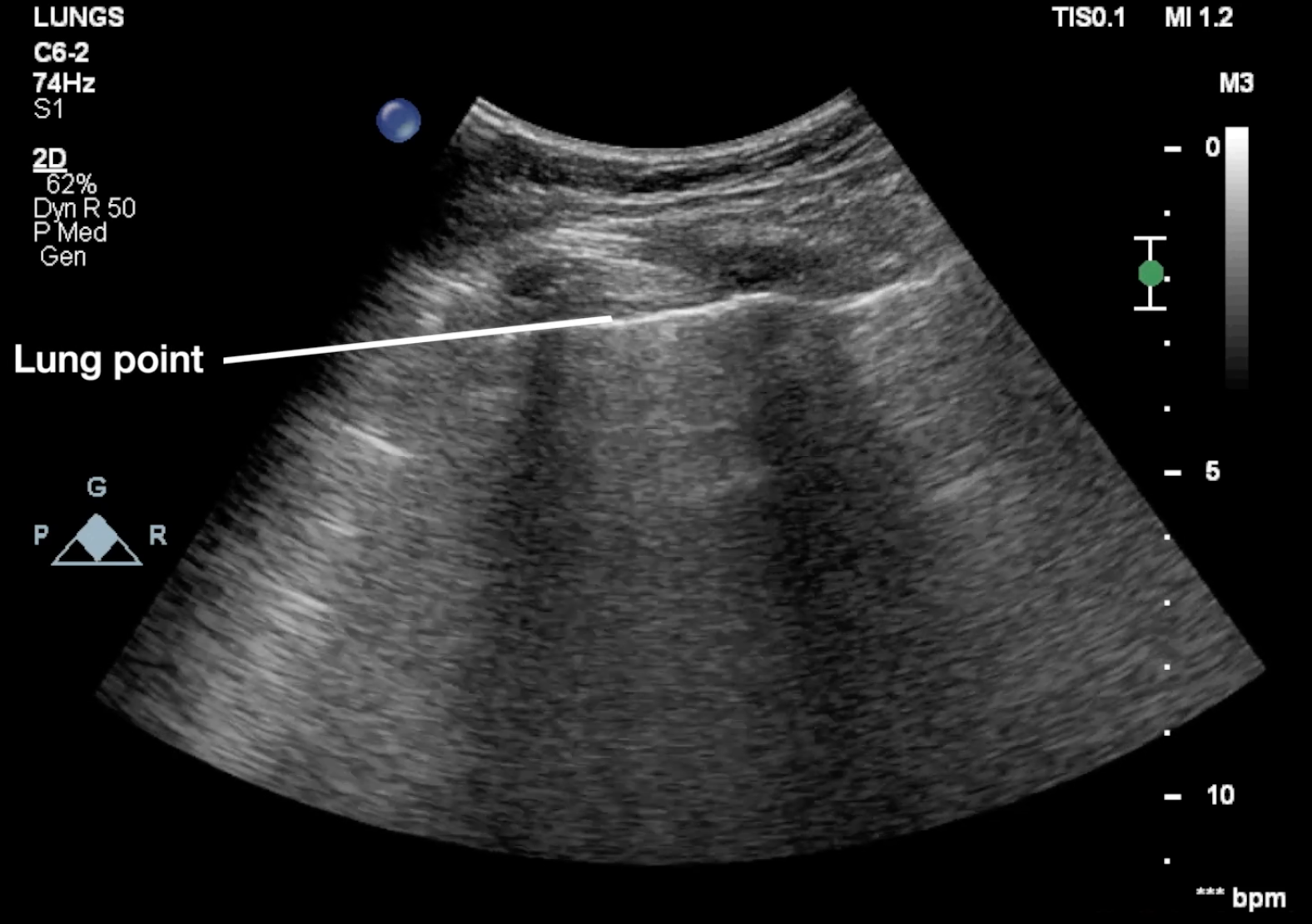
| Pneumothorax | Absence of lung sliding, absence of B lines/subpleural lesions, and absence of the lung pulse. • Seashore sign: Normal M-mode (resembles sea and sand). • Stratosphere / Barcode sign: M-mode signature of absent lung sliding. | ”Lung Point” is the only pathognomonic sign. It is the exact transient boundary where a healthy lung (with sliding) meets the pneumothorax (no sliding). |
| COPD & Asthma | Typically presents with completely normal lung ultrasound findings, acting as a diagnosis of exclusion. | Airway obstruction is diagnosed using M-mode to observe diaphragmatic kinetics (hyperechoic line rising on inspiration, falling on expiration). M-Mode Index of Obstruction: Ratio of excursion in the 1st second of forced expiration vs. total expiration. A value indicates an obstructive pattern. |
| Pulmonary Embolism | Limited diagnostic value; primarily a diagnosis of exclusion. May occasionally reveal oval, round, or wedge-shaped consolidations. | The Vascular Sign: Characterized by blood flow that cuts off proximally within the consolidation on Doppler. (Distinguishes it from inflammatory consolidations where blood flow spans the entire structure) . |
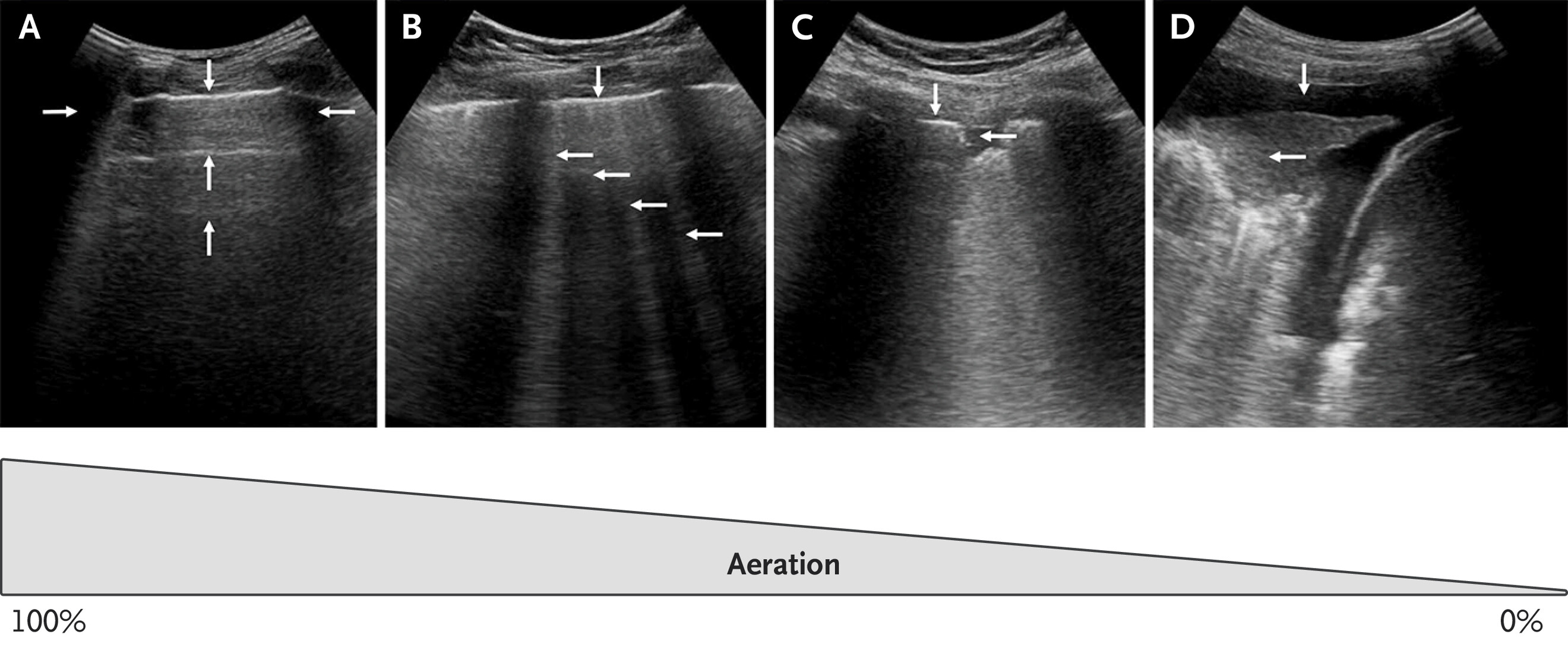
B-lines (interstitial Oedema)
- B-lines are thickening of the interlobular septum
- Appearance: Hyperechoic, laser-like vertical artifacts arising directly from the pleural line. They move in unison with lung sliding, travel all the way to the bottom of the screen, and erase A lines
- Clinical Significance: Healthy lungs may have 1–2 B lines per field. An increasing number signifies worsening edema. In severe cases, they merge to create a “white lung” pattern
- Increase depth to differentiate true B lines from Z lines (short, ill-defined, clinically irrelevant artifacts)
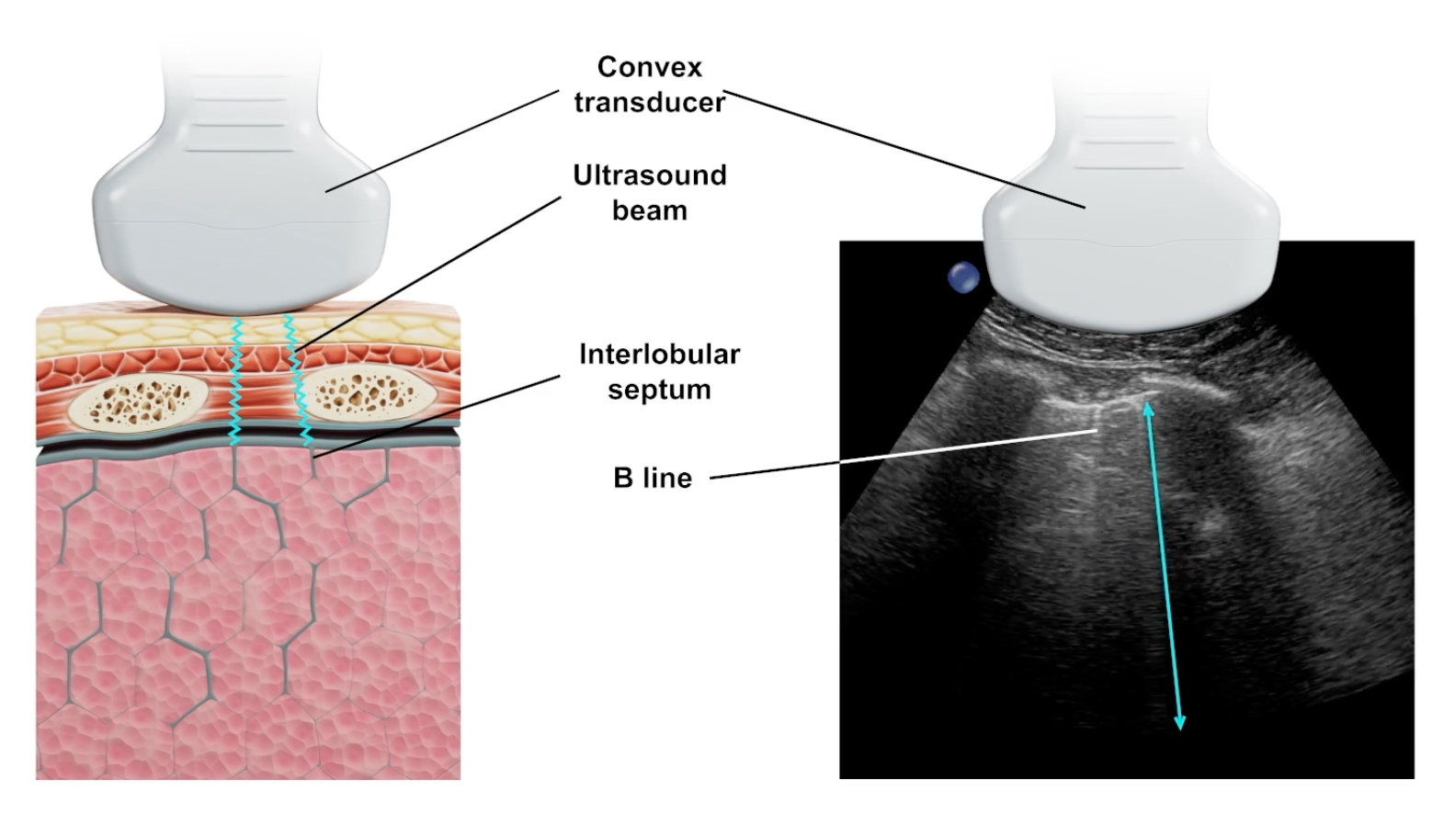
- Artefacts that do not extend from the pleural line may be as a result of subpleural consolidation
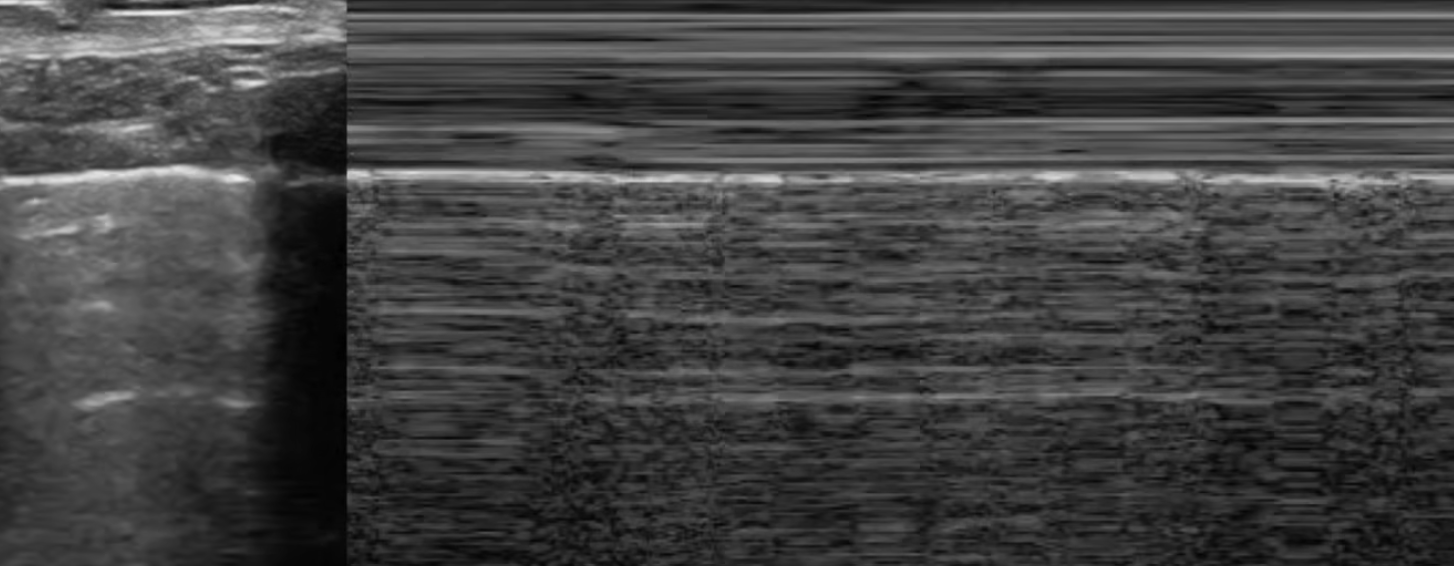
Sea Shore Sign
- Shows that lung sliding is present
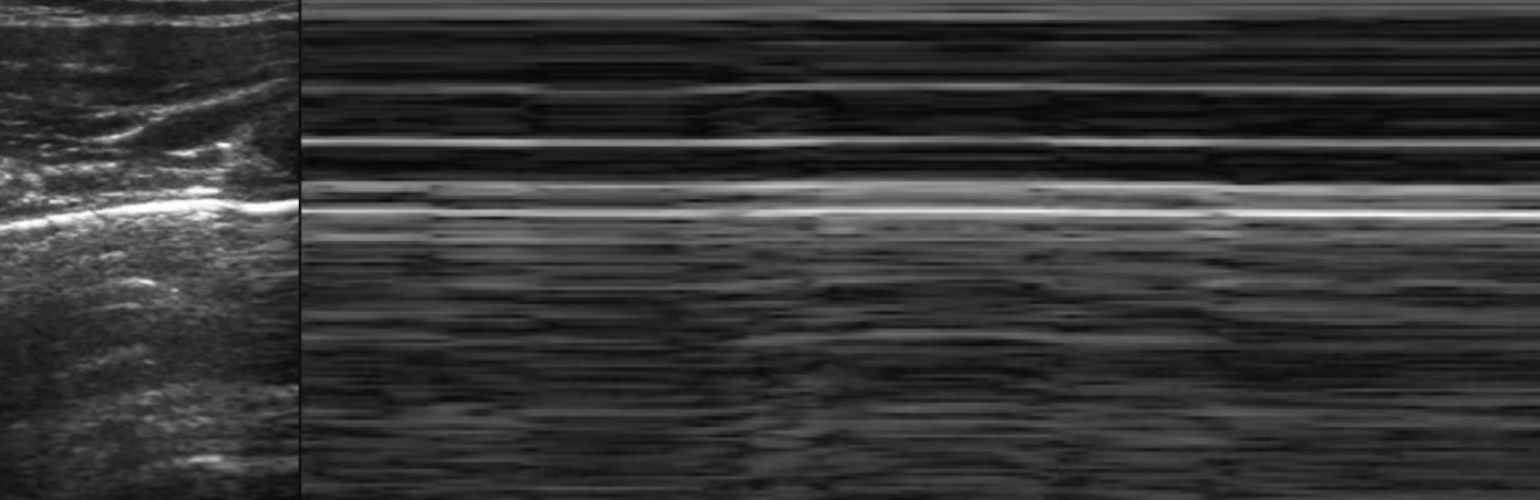
Barcode Sign
- Absence of lung sliding
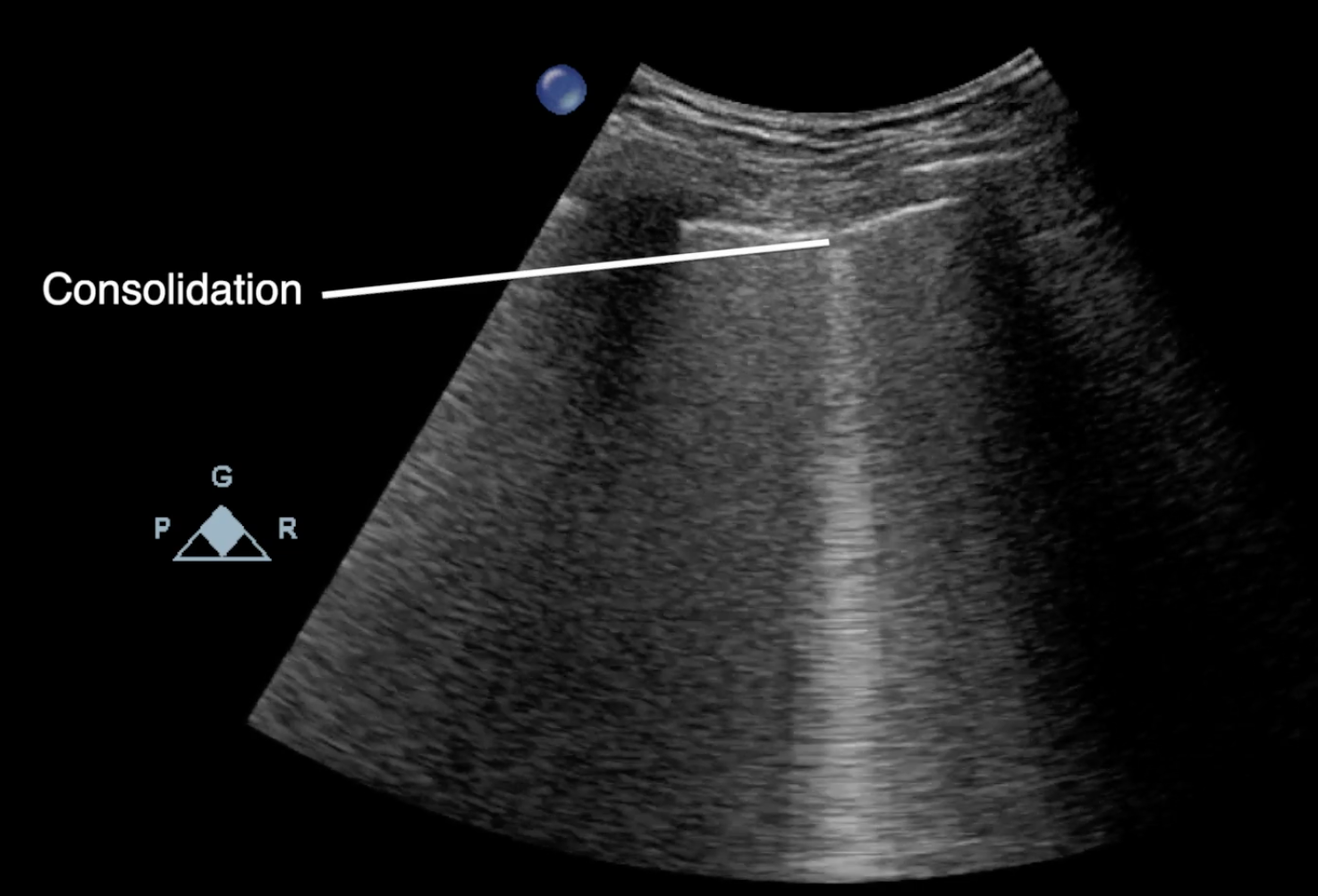
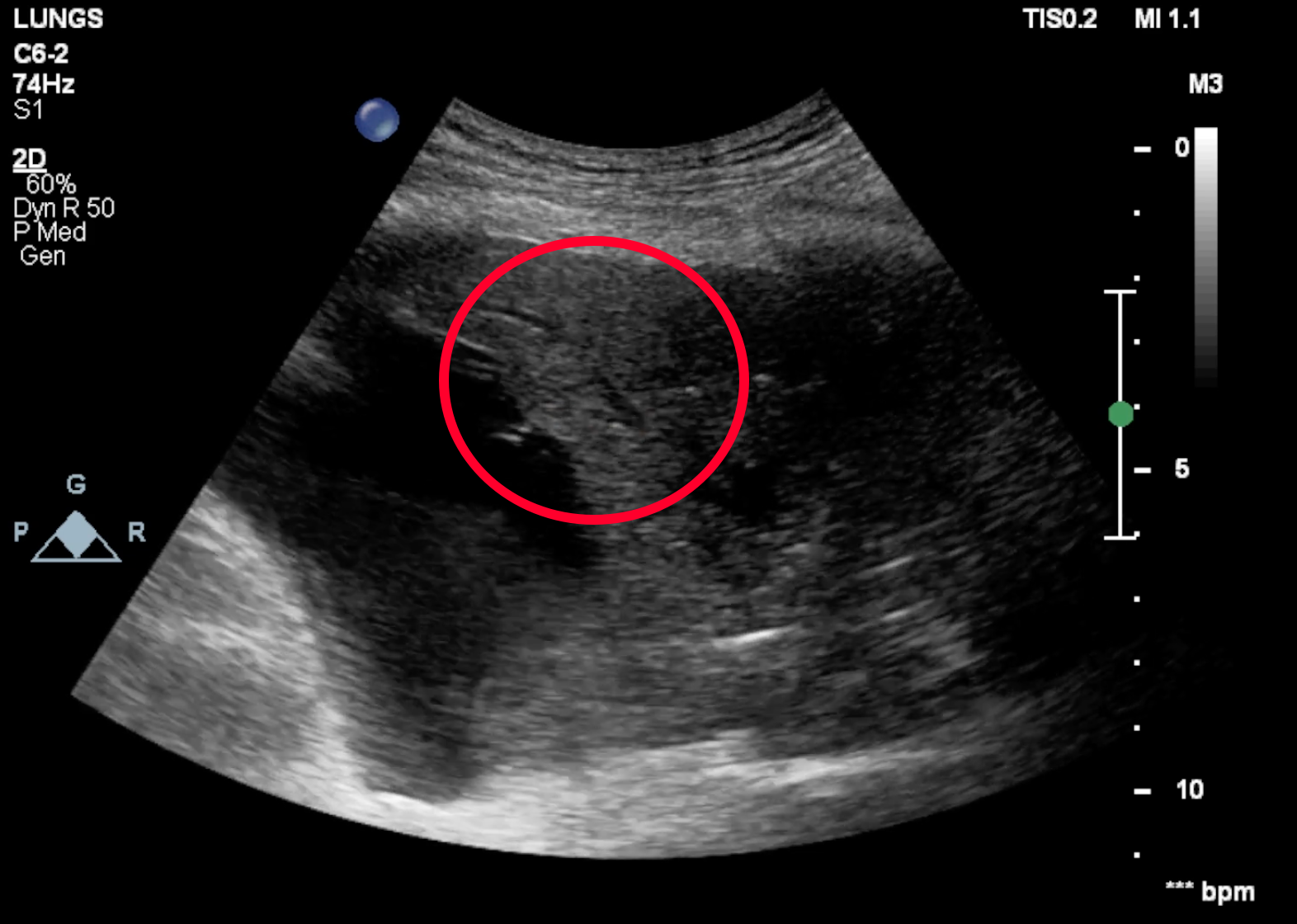
Community Acquired Pneumonia Findings
- Focal pleural line abnormalities
- Multiple B-lines
- Multifocal confluent B-lines
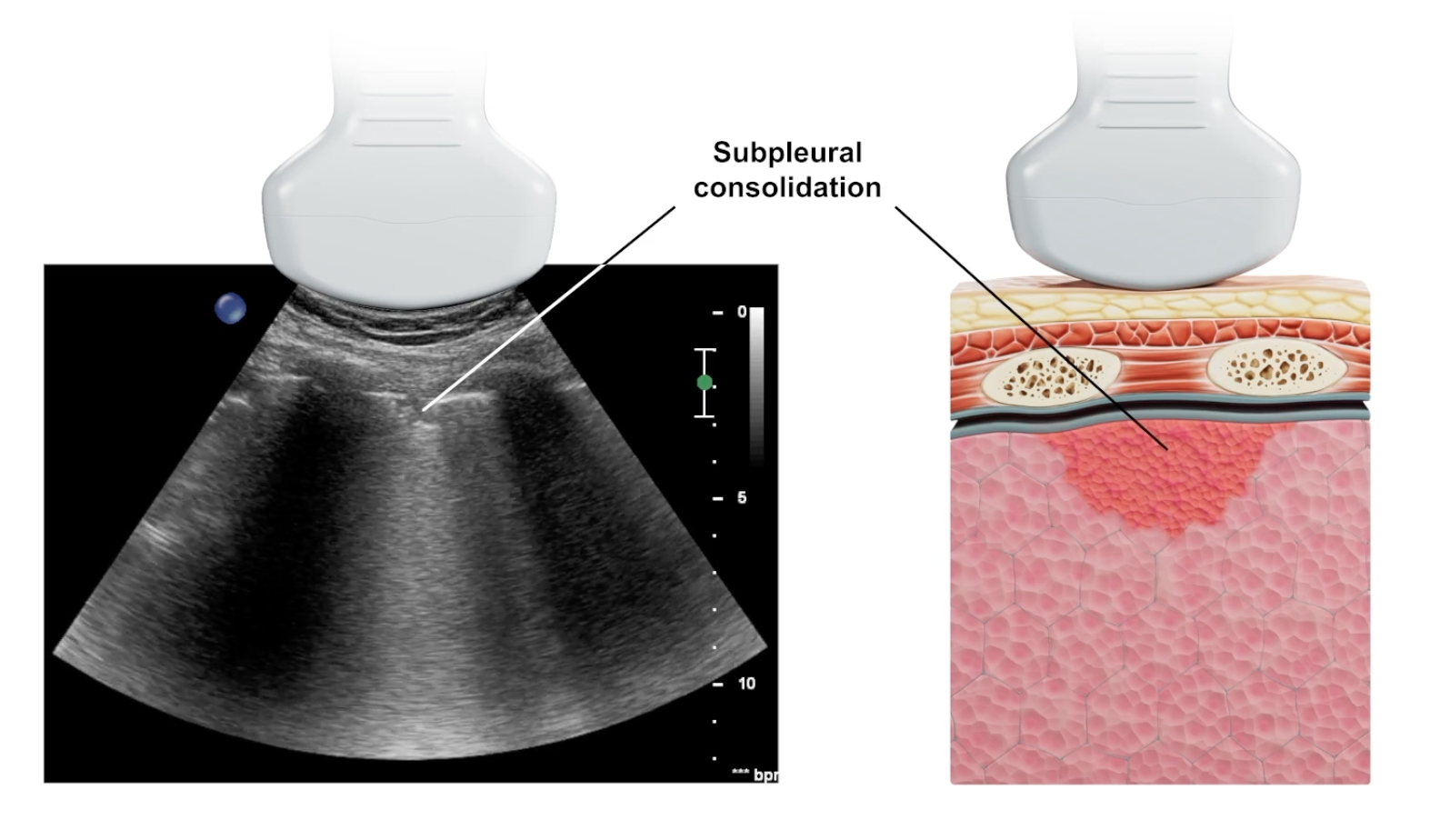
- Subpleural consolidations
- Lobular or segmental consolidation
- Air or fluid consolidations
Interstitial Pneumonia Findings
- Focal pleural line abnormalities
- Multifocal B-lines
- Multifocal confluent B lines
- Subpleural consolidations
Pulmonary Oedema Findings
- B lines across lower 4 quadrants
Pleural Effusion Findings
- Observe at lowest point
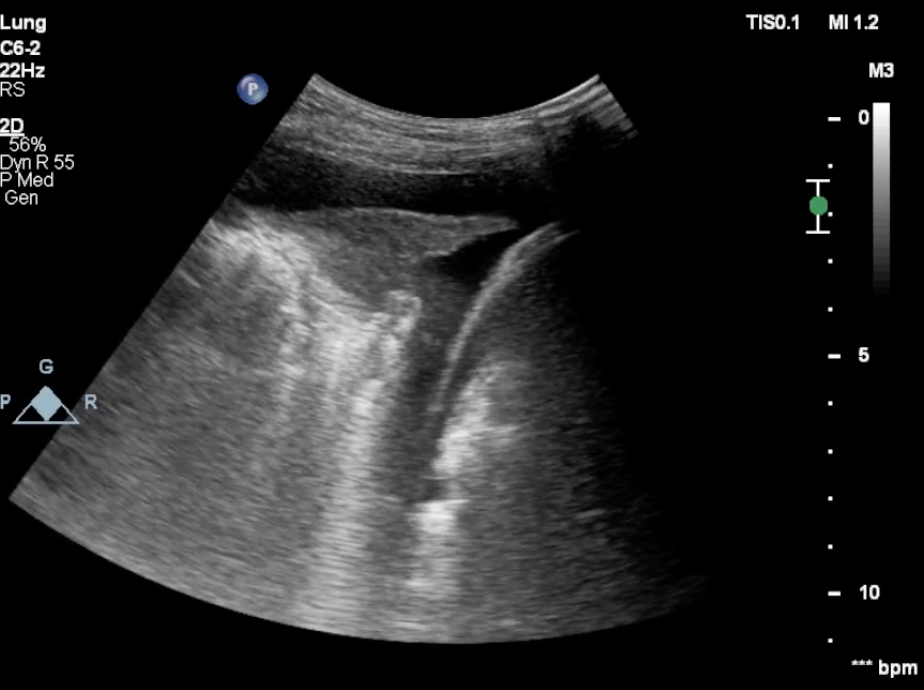
Pneumothorax Findings
- Absence of lung sliding
- Absence of B lines or subpleural lesions
- Absence of lung pulse
- Presence of the lung point
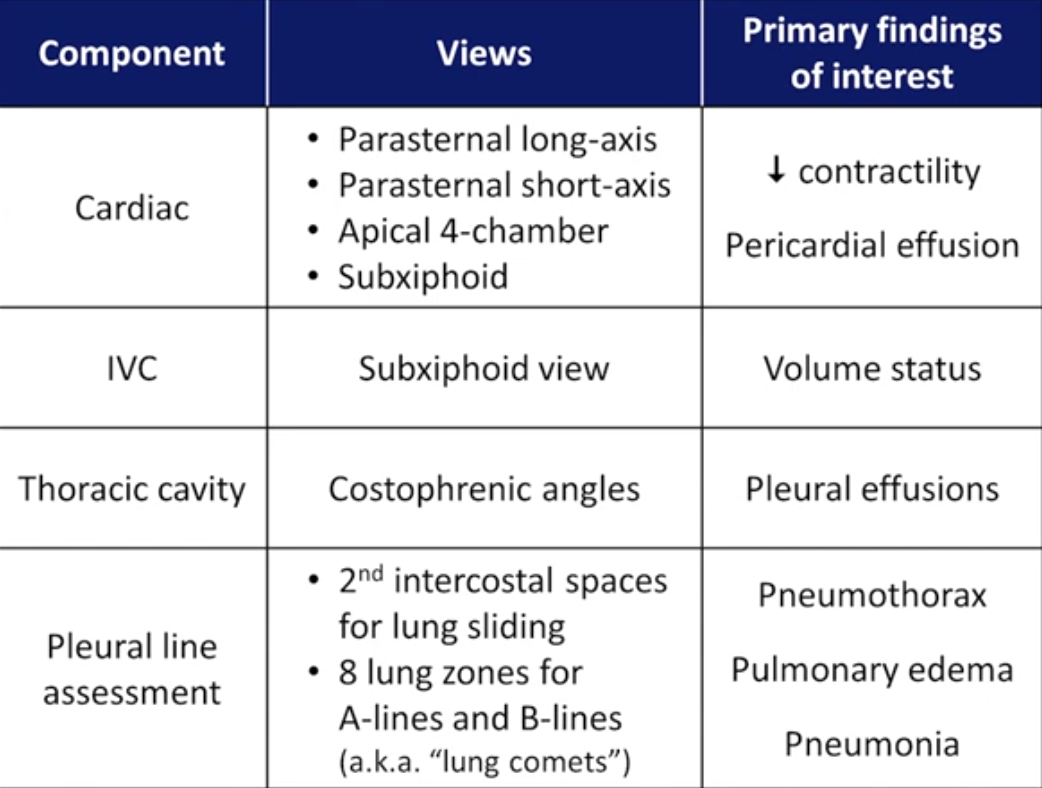
RADiUS Exam