WARNING
Note that mixed picture DKA and HHS can and do occur
Assessment
History
- Presentation: Dry, abdominal pain, polyuria, weight loss, coma
- Risk factors: non-compliance, illness, newly diagnosed
- Review of symptoms to rule find out possible precipitant (infection, MI, pneumonia, GI illness)
- Normal insulin regime
- Diabetic control
- Previous DKA / admissions
- Previous ICU admissions
Examination
- Assess volume status
- Assess for signs of a cause (e.g. infection)
- GCS
- Work of breathing
Investigations
- ABG
- Electrolytes
- Osmolality
- Urinalysis: ketones
- Pregnancy test
- Standard investigations to rule out cause: FBC, ECG, CXR
Severity Assessment
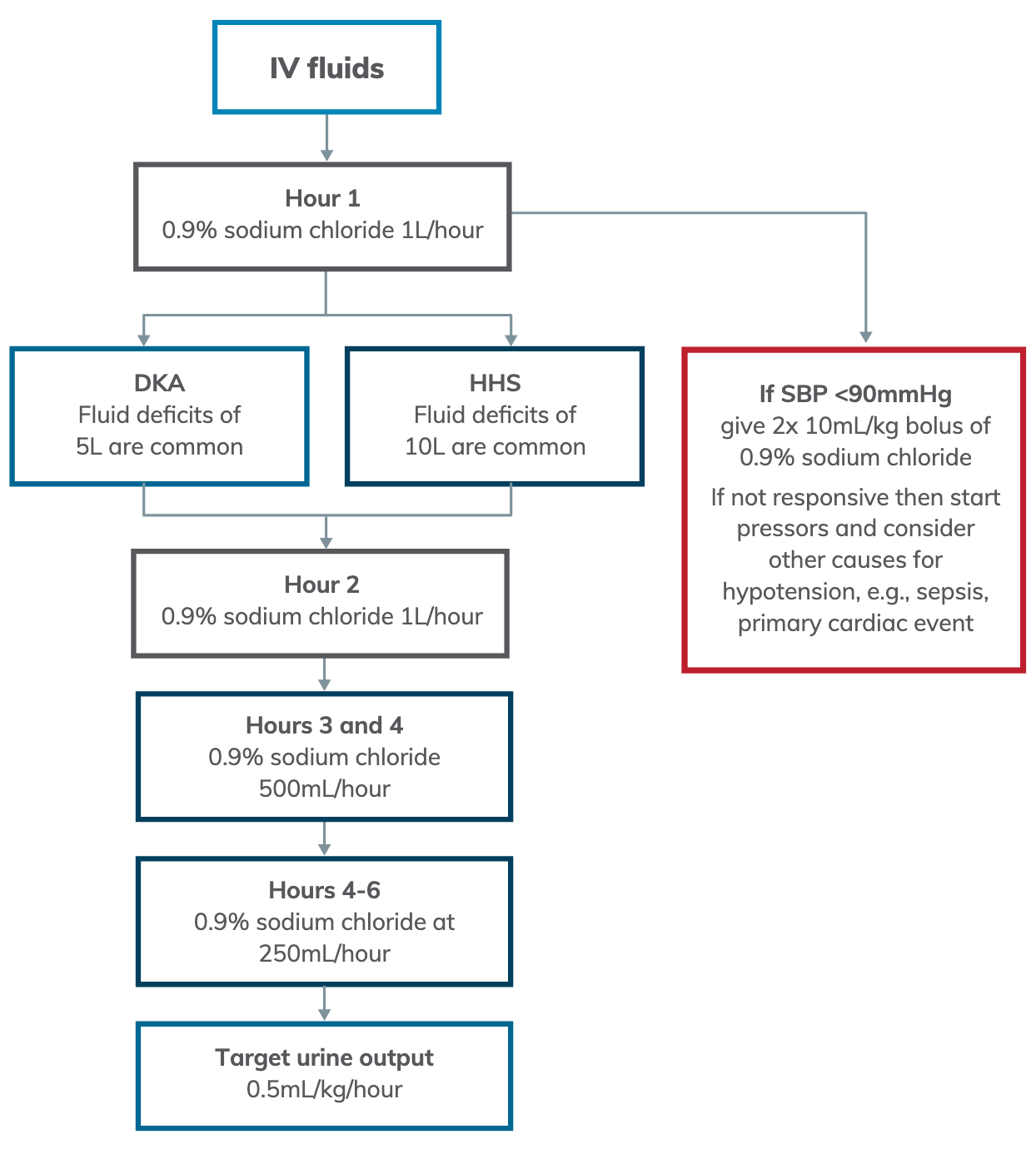
- The focus of DKA management is glucose management while the focus of HHS management is fluid replacement
| Parameter | DKA – Mild | DKA – Moderate | DKA – Severe | HHS |
|---|---|---|---|---|
| pH | 7.25–7.30 | 7.00–7.24 | <7.00 | >7.30 |
| Ketones (mmol/L) | 1.5–3 | >3 | >3 | <3 |
| HCO₃⁻ (mmol/L) | 15–18 | 10–14 | <10 | >18 |
| Osmolality (mmol/L) (calculated) | Variable | Variable | Variable | >320 |
| Blood glucose level (BGL) (mmol/L)† | >11 | >11 | >11 | >33 |
- †: Euglycaemic DKA can occur in pregnancy, in known T1DM, and in patients on SGLT2 inhibitors
- Calculation of osmolality can be performed using the following formula:
Management
WARNING
Intravenous insulin infusions are resource intensive and are potentially dangerous because of the rapid drop in potassium and/or glucose which can occur. If insulin infusions are commenced in the emergency department, use half dose insulin infusion rates (see flowchart) until the patient can be moved to the ICU or similar specialist area
- Goals of management:
- Establish precipitant and treat
- Assess severity of metabolic derrangement
- Cautions fluid resuscitation
- Insulin
- Replacement of electrolytes
- Monitor patients with:
- Hourly vital signs including a GCS
- Telemetry if replacing potassium quickly
Insulin Therapy
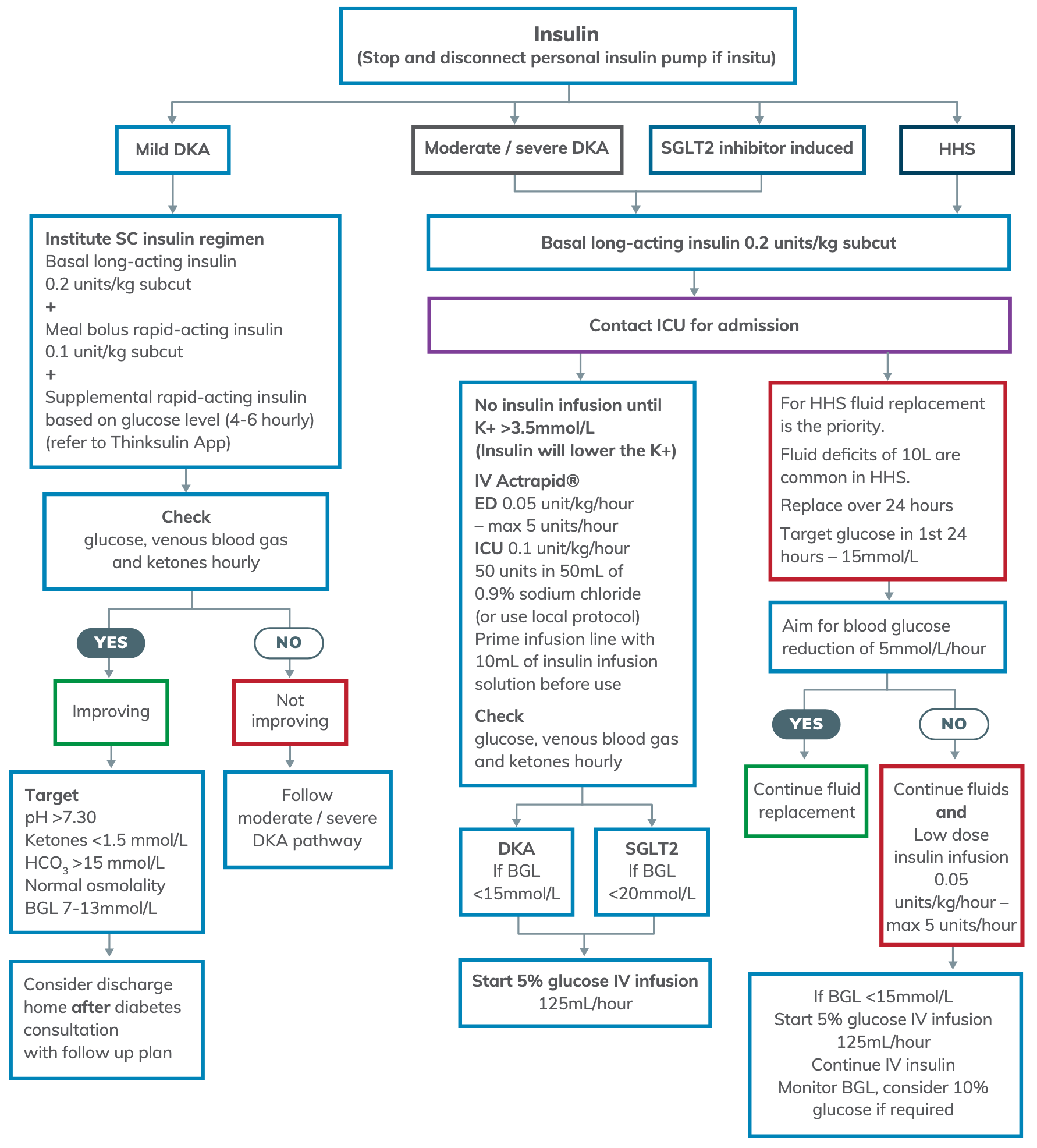
- Aim to lower BGL by 1-2 mmol/L/hr
- Correct osmolality by 3 mosmol/kg/hr
IV Fluid Replacement
Correct Sodium for Hyperglycaemia
Ensure correction of sodium for hyperglycaemia. Seek advice regarding fluid replacement if calculated sodium >145 mmol/L.
Potassium Replacement
- Check potassium levels 1-2 hourly; cardiac monitoring is often required
- If potassium level is:
-
5.5 mmol/L
- Do not give potassium
- 4.5-5.5 mmol/L
- Give 20 mmol in 1L 0.9% sodium chloride over 2 hours
- 3.5-4.5 mmol/L
- Peripheral access ⇒ 20 mmol in 1L 0.9% sodium chloride over 2 hours
- Central access ⇒ 20 mmol in 0.9% sodium chloride over 1 hour
- <3.5 mmol/L
- Do not start insulin until corrected
- Peripheral access ⇒ 20 mmol in 1L 0.9% sodium chloride over 2 hours
- Central access ⇒ 20-40 mmol in 0.9% sodium chloride over 1 hour
-
Supportive Management
- Magnesium <0.8 mmol/L ⇒ Replace with 10mmol over 4 hours IV
- Phosphate <0.32 mmol/L ⇒ Replace with 20mmol over 4 hours IV
- IV anti-emetic
- Assess and appropriately manage precipitating factors (e.g. MI, infection, overdose and non-adherence to insulin)
Sources
- ACI website:
- LITFL:
- IBCC: