Pathophysiology
- Hyponatraemia generally causes low extracellular osmolality causing fluid shift into the intracellular space
- This can cause cerebral oedema, precipitating the clinical features
- ADH acts primarily on water re-absorption and at a distal end of the nephron, and therefore can cause disorders of serum sodium concentration
- Angiotensin II, Aldosterone and ANP/BNP all cause same directional shifts in sodium and water reabsorption in the kidneys so it is unusual for disorders of these hormones to cause significant derangement in serum sodium concentration
- Severity classification:
- Mild 125-134
- Moderate 120-124
- Severe <120
Clinical Features
- Mostly neurological
- At sodium 125-130 when acute or sodium 120-125 when chronic:
- Fatigue
- Headache
- Nausea and vomiting
- At sodium 120-125 when acute or sodium 110-120 when chronic:
- Confusion
- Seizures
- Coma
- At sodium 125-130 when acute or sodium 120-125 when chronic:
- Presence and severity of symptoms are related to severity of hyponatraemia and speed of derangement (as indicated above)
Assessment
History
- Speed of onset more important than level; note that most patients won’t be symptomatic until Na+ < 125mmol/L
- Fluids status and losses
- Fluid intake/output
- Nausea
- Vomiting
- General symptoms
- Muscular weakness
- Headache
- Lethargy
- Neurological symptoms
- Raised ICP
- Seizures
- Coma
- Psychosocial history for suggestion of psychogenic polydipsia or weird diets
- Medications (diuretics, steroids, drugs which cause SIADH e.g. SSRIs)
- Also review the fluid chart (has someone been charting dextrose without interchanging with saline)
- Co-morbidities: adrenal disease, liver disease
- Trauma history suggesting cerebral salt wasting or pituitary injury
- Recent procedures: TURP, contrast CT, recent surgery etc.
- Social history: alcohol intake
Examinations
- Volume status
- Neurological complications (e.g. increased ICP, lateralising signs)
Investigations
- Standard bloods
- Plasma osmolality
- Plasma proteins and lipids
- Urinary sodium → here a high urine sodium suggests SIADH
- Urine osmolality
- Serum glucose level
- Optional extras to consider:
- ABG
- TFTs
- LFTs
- Urea and creatinine
- Random cortisol
- Short synacthen test
Workup
-
The main goals in the assessment of hyponatraemia are:
- Severity of hyponatraemia (correct for hyperglycaemia if present)
- Type of hyponatraemia (hypertonic/isotonic/hypotonic); although pretty much all hyponatraemia is hypo-osmolar
- Check urine osmolality
- Assess volume status and measure urinary sodium
- Consider additional tests
- Low uric acid or urea suggests SIADH or cerebral salt wasting
- Metabolic alkalosis + hypokalaemia suggests volume depletion from vomiting or diuretics
- Metabolic acidosis + hypokalaemia suggests volume depletion from diarrhoea
- Metabolic acidosis + hyperkalaemia suggests primary adrenal insufficiency
- Consider workup of SIADH causes if SIADH is likely
- Treat cause
- Prevent complications
-
Remember to correct serum osmolality for the effect of urea
- Urea is an ineffective osmole (as it freely crosses cell membranes) → therefore does not cause H2O to moved out of cells
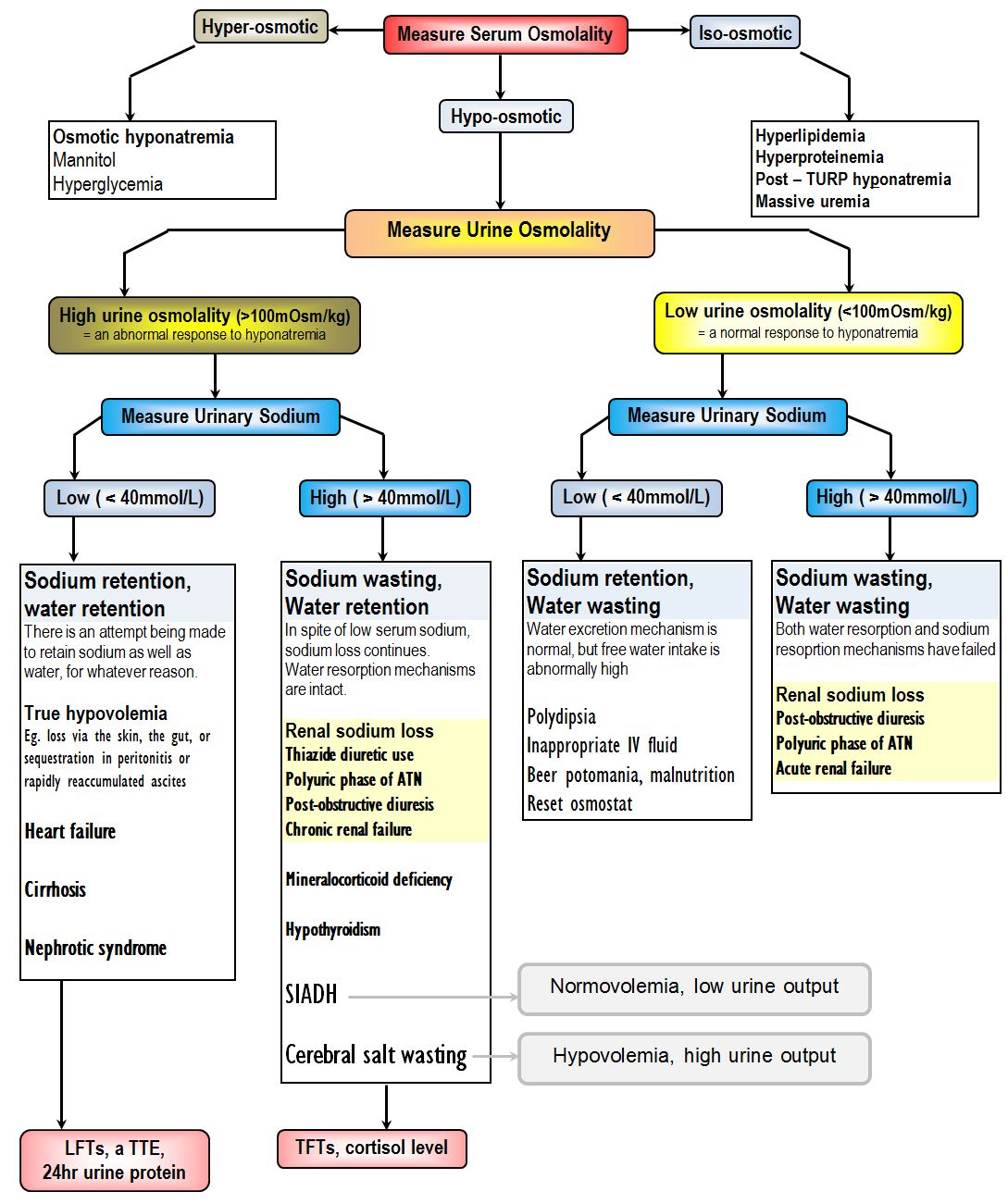
Hypotonic
- The main causes here are either caused by solute depletion or dilution and are differentiated by the volume status or by urine studies
- Hypo-osmolar urine
- Low urine sodium
- Dilutional hyponatraemia; the kidney is trying to pass free water to concentrate extracellular fluid
- Water excess: psychogenic polydipsia, inappropriate fluids (i.e. 5% dextrose)
- Dietary solute deficiency (beer potomania, malnutrition e.g. ovolactovegetarians, crash dieters, elderly “tea and toast” diet)
- Minimum urine osmolality ~40–60 mOsm/kg — kidney cannot dilute below this; therefore and with a normal diet this is up to 10-15 L/day
- With a low protein and ow sodium diet, there is less urea production and less sodium is available for excretion
- As the solute load falls the maximum water excretion decreases sometimes down to ~4 L/day
- Excess water intake beyond this results in dilutional hyponatraemia
- Management here is to increase solute intake and fluid restrict
- High urine sodium
- Normal mechanisms of water resorption and sodium retention have failed
- Acute Renal Failure
- Sodium reabsorption failure — damaged tubules can’t reclaim Na⁺ from the lumen
- ADH unresponsiveness — collecting duct can’t concentrate urine even if ADH is present
- Reduced flow delivered to distal nephron compounds both problems
- Above result in small volume of dilute, sodium rich urine
- Post obstructive diuresis
- Polyuric phase of Acute Tubular Necrosis
- Low urine sodium
- Hyper-osmolar urine
- Low urine sodium
- Hypovolaemia in patients who have extracellular fluid losses (e.g. diarrhoea, vomiting, burns, blood loss, third spacing into post-laparotomy abdomen)
- Manage with just normal saline
- Hypervolaemia where the renin-angiotensin-aldosterone system is activated inappropriately
- Heart Failure results in decreased salt delivery to macula densa activating the renin-angiotensin-aldosterone system
- Cirrhosis with ascites where the blood pressure is low due to systemic vasodilation despite a hyperdynamic circulation thereby activating the renin-angiotensin-aldosterone-system
- Nephrotic syndrome where fluid leaving the intravascular compartment results in reduced effective circulating volume thereby activating the renin-angiotensin-aldosterone-system
- Hypovolaemia in patients who have extracellular fluid losses (e.g. diarrhoea, vomiting, burns, blood loss, third spacing into post-laparotomy abdomen)
- High urine sodium
- Thiazide diuretics
- Polyuric phase of Acute Tubular Necrosis
- Chronic Renal Failure
- In chronic renal failure, urine osmolality tends towards 300 mOsm/kg (isothenuria) where the kidney is neither adding nor removing water effectively, so urine ends up isotonic to plasma
- This is because of the loss of the corticomedullary osmotic gradient
- Tubules faile to retain sodium also resulting in sodium wasting
- In chronic renal failure, urine osmolality tends towards 300 mOsm/kg (isothenuria) where the kidney is neither adding nor removing water effectively, so urine ends up isotonic to plasma
- Corticosteroid deficiency (e.g. Addison disease)
- Loss of aldosterone causes decreased sodium resorption and increased potassium retention thereby causing hyponatraemia and Hyperkalaemia
- Cortisol itself inhibits ADH secretion meaning less cortisol results in water retention due to more circulating ADH causing concentrated high sodium urine
- Exogenous corticosteroids resolves this issue
- Hypothyroidism
- Pan-hypopituitarism
- SIADH
- Elevated vasopressin causes water retention and dilutional hyponatraemia but sodium excretion remains intact, hence the high urinary sodium
- Cerebral salt wasting
- These patients are hypovolaemic and produce high urine output in contrast to SIADH patients who are normmovolaemic and have low urine output
- There is an inappropriate inhibition of sodium reabsorption in the kidneys resulting in volume depletion
- Here ADH is elevated as an appropriate response to hypovolaemia
- Fluid restriction will improve SIADH but worsen cerebral salt wasting
- Isotonic saline improves cerebral salt wasting but has no effect on SIADH
- Low urine sodium
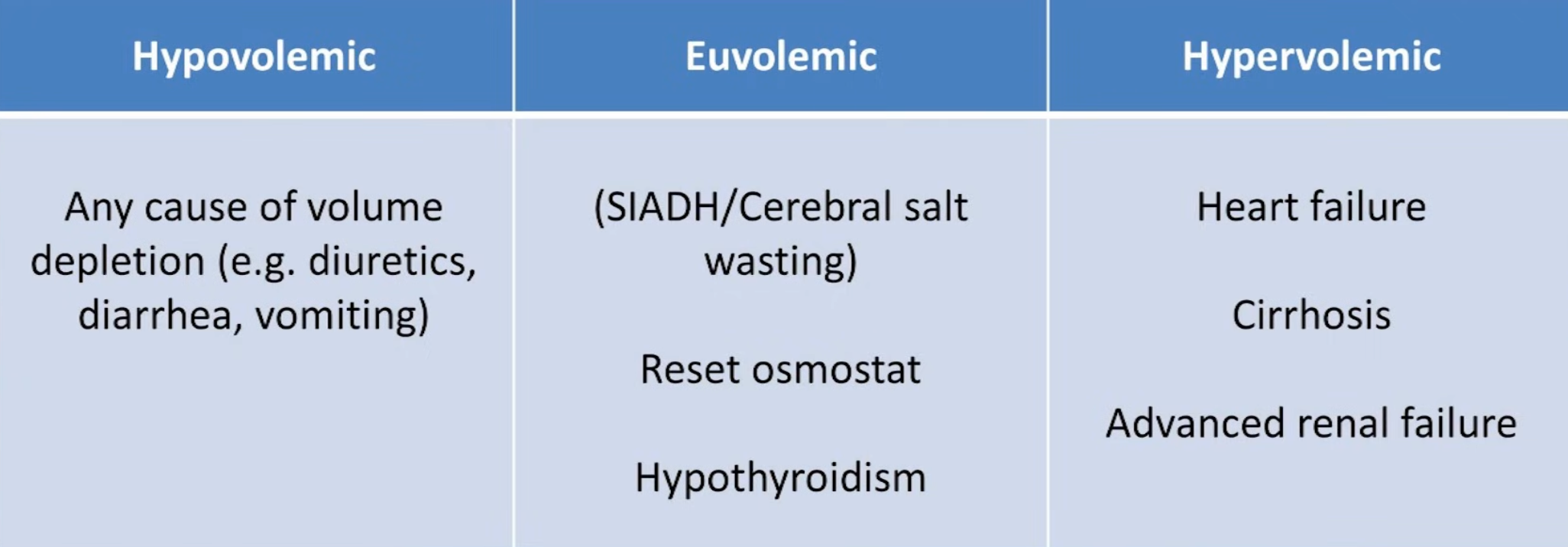
- Determine volume status
- Hypovolaemic: Loss of and sodium from the extracellular fluid space → ↑ ADH secretion → ↓ free excretion and retention → hyponatraemia
- Intra-renal causes: ACE-i, Diuretics, Addison disease, Cerebral sodium wasting syndrome, Acute Tubular Necrosis → would expect urine sodium to be high > 20 mmol/L
- Extra-renal causes: vomiting, diarrhoea, dehydration, burns, bleeding → would expect urine sodium to be low < 10 mmol/L
- Euvolaemic (usually because of limited free water excretion)
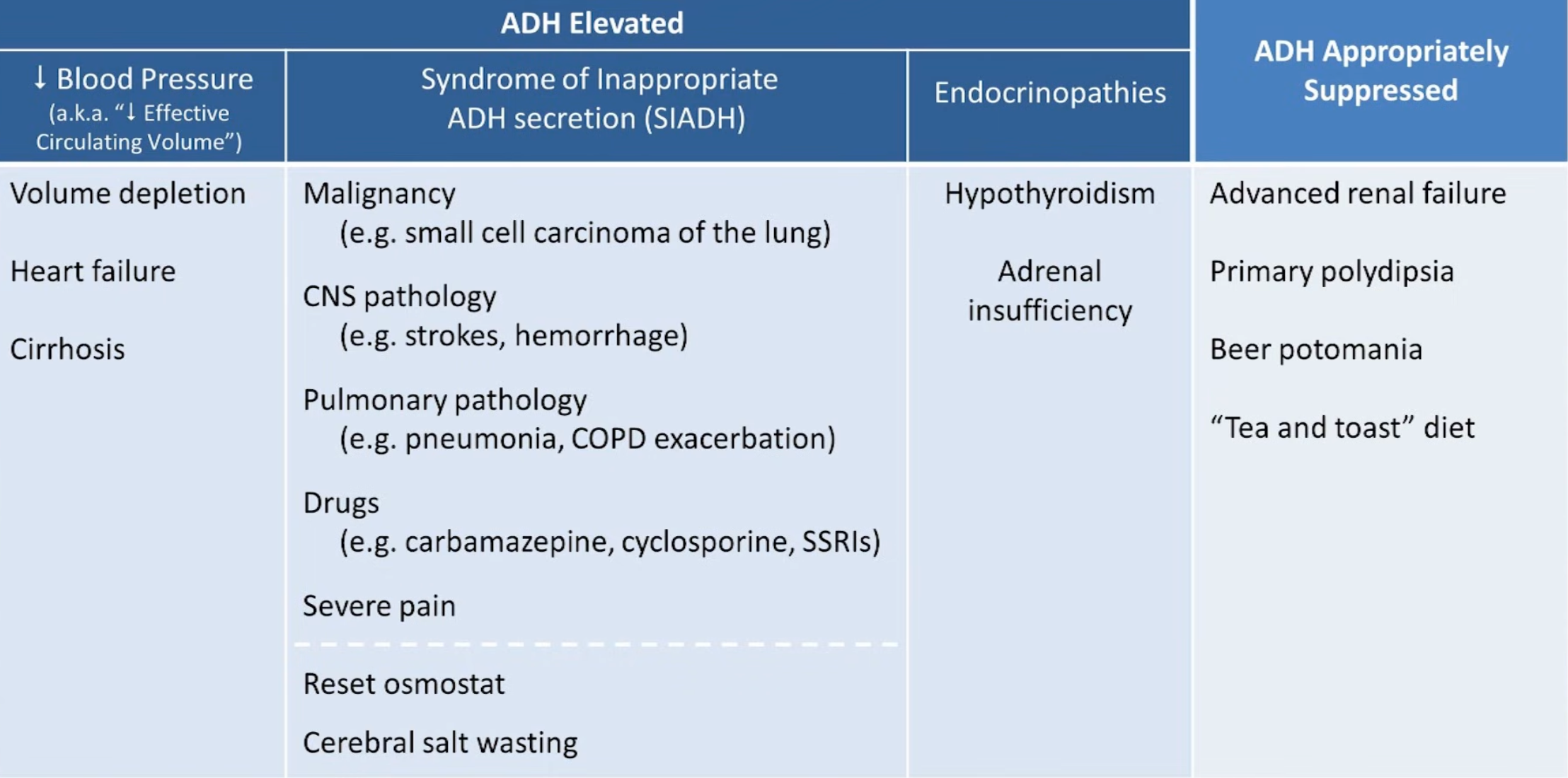
- SIADH (causes of SIADH can be remembered with MAD CHOP: malignancy, ectopic ADH secretion, Drugs (e.g. SSRIs), CNS disease, hormone deficiency (Hypothyroidism, Adrenal Insufficiency), others, pulmonary)
- Hypothyroidism
- Psychogenic polydipsia
- Iatrogenic SIADH (SSRIs, carbamazepine)
- Beer potomania
- Hypervolaemic (fluid overload state)
- Congestive heart failure
- Cirrhosis
- Nephrotic syndrome
- End stage renal disease
- TURP/hysteroscopy syndrome
- Acutely TURP syndrome can present with isotonic or hypertonic picture with high osmolar gap before the glycine is metabolised as glycine itself is osmotically active; Once metabolised to ammonia or glyxoxylate and the true hypotonic hyponatraemia is unmasked
- Hypovolaemic: Loss of and sodium from the extracellular fluid space → ↑ ADH secretion → ↓ free excretion and retention → hyponatraemia
Isotonic
- Referred to as pseudohyponatraemia as it is due to a measurement artifact
- In the lab, the sample is diluted to 1/10th the solution then the sodium is measured
- The concentration of sodium is then calculated with the assumption that it comes from a sample which originally consisted of 93% water
- Hyperlipidaemia, multiple myeloma ⇒ pseudohyponatraemia because of reduction in aqueous plasma
Correcting sodium for high lipids (lipid concentration measured in mg/dL) or proteins (protein concentration measured in g/L) is possible with the following formula
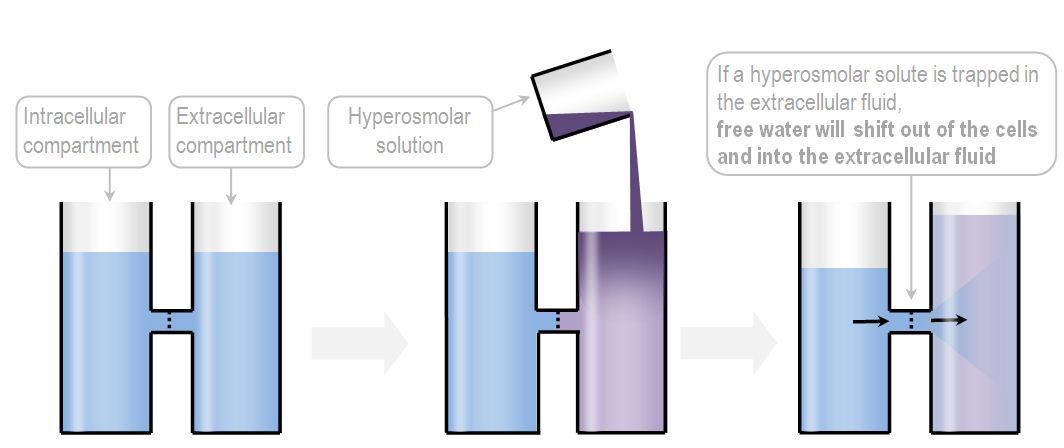
Hypertonic
- Osmotically active particles in the plasma induce movement of from intracellular to extracellular space decreasing serum sodium conentration even through the serum osmolality remains elevated
- Mannitol; although this turns into Hypernatraemia as mannitol is a free-water-sucking osmotic diuretic
- Alcohol intoxication can cause hyperosmolarity and thus hyponatraemia but the inhibition of ADH by alcohol leads to massive diuresis and dehyudration and typically hypo-osmolar hyponatraemia
- Radiocontrast use
- Highly osmotic agents cause increase in water osmosis into intravascular space causing dilutional hyponatraemia
- Calculate corrected sodium for hyperglycaemia
A linear equation can be used but it tends to be inaccurate once the BGL goes above 25
Alternatively can remember that at:
- A BSL of 14, the sodium decreases by 4 mmol/L
- A BSL of 28, the sodium decreases by 8 mmol/L
- A BSL of 56, the sodium decreases by 16 mmol/L
Hence we start to use this formula for higher BGLs
Management
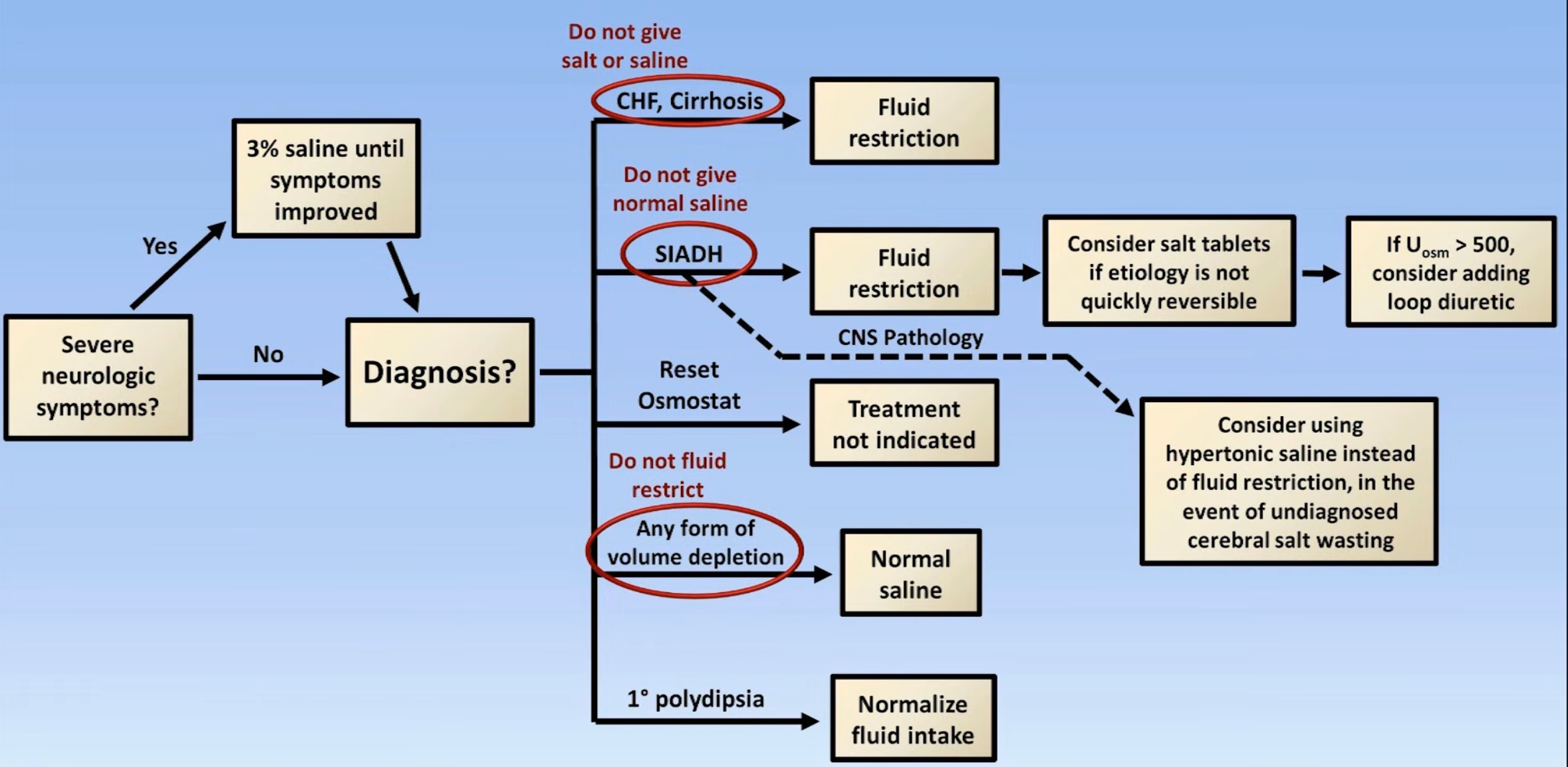
- Recommendation for rise:
- Correct rate of ≤6 mmol/L over the first 24 hours
- In the presence of severe neurological symptoms increase the sodium immediately in the first few hours until symptoms improve then hold for the remainder of the day
- Fluid restriction to <800 mL/day
- Diuretics
- Isotonic saline in true volume depletion
- Oral sodium tablets
- Can consider hypertonic saline
- Desmopressin or dextrose if inadvertent rapid correction takes place
Acute and Symptomatic
- i.e. patient is seizing or comatose
- Raise by 1-5 mmol/hr until symptoms resolve or 125-130 mmol/L
- Hypertonic saline 3% 1-2 mL/kg/hr; can consider rapid reversal with 100mL q10 minutes until seizure stops
- Furosemide 20mg IV
Chronic symptomatic
- More than 48 hours of hypontraemia or of unknown duration
- Calculate the sodium deficit and correct by 10 mmol/L/day’ (refer to calculations section of Hyponatraemia • LITFL • CCC Electrolytes)
- Furosemide 20 mg IV
- Fluid restrict
- Repeat sodium every 2 hours
Fluid Restriction
- Management of choice in euvolaemic and hypervolaemic hyponatraemia (e.g. SIADH, CCF, cirrhosis, nephrotic syndrome, psychogenic polydipsia, beer potomania)
- May not work where:
- High urine osmolality
- Low urine output
- Sum of urinary sodium and potassium concentration exceeds the serum sodium concentration
- After 2 days of fluid restriction, the sodium concentration has failed to increase by more than 2 mmol/L
Isotonic Saline Replacement
- Management of choice in hypovolaemic hyponatraemia as the hyponatraemia is due to increased ADH due to low circulating volume
- Once volume is corrected, the stimulus for ADH secretion will cease and tonicity will be restored by diuresis
- In summary:
- Hypovolemia has resulted in excess ADH release in spite of hypo-osmolarity, because the baroreceptor reflex is a stronger stimulus for ADH release than the osmoreceptor reflex
- The excess ADH results in free water retention, which counteracts the attempts to increase sodium concentration with hypertonic saline
- Once volume is restored, ADH release will decrease, and dilute diuresis will ensue
- This loss of free water will assist the attempts to correct hyponatremia with hypertonic saline
- Thus, volume replacement must occur together with sodium replacement
- Initial infusion rate can be calculated by:
Hypertonic Saline Replacement
- Symptomatic hyponatraemia should be managed with the infusion of hypertonic saline
- Initial infusion rate can be given by:
- For example for a 100kg man with a sodium of 110 mmol/L, what is the desired rate of 3% saline to increase the sodium to 113 mmol/L over 6 hours
Asymptomatic from SIADH
- Fluid restrict
- Furosemide 20-40mg/day
- tablets 3-18g/day
- Urea 30g/day
- Demclocycline 600-1200mg/day
Sources
- Youtube videos
- LITFL:
- Deranged Physiology: