Do not neglect airway issues and place heavy importance of suctioning if relevant (e.g. aspiration, mucous plugging)
Use supplemental oxygen in all hypoxic patients with high-flow oxygen at 15 L/min through a mask with a reservoir, (target oxygen saturation > 90-92%)
High inspired oxygen concentrations do not depress ventilation in patients who are in respiratory distress
In patients with COPD who chronically retain COX2 titrate use of a venturi mask
Giving too much oxygen to patients who chronically retain COX2 causes a rise in PaCOX2 because:
Changes in pulmonary vasoconstriction, dead space and shunting (V/Q mistmatch)
Haldane effect (haemoglobin molecules release COX2 in the presence of oxygen)
Blunting of the hypoxic drive; these patients depend on mild hypoxia to stimulate their respiratory centre
If unsure if they are a chronic retainer, check any previous blood gas results
Begin empirical OX2 treatment under pulse oximetry monitoring
Increase/decrease oxygen delivery until OX2 saturation is 88-92% by using different oxygen mixers in a venturi mask or changing the flow rate in a simple mask
Recheck blood gases and watch for a change in PCOX2:
Continue with current therapy if COX2 is normalising
Decrease oxygen deliver if COX2 is increasing but maintain OX2 saturation of 88-92%
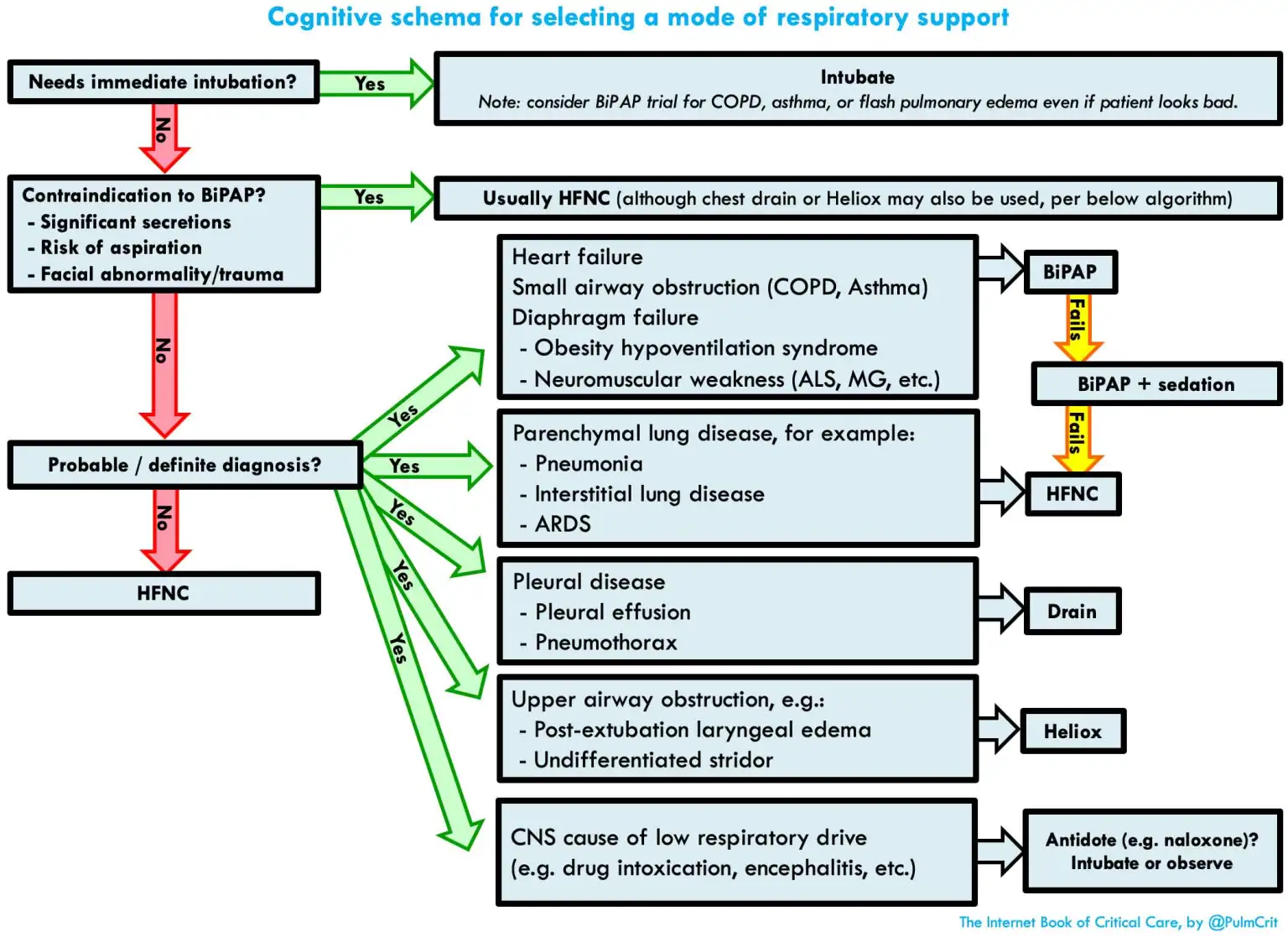
If COX2 is increasing and you are unable to maintain oxygen saturation >88%, the patient requires assisted ventilation (BiPAP) see ventilation below
Blood gases are necessary to determine the adequacy of ventilation (can use either venous or arterial as it will likely not influence immediate management) - see ABG Interpretation
If wheezing, consider bronchodilators (see: COPD Exacerbation) perhaps nebulised
Rule out tachy-arrythmia or demand related ischaemia if you can prior