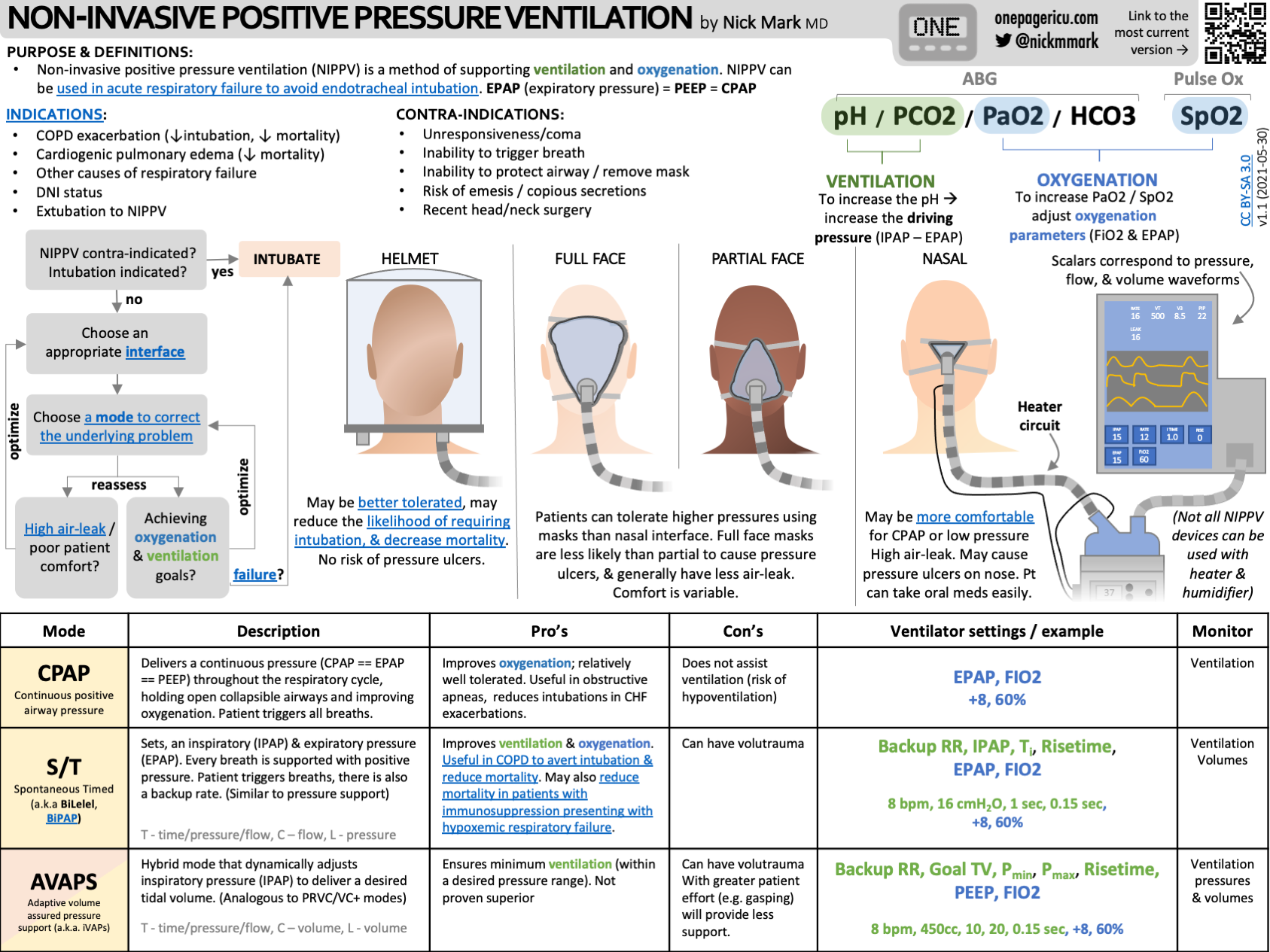
Definitions
- CPAP
- Maintains alveolar recruitment and improves pulmonary shunting
- Improves predominantly oxygenation and therefore indicated in type 1 respiratory failure
- BiPAP
- S/T mode refers to spontaneous and timed mode and therefore has a backup rate
- The use of ventilator-triggered breaths in acute respiratory failure while on NIV is questionable; if the patient doesn’t have a good respiratory rate perhaps they should be intubated
- S mode refers to spontaneous (only)
- S/T mode refers to spontaneous and timed mode and therefore has a backup rate
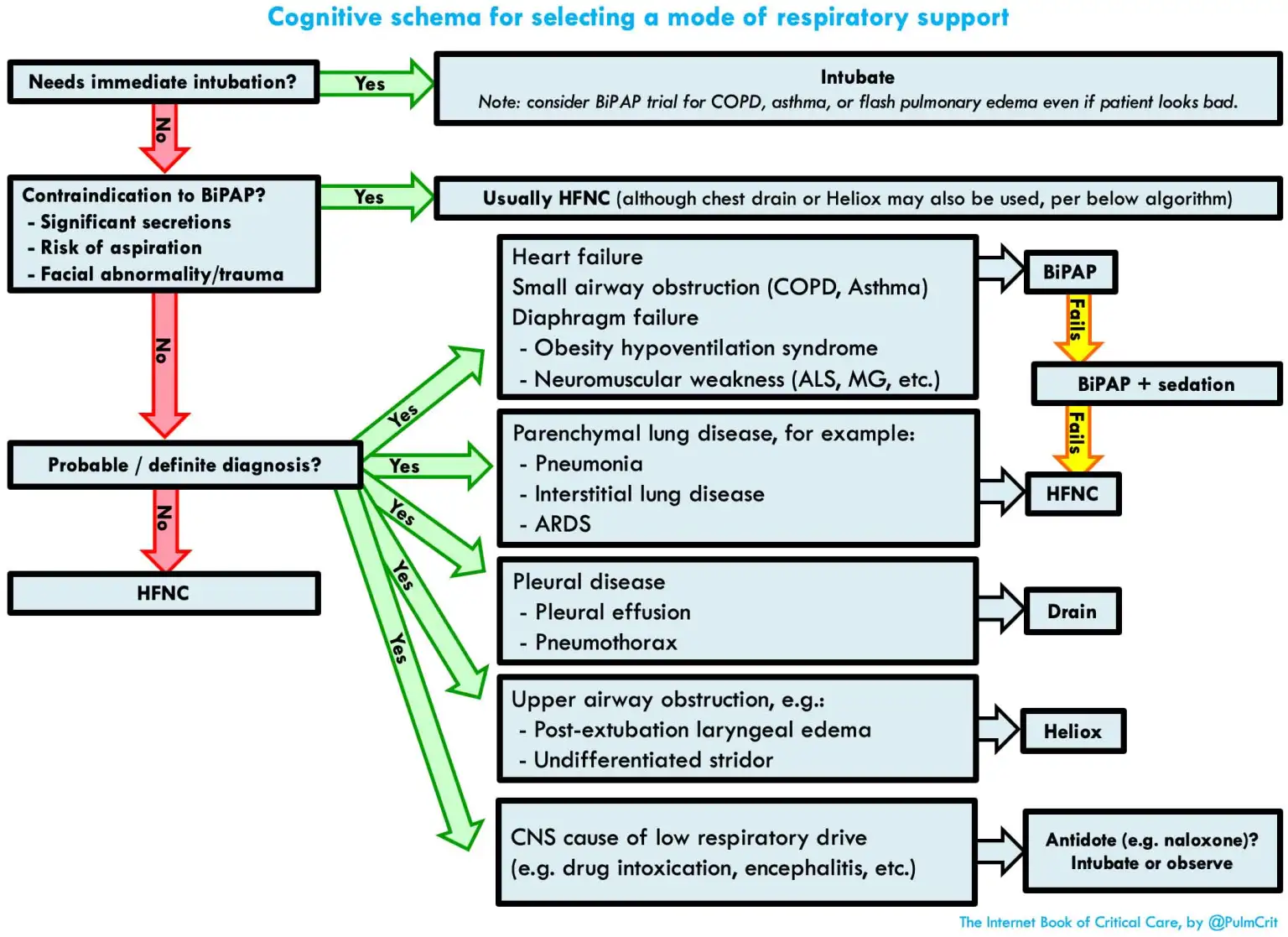
Indications
- Acute hypercapnic respiratory failure secondary to COPD exacerbation, neuromuscular disease, obesity hypoventilation syndrome
- Patients with COPD and a pH < 7.26 or a reduced level of consciousness are at greater risk of failing NIV and require closer monitoring
- Acute Pulmonary Oedema
- Immunocompromised patients with acute respiratory failure
- Acute pneumonitis (including COVID-19) with acute respiratory failure with / > 150 mmHg
- In moderate-to-severe hypoxaemia with / ≤ 150 mmHg, delayed intubation can increase mortality and so NIV should only be applied in context of the ability to closely monitor
- Weaning high-risk patients from mechanical ventilation
- Post extubation management
- Post-operative acute respiratory failure
- Trauma
- Widely used for asthma, but this remains controversial1
Contraindications
- Absolute
- Immediate need for tracheal intubation
- Imminent cardiorespiratory arrest
- Anatomically fixed upper airway obstruction
- Facial burns
- Decreased level of consciousness in the setting of severe acute traumatic brain injury
- Relative
- Haemodynamic instability
- Impaired consciousness with inability to protect the airway
- Altered level of consciousness due to hypercapnia
- Recent upper airway surgery (requires discussion with surgeon)
- Copious secretions or vomiting
- Pneumothorax
- Facial injuries, including fractured base of skull
- Recent upper gastrointestinal surgery (requires discussion with surgeon)
- Following immediate transsphenoidal resection of a pituitary tumour (requires discussion with neurosurgeon)
Initial NIV Settings
Fraction of Inspired Oxygen ()
- Titrate to achieve target saturation of 88-92% in patients with chronic respiratory failure
- In other medical conditions (including neuromuscular disease and chest wall deformity), target range of 92-96%
- In acute coronary syndromes, target > 93%
- In heart failure, target > 90%
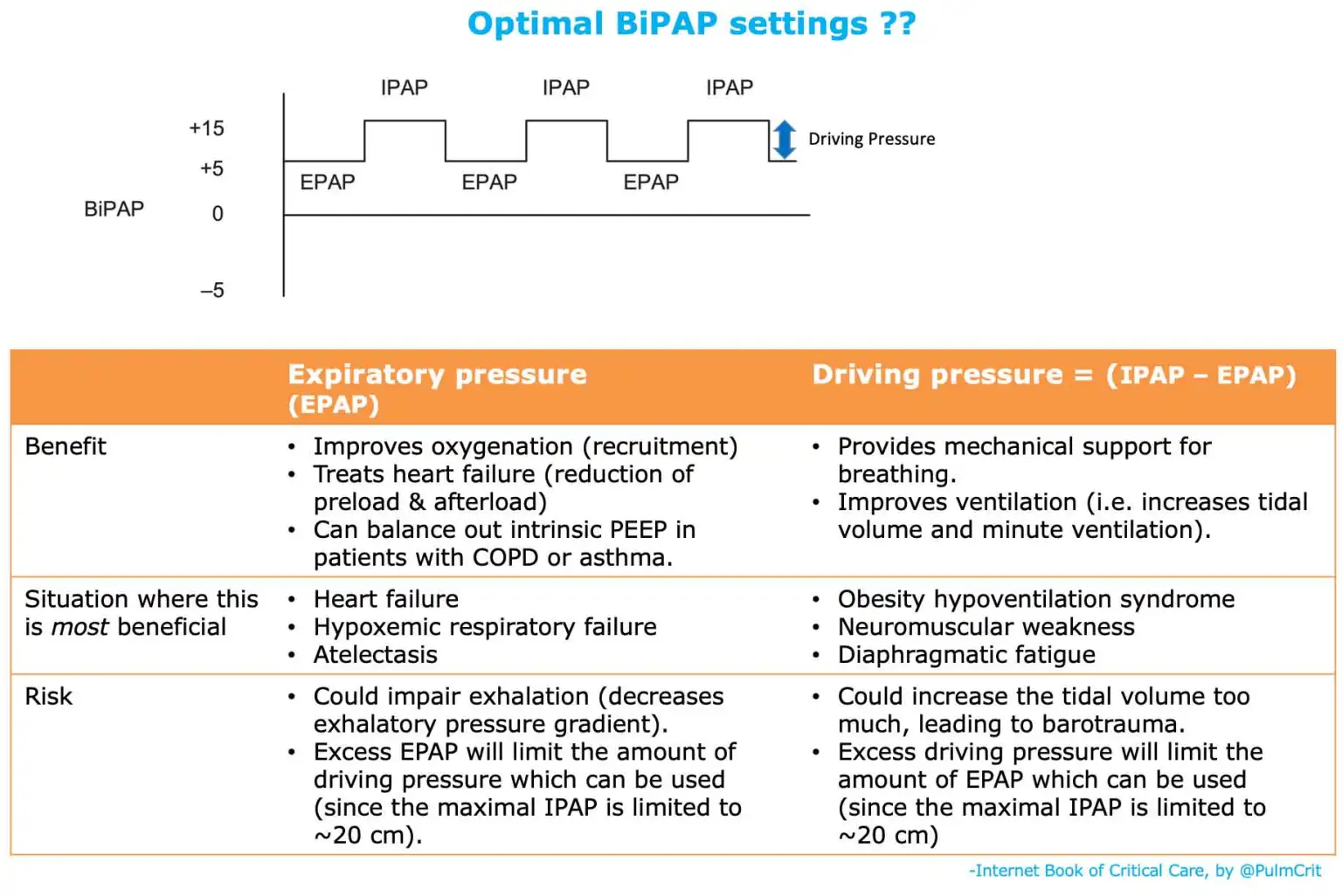
Settings for Congestive Heart Failure
- The goal is to have a relatively high EPAP setting to maintain high intrathoracic pressures throughout the respiratory cycle
- Example:
- Start at 10 cm IPAP / 5 cm EPAP to allow the patient to get used to the mask
- Increase to 15 cm IPAP / 10 cm EPAP
- Increase to 18 cm IPAP / 15 cm EPAP
- CPAP is also perfectly fine and is equally effective
Settings for COPD and Restrictive Diseases
- Initial settings
- S/T mode – spontaneously triggered with a timed backup respiratory rate
- IPAP 14 cm
- EPAP 4 cm
- Rise time 0.2 seconds
- Back-up respiratory rate (BRR) 12-16 breaths per minute
- Inspiratory time 1.0-1.4 seconds
- Increase IPAP by 2 cm increments every few minutes until maximum tolerance or target tidal volume of 8-10 mL/kg ideal body weight is achieved
- An IPAP of 20-25 cm may be required for adequate alveolar ventilation2
- Do not increase EPAP in the absence of obesity or obstructive sleep apnoea
- Adjust mask to minimise leaks
- Minimise to maintain 88-92%
Settings for Obesity Hypoventilation Syndrome
- The goal is to increase the driving pressure which provides mechanical support
- Initial settings
- S/T mode – spontaneously triggered with a timed backup respiratory rate
- IPAP 20 cm
- EPAP 8-10 cm
- Rise time 0.3 seconds
- BRR 12-16 breaths per minute
- Inspiratory time 1.4 seconds
- Increase IPAP by 2 cm increments every few minutes until maximum tolerance or target tidal volume of 8-10 mL/kg ideal body weight is achieved
- An IPAP of 20-30 cm is often required to effectively treat alveolar hypoventilation during sleep
- EPAP needs to be sufficient to overcome upper airway resistance and extrapulmonary restriction
- Adjust mask to minimise leaks
- Minimise to maintain 88-92%
Settings for Neuromuscular Disorders
- Initial settings
- S/T mode – spontaneously triggered with a timed backup respiratory rate
- IPAP 8 cm
- EPAP 4 cm
- Rise time 0.3 seconds
- BRR 12-16 breaths per minute
- Inspiratory time 1.4 seconds
- Increase IPAP in 1 cm increments, until maximum tolerance or target tidal volume of 6-8 mL/kg ideal body weight is achieved
- An IPAP of 12-16 cm is often sufficient
- A slightly higher EPAP may be required in bulbar disease or obesity (although generally minimal EPAP required)
- Adjust mask to minimise leaks
- Minimise to maintain 88-92%
Sedation
- Demedetomidine remains as one of the first line agents to allow tolerance of BiPAP however it has limited availability outside the ICU setting and can cause bradycardia and hypotension
- Alternatives include IV droperidol, haloperidol, ketamine, fentanyl
- Benzodiazepines are unfortuantely widley used but are probably not the best agents
Sources
- Non-Invasive Positive Pressure Ventilation (NIPPV) — ICU One Pager
- aci.health.nsw.gov.au/__data/assets/pdf_file/0004/820372/ACI-Non-invasive-ventilation-for-patients-with-acute-respiratory-failure.pdf
- Non-Invasive Ventilation (NIV) SID • LITFL • CCC Respiratory
- Noninvasive Respiratory Support - EMCrit Project
Footnotes
-
See Non-invasive ventilation (NIV) and asthma • LITFL for more information ↩
-
Noninvasive Respiratory Support - EMCrit Project suggests to avoid inspiratory pressures above 20 cm as it increases the risk of aspiration and gas inssuflation ↩