Immediate Assessment and Management in ED
| Mild-moderate | Severe | Life threatening | |
|---|---|---|---|
| Assessment | All of: Can walk, speak whole sentences in one breath (room air) > 94% | Any of: Unable to complete sentences in one breath Use of accessory muscles of neck or intercostal msucles/tracheal tug/subcostal recession during inspiration Obvious respiratory distress (room air) ≤94% | Any of: Reduced consciousness/collapse exhaustion/confused/agitated Cyanosis Poor respiratory effort (room air) <92% Poor respiratory effort, soft/absent breath sounds |
| Immediate treatment | Give salbutamol 4-12 puffs via pMDI and spacer | Start bronchodilators: Salbutamol 12 puffs via pMDI and spacer If can’t use spacer give 5mg nebule via nebuliser Ipratropium 8 puffs via pMDI and spacer every 20 minutes for first hour Start supplementation if <92% on room air and titrate to 92-96% | Arrange immediate transfer to higher-level care Start bronchodilators Salbutamol 2x5mg nebules via continuous nebulisation driven by oxygen Ipratropium 500mcg added to nebulised solution every 20 minutes for the first hour Maintain 92-96% |
| Continued treatment | Repeat salbutamol 4-12 puffs every 20 miutes for the first hour (or sooner if needed) Then reduce to every 4-6 hours if needed | Repeat salbutamol 12 puffs every 20 minutes for the first hour (or sooner if needed) Repeat bronchodilators every 4-6 hours for 24 hours If salbutamol delivered via nebuliser, add 500mcg ipratropium to nebulised solution every 20 minutes for first hour Repeat 4-6 hourly | Repeat bronchodilators 4-6 hourly When dyspnoea improves consider changing to salbutamol via pMDI plus spacer or intermittent nebuliser |
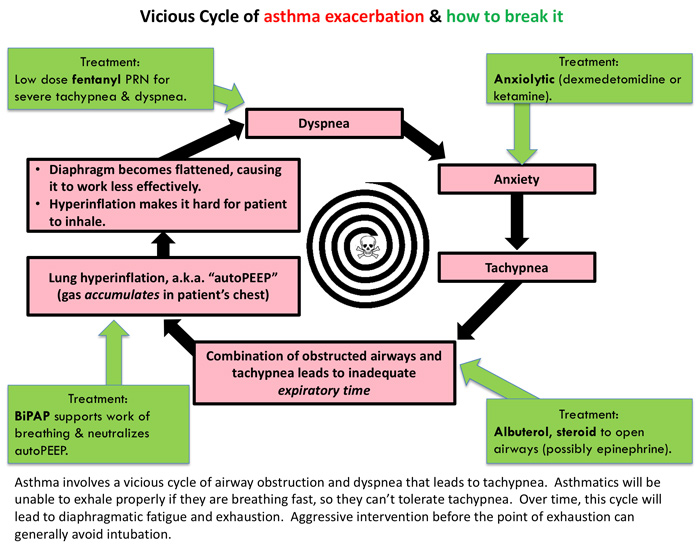
Severe asthma attack
Indicated by any of the following:
- RR ≥25 breaths/min
- Tacycardia ≥110 beats/min
- PEFR or FEV1 = 33-50% of predicted or known, despite nebuliser therapy Management includes steroid
Life-threatening attack with risk of Acute Respiratory Failure
Indicated by any of the following:
- Silent chest, cyanosis or feeble respiratory effort
- Bradycardia, arrhythmia or hypotension
- Altered mental status with exhaustion or confusion
- <92%; <60mmHg or normal or raised >34-45 mmHg on ABG If precipitate onset also consider Anaphylaxis; look for other features (e.g. urticaria, erythema, pruritis or angio-oedema)
- First line management
- Commence high-dose oxygen via a mask maintaining >95% and attach pulse oximetry monitoring
- Give salbutamol 5mg via an oxygen-driven nebuliser, diluted with 3mL normal saline
- Add ipratropium 500mcg to a second dose of salbutamol 5mg via the nebuliser if there is no response or there is a severe attack
- Give prednisolone 50mg PO or hydrocortisone 200mg IV if unable to swallow
- Avoid all sedatives, anxiolytics, NSAIDs and histamine-releasers (morphine)
- If patient’s condition does not improve
- Give repeated salbutamol 5mg nebulisers (up to 3 doses in first hour)
- Continue regular ipratropium 500mcg every 6 hours
- If patient’s condition is deteriorating or life-threatening features
- Obtain IV access, ensure steroids have been given, perform a CXR and call for senior help
- Give continuous salbutamol nebulisers
- Obtain ABG to check , pH and potassium which may be 2° low to beta-agonist therapy
- Treat if <3.0 mmol/L
- Start bronchodilator infusion IV with ECG monitoring and arrange ICU bed
- Give magnesium sulfate 2.5g IV (10 mmol) over 20-30 minutes
- Give salbutamol 250-500 mcg IV over 10 minutes
- Follow with infusion of salbutamol 5mg in 5% dextrose running at 60mL/h (10mcg/min) initially and titrate up to 120-240mL/h (20-40mcg/min)
Secondary Assessment
- Secondary assessment to be completed when feasible after starting salbutamol and oxygen
- Physical examination including vital signs
- Chest auscultation assessing for signs of complications (e.g. Pneumothorax, Pneumonia)
- Obtain an ABG if life-threatening acute asthma
- Obtain a chest radiograph to detect the presence of pneumothorax, consolidation or evidence of heart failure
- Obtain spirometry when patient able
- Brief history including:
- Reliever taken for this episode before presentation (dose, number of doses, time of last dose)
- Whether oral corticosteroid has been started (e.g. from asthma action plan)
- Current asthma medications
- Whether the patient has been prescribed a preventer (inhaled corticosteroid or combination of inhaled corticosteroid and long acting beta-2 agonist taken as maintenance or budesonide-formoterol as needed)
- Ask about adherence
- What triggered this episode if known (e.g. allergies, medicines, respiratory infections)
- Rarely triggered by food allergies but food allergy is a risk factor for life-threatening asthma
- Presence of co-existing heart or lung disease, including COPD
- Smoking/vaping status and exposure to environmental smoke/vaping
- Peak flow measurements at home
- Previous admission(s) to hospital (esp. in last 4 weeks)
- Socioeconomic challenges
- Homeless, unemployed, living alone
- Drug or alcohol use
- Psychiatric illness
Additional Therapy
- Start systemic corticosteroids within 1 hour of presentation if indicated; systemic corticosteroids are indicated for all severe and life-threatening acute asthma exacerbations and should be considered in other exacerbations on a case-by-case basis
- Adults: Oral prednisone/prednisolone 37.5–50 mg, then repeat each morning on second and subsequent days (total 5–10 days)
- Adolescents: Oral prednisone/prednisolone 1 mg/kg (maximum 50 mg) once daily for 3–5 days
- Assess clinical response after each dose of bronchodilator
- If dyspnoea/increased work of breathing is partially relieved within the first 5 minutes, reassess the need for repeated bronchodilator at 15 minutes.
- If dyspnoea/increased work of breathing is not relieved, or condition deteriorates, repeat bronchodilator dose and consider adding inhaled ipratropium bromide (if not part of initial treatment) or IV magnesium sulfate.
- Inhaled ipratropium bromide: Adults and adolescents: 8 actuations (21 microg/actuation) via pressurised metered-dose inhaler and spacer every 20 minutes for first hour. Repeat 4–6 hourly for 24 hours
- Intravenous magnesium sulfate: Adults and adolescents: 0.2 mmol/kg (maximum 10 mmol) diluted in a compatible solution as a single IV infusion over 20 minutes
- ABG is expected to be initially respiratory alkalosis but with tiring rises (respiratory acidosis) and metabolic lactic acidosis occurs
- Remember to monitor with ongoing salbutamol use
- Consider XR chest
- Other non-established treatments:
- Adrenaline – nebulised 5mg, SC 0.5mg, IV – load with 1mg → 1-20mcg/min
- Heliox – reduces turbulent air flow, 70:30 (He:O2)
- Ketamine – 0.5-2mg/kg/hr
- Inhalational agents – sevoflurane, anaesthetic machine or custom fitted ventilator required
- Leukotriene anatagonists – some benefit in chronic asthma
- BAL – can clear mucous plugging but transiently worsens bronchospasm
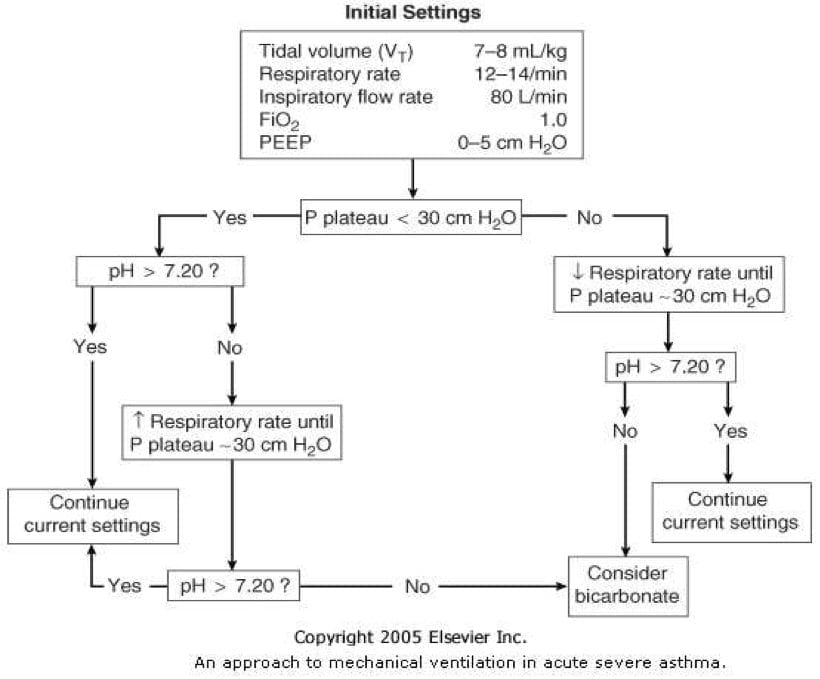
- Rapid sequence induction
- Induction agent: ketamine preferred because of bronchodilation, haemodynamic stability and preservation of respiratory drive
Differentials to Consider
- LVF
- Anaphylaxis
- Aspiration
- Upper airway obstruction (vocal cord dysfunction, tracheal stenosis)
- Inhaled foreign body
- PE
- Hyperventilation syndrome
- Pneumothorax
- Parodoxical motion of the vocal cords
Discharge criteria
- After respiratory distress or increased work of breathing has resolved and symptoms stabilised observe the patient for at least 4 hours
- Repeat spirometry and peak expiratory flow before discharge
- Ensure the patient has adequate maintenance doses of ICS and sufficient oral corticosteroid to complete the short course:
- ICS-formoterol (budesonide-formoterol or beclometasone-formoterol) to be taken as maintenance treatment and also as needed for relief of symptoms
- A combination of ICS and long-acting beta-2 agonist taken as maintenance treatment, with a short-acting beta-2 agonist (e.g. salbutamol) taken as needed for relief of symptoms
- Patient to see GP within 3 days with comprehensive assessment in 2-4 weeks to reassess risk factors and review treatment regimen
Useful Links
- Australian Asthma Handbook | Managing acute asthma in adults and adolescents
- Australian Asthma Handbook | Managing acute asthma in children 6–11 years
- Australian Asthma Handbook | Managing acute asthma in children 1–5 years
Sources
- On call handbook
- Asthma handbook (links above)
- Acute Severe Asthma SID • LITFL • CCC Respiratory
- Critical asthma exacerbation - EMCrit Project