Phone Call/Presentation Questions
- In what way is the patient acutely confused?
- Is there a depressed level of consciousness (see Unconsciousness)?
- Other vital signs?
- How old is this patient?
- Reason for admission?
- Previous episodes?
- Is there an obvious reason for the patient’s behaviour?
- Does this patient have dementia?
- Is the patient aggressive?
- Are they a danger to themselves/others?
- What measures have been tried to reason or calm the patient?
- Are staff or patients at risk of harm or actually injured?
- Who is there with the patient?
- What additional hospital personal are there to help now?
Instructions Over the Phone
- Check the patient’s airway, breathing and circulation and attach a pulse oximeter if the patient becomes unresponsive
- For combative or aggressive patients ensure safety of nursing staff and the patient by:
- Call security personnel if the patient is aggressive, confused or irrational
- Check a fingerprick glucose test
- Ask the nurse to give diazepam 5-10mg PO or olanzapine 5-10mg PO
- Request an IV trolley for the patient’s bedside and ask for 10mg midazolam or 10mg diazepam in 10mL syringe and 10mg haloperidol also in a 10mL syringe to be drawn up ready
Prioritisation
- Immediately see any patient with confusion associated with abnormal vital signs, a decreased level of consciousness, agitation or aggressive behaviour.
- Your role is not to rush to the ward to help restrain the patient, but to determine the cause of the patient’s behaviour and to organise appropriate support and medical treatment
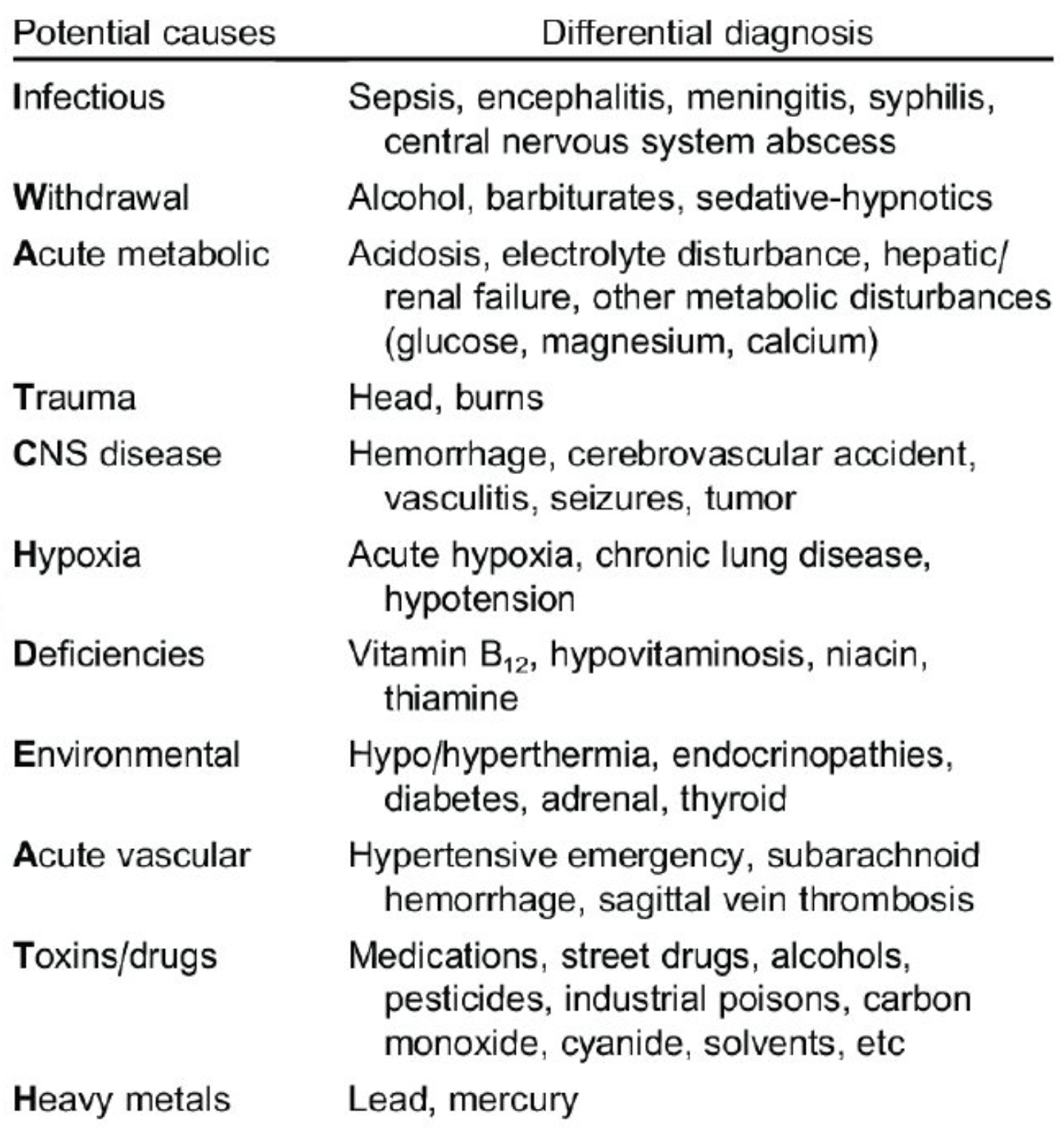
Common Causes (Corridor thoughts)
- CNS causes
- Infection: meningitis, encephalitis, abscess
- Stroke: CVA, SAH
- Tumour
- Head trauma: subdural or extradural haematoma
- Seizures: post-ictal, complex partial
- Cerebral vasculitis: SLE, polyarteritis nodosa
- Drugs (especially in the context of new meds, ↑ medication doses or AKI)
- Illicit drug substances
- Alcohol
- Narcotic and sedative drug excess or withdrawal
- Psychotropic medications (TCAs, lithium, phenothiazines, MAOIs, benzodiasepines, SSRIs) (e.g. serotonin syndrome & NMS)
- Miscellaneous (steroids, antihistamines, anticholinergics, levodopa)
- Metabolic
- Hyper/hypoglycaemia
- Hyper/hyponatraemia
- Hypercalcaemia
- Endocrine
- Hyper/hypothyroidism
- Cushing’s disease
- Addison’s disease
- Septicaemia
- UTI, biliary tract, meningococcaemia
- Environmental
- Hyper/hypothermia
- Psychiatric
- Mania, depression, schizophrenia
- Personality disorders or traits
- Delirium (mnemonic: I WATCH DEATH)
- Transient clouding of consciousness, inattention and failure of recent memory
- Acute fluctuating confusional state with restless (sometimes aggressive) behaviour and non-auditory hallucinations
- Dementia
- Chronic, progressive state of irreversible memory loss with global cognitive deficit
- Psychiatric disorder
- Can cause altered thinking with delusions but there is not disorientation or clouding of consciousness
Elderly Patients
Elderly patients with limited cerebral reserve become disorientated or delirious with relatively minor insults such as:
- Pain, cold
- Urinary retention, faecal impaction
- Decrease in vision or hearing (including missing aids)
- Unfamiliar surroundings (e.g. in hospital)
- Bereavement/separation
Assessment
End of Bed
- Be alert for agitation or aggressive behaviour
- Call for help early if concerned
- Is the patient responsive?
- Assess the airway for obstruction and ensure adequate respiratory effort
- Give oxygen and attach pulse oximeter to the patient and check blood glucose level
- Pallor or cold peripheries may indicate circulatory failure or blood loss
- Gain IV access, send bloods and start fluids
- Assess the pupils: constriction may indicate narcosis and dilation may indicate critical hypoxia
- Assess the airway for obstruction and ensure adequate respiratory effort
- What is the patient’s general appearance
- Look for external bruising and bleeding (coagulopathy)
- Subtle facial twitching may indicate ongoing seizure activity (non-convulsive state)
- Is the patient aggressive
- Decide from a safe distance how dangerous the patient is and what immediate measures are required to calm the situation
- Any signs of escalating aggressive behaviour → call for help
A → E Assessment
- Write Unable to review, patient not allowing for any part not able to be examined
- Can generally assess A and D
- Document the GCS
- Temperature?
- ↑ ⇒ infection, drug withdrawal or adverse drug reaction (including hyperpyrexia syndromes e.g. neuroleptic malignant or serotonin syndrome)
- ↓ ⇒ myxoedema, alcohol or sedative drug ingestion
- Respiratory rate?
- Confusion + tachypnoea ⇒ hypoxia or sepsis
- Bradypnoea + pinpoint pupils ⇒ narcotised by excessive opioid analgesia or a brainstem catastrophe
- Brainstem stroke = absent pupillary light reflex
- Narcotic poisoning = pupillary light reflex intact
- COPD + high flow oxygen → lose their hypoxic respiratory drive → hypercapnoea → confusion
- Heart rate?
- Tachycardia ⇒ hypoglycaemia, hypoxia, hypotension, sepsis, alcohol withdrawal and hyperthyroidism
- Bradycardia ⇒ ↑ ICP, myxoedema or preterminal hypoxia
- Blood pressure?
- Confusion + SBP <90mmHg ⇒ impaired cerebral perfusion in shock (see: Shock)
- Hypertension ⇒ intracranial haemorrhage, stimulant drug intoxication or alcohol withdrawal
- Blood glucose?
- Consider hypoglycaemia in diabetic patients (commonly due to excessive insulin, inadequate food intake or excessive exertion; may also occur with liver failure, alcohol excess or sulfonylurea overdose in the non-diabetic patient)
Immediate Management
- Unresponsive patient:
- Commence immediate management of DRSABCDE and call for help (see: ALS, Unconsciousness):
- Commence CPR if no signs of life
- Maintain spinal immbolisation if head trauma has occurred
- Commence high-dose oxygen via reservoir mask to maintain oxygen saturation >94%
- Attach cardiac monitoring and pulse oximeter to the patient
- Open the airway, insert an oropharyngeal device and assist ventilation with bag-valve-mask if required; call for senior anaesthstic assistance for endotracheal intubation
- Obtain IV access and take blood for FBC, UEC, LFTs, blood glucose and VBG
- Give 20mL/kg bolus of normal saline if BP <90mmHg
- Give 50mL of 50% glucose IV if fingerprick glucose <2.5mmol/L
- Give thiamine 250mg IV to prevent Wernicke’s encephalopathy if the patient is alcoholic or malnourished
- Give naloxone 200mcg boluses IV every 5 minutes if the patient has evidence of opioid toxicity (beware of precipitating a withdrawal state)
- Start immediate treatment for bacterial meningitis (e.g. ceftriaxone 2g IV) if the patient has meningism and fever
- Organise an urgent CT head scan if the patient has headache, possible head trauma, is on warfarin or a NOAC or has lateralising neurological signs
- Commence immediate management of DRSABCDE and call for help (see: ALS, Unconsciousness):
- Agitated and aggressive patient
- Reassure the patient and ensure physical safety of yourself and staff
- Some patients calm down simply because the doctor has arrived but still judge whether this is the case
- Verbal de-escalation
- Define acceptable and unacceptable behaviour and their likely consequences
- Speak firmly with courtesy and respect and address immediate concerns
- Explain what is happening at all times to the patient
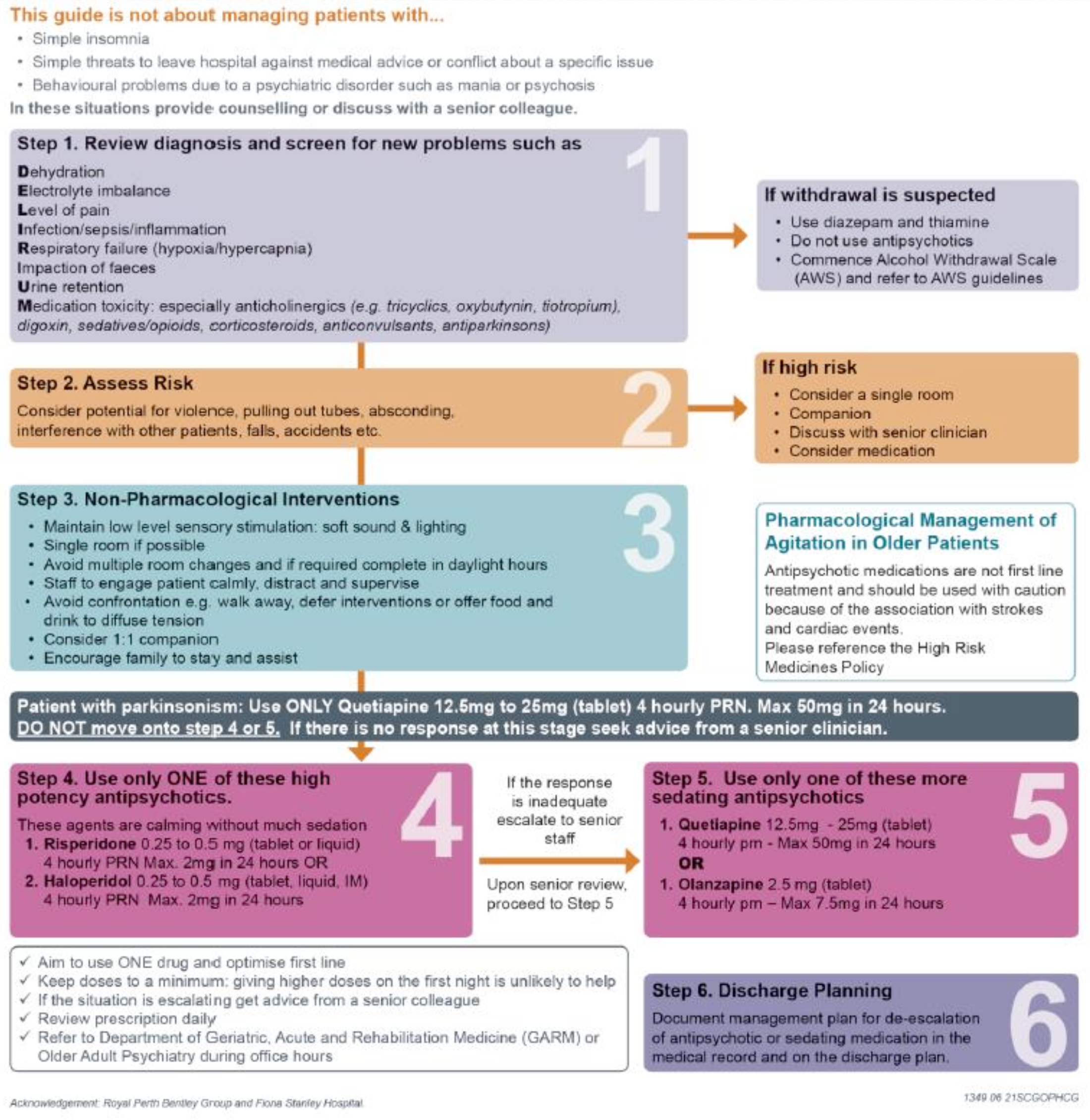
- Call the registrar, geriatrics or team on call before using physical or chemical restraints
- Physical restraint
- A show of force with ideally five security personnel aims to encourage the patient to accept reasoning
- Have at least one person per limb plus one controlling the head
- If the patient continues to threaten you or your staff, security personnel should restrain the patient after a clear verbal warning
- Rapid tranquilisation
- If the patient has already been given a benzodiazepines and is still out of control try to convince the patient to have further oral sedation (give another dose of midazolam 5mg PO or diazepam 5-10mg PO) or move to a different oral agent such as olanzapine wafer 10mg PO
- Using a temporary physical restraint, insert an IV cannula if still agitated1
- Give midazolam 2.5-5mg IV boluses, titrated to effect
- Add haloperidol 1-2mg IV boluses up to 10mg if the midazolam is wearing off too quickly
- Consider if the patient has a history of parkinsonism (parkinson’s disease, parkinson plus or lewy body)
- Once the patient is sedated, continuous bedside monitoring with pulse oximetry is essential, ideally with one-on-one nursing, until the patient wakes and is able to protect the airway
- Explain to any relatives what has happened. Reassure them that restraint is a temporary measure to protect the patient and others
- Reassure the patient and ensure physical safety of yourself and staff
Selective History and Chart Review
- The patient’s history is unreliable
- Are they orientated to person, place or time?
- Gain a collateral history from relatives or ward staff (esp. if precipitating event such as a seizure or fall out of bed)
- Review the patient’s chart and note the presenting problem and past medical history including:
- History of head trauma, recent febrile illness
- History of alcohol or drug misuse
- Ask when the patient’s last alcoholic drink was
- Withdrawal symptoms present within the first 72 hours of hospitalisation; unlikely after 1 week of abstinence
- Previous episodes of confusion? History of dementia
- Previous psychiatric history
- Recent surgery
- Consider residual effects of anaesthetic and analgesic medication, fluid and electrolyte disturbances, urinary infection (esp. with IDC), chest infection (including atelactasis within 24-48 hours) and/or PE
- Charts
- Observation chart
- Sudden change in vital signs may indicate drug toxicity or acute intracranial pathology
- Medication chart
- Look for newly prescribed medications and potential drug interactions
- Look at the list of medications normally taken at home; consider if an important medication has been omitted e.g. anti-hypertensive
- Look at hypoglycaemic medication
- Consider dose adjusting medications that might need renal or hepatic adjustment
- Observation chart
Examination
| Examination | Notes |
|---|---|
| Vitals | Repeat |
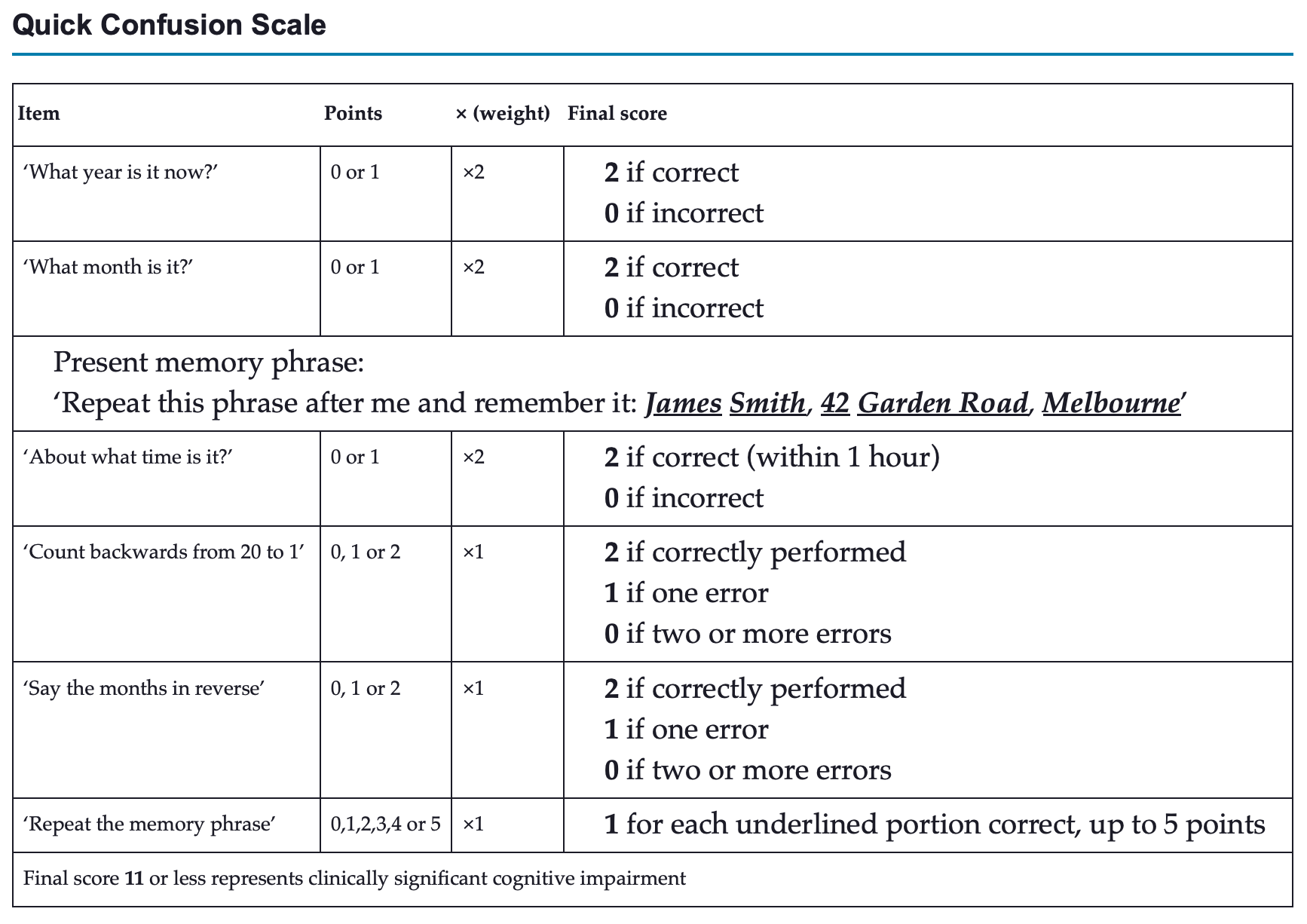
| Mental status | Record a formal GCS for level of consciousness |
| If GCS intact perform a quick confusion scale | |
| HEENT | Nuchal rigidity, neck stiffness, photophobia ⇒ meningitis, Subarachnoid Haemorrhage |
| Pinpoint pupils ⇒ opioids, clonidine, brainstem stroke or eye drops (e.g. pilocarpine for glaucoma) | |
| Dilated pupils ⇒ sympathomimetic or anticholinergic effect, hypoxia, ↑ ICP | |
| Haemotympanum or blood in ear canal ⇒ basal skull fracture | |
| Lacerated tongue or cheek ⇒ post-ictal state | |
| Fundoscopy | Papilloedema ⇒ hypercapnoea, ↑ ICP, Hypertensive encephalopathy |
| Dot and blot haemorrhages, exudates, neovascularisation ⇒ diabetic retinopathy | |
| Silver wiring, AV nipping, cottol-wool exudates and haemorrhage ⇒ hypertensive retinopathy | |
| Resp | Cyanosis ⇒ hypoxia |
| Barrel chest, wheeze, prolonged expiration and ↑ WOB ⇒ COPD with predominant hypoxia or with hypercapnoea | |
| Basal crackles ⇒ LVF, pneumonia | |
| CVS | ↑ JVP, S3 gallop, pitting oedema ⇒ CCF |
| Abdo | Costovertebral angle tenderness ⇒ pyelonephritis |
| Guarding, rebound tenderness ⇒ intra-abdominal haemorrhage or peritonism | |
| Jaundice, hepatomegaly, bruising, flap, encephalopathy ⇒ liver failure and/or ascites with splenomegaly ⇒ portal hypertension | |
| Neuro | Bilateral upgoing plantars ⇒ encephalopathies, ↑ ICP, postictal state, non-convulsive epilepticus, brainstem stroke |
| Asterixis or flap ⇒ liver failure, renal failure, hypercapnoea | |
| Tremor ⇒ DT, Parkinson’s disease hyperthyroidism |
Investigations
- Exclude hyper/hypoglycaemia and hypoxia:
- Check a BGL and pulse oximetry
- Send blood for FBC, UEC, LFTs
- FBC may reveal a leucocytosis indicating infection
- Macrocytosis suggesting alcohol use, folate or vitamin B12 deficiency
- Reticulocytes may suggest haemolysis
- UEC may identify renal failure or electrolyte abnormality
- LFTs may show hepatic dysfunction → if abnormal send a coagulation screen
- CXR
- Take two sets of paired blood cultures and send urine for MCS if sepsis is possible
- Other investigations depending on aetiology
- Thyroid function tests (myxoedema, thyrotoxicosis)
- Drug levels (digoxin, lithium, anticonvulsants)
- Antinuclear antibody, rheumatoid factor, ESR, complement C3 or C4 in autoimmune disease
- CT ead scan if suspect head trauma, meningism, focal neurological signs, ↑ ICP (papilloedema, hypertension and bradycardia); seizures
- Lumbar puncture after CT if suspect SAH or meningitis/encephalitis
- EEG if non-convulsive status epilepticus is considered
Specific Management
- Hypoxia: see Acute Respiratory Failure
- Hypotension: see Shock or Hypotension
- CNS disorders including seizures
- Drug intoxication or side effects:
- Stop the medication if the confusion is secondary to drugs
- Reverse opioid intoxication. with naloxone 0.1-0.2 mg IV, SC, IM every 5 minute repeated until alert
- Beware of precipitating an agitated withdrawal state in an opioid dependent patient or re-sedation as the naloxone wears off
- Drug withdrawal
- Alcohol withdrawal syndrome (see Alcohol Withdrawal)
- 12-48 hours of abstinence and may last up to 1 week; characterised by agitation, irritability, fine tremor, sweats and tachycardia
- Start the patient on an alcohol withdrawal chart
- Commence diazepam 5-20mg PO regularly until the patient is comfortable, plus thiamine 250mg IV daily. Give IV fluids and electrolyte replacement as required
- Delirium tremens
- DT is uncommon and usually occurs later at 72 hours after abstinence
- There is clouding of consciousness, terrifying visual hallucinations, gross tremor, autonomic hyperactivity with tachycardia and cardiac arrhythmias, dilated pupils, fever, sweating, dehydration and grand mal seizures that may be prolonged (status epilepticus)
- Give midazolam or diazepam 5-10mg IV as a bolus every 5-15 minutes until the patient is sedated (i.e. drowsy but rouses when stimulated)
- Refer to ICU
- Alcohol withdrawal syndrome (see Alcohol Withdrawal)
- Renal and hepatic failure - Ensure that end-stage kidney and liver failure have not been worsened by nephrotoxic or hepatotoxic medications - Aggressive treatment of the kidney failure (dialysis) or liver failure (lactulose, coagulopathy, raised ICP) may be needed; get senior help
- Depressed consciousness of unknown cause
- Some patients may have a depressed conscious level with no cause evident on history, physical examination or routine tests, including CT scan and lumbar puncture
- Intoxication or poisoning with:
- Anticonvulsant medication (may have ataxia or nystagmus)
- New-generation antipsychotics
- Partial-agonist opioids
- Long-acting benzodiazepines (e.g. clonazepam)
- Gamma-hydroxybutyrate (GHB)
- ‘Other’ alcohols, including methanol, ethylene glycol, isopropanol. Check for a metabolic acidosis with raised anion and osmolar gaps, and renal function
- Brainstem stroke
- May have pinpoint pupils, generalised hyperreflexia and bilateral upgoing plantars
- Non-convulsive status epilepticus or prolonged postictal phase
- Obtain urgent EEG if possible or give therapeutic trial of benzodiazepine to abort seizure activity
- Cerebral vasculitis
- CT or MR angiography will be needed, plus an immunology or rheumatology opinion
- Dementia
- Stable dementia may acutely decompensate to cause, or follow, hospital admission
- Manage as for acute delirium after looking for a precipitating cause:
- Quiet environment
- Set routines
- Calendars, clocks and staff continuity for environmental re-orientation
- Risperidone PO or SL to control agitation
Psychiatric Evaluation
- When normal level of consciousness, normal vital signs, normal investigation and no remaining confusion, but the patient has altered mental state perform a mental state examination and discuss with the acute psychiatry services:
- General appearance—grooming, posture, eye contact, motor activity, attitude
- Speech—rate, volume, spontaneity, articulation, pressure, neologisms
- Mood (the patient’s subjective experience of the emotional state)—elevated, happy, sad, angry, depressed
- Affect (the observer’s assessment of the patient’s emotional state)—dull, inappropriate, disinhibited
- Thought process—quality, relevance, blocking
- Thought content—suicidal, delusions, preoccupations, phobias, depersonalisation, ideas of reference, thought disorders
- Perceptual disorders—illusions, hallucinations
- Cognition
- Level of consciousness and orientation
- Memory—remote, recent, immediate (phrase or object recall)
- Concentration—serial 7s or equivalent
- Intelligence—vocabulary, general knowledge
- Judgement—ability to form rational opinions and choices
- Insight—awareness of situation.
Reference
Additional Flashcards
Avoid using benzodiazepines for delirium except when delirium is related to {{c1::alcohol or benzodiazepine withdrawal, or seizures::(2)}}
Benzodiazepines increase delirium risk and adverse effects are common
What is the pharmacological oral management for patients with delirium?
{{c1::Haloperidol 0.5 mg orally as a single dose}}
1 mg may be required for younger patients. Olanzapine and risperidone are also acceptable.
What is the pharmacological management for patients with delirium in which oral administration is not possible?
{{c1::Haloperidol 0.5 mg intramuscularly}}
1mg may be required for younger patients. Olanzapine also acceptable.
Footnotes
Footnotes
-
On call says to do this although I really thought you could give midazolam IM ↩