Indications for Chest Drain
- Primary spontaneous pneumothorax that was initially treated with catheter aspiration but did not respond
- Secondary spontaneous pneumothorax, unless the pneumothorax is small and the patient is clinically stable
- Traumatic pneumothorax, unless the patient is small and the patient is stable
- Decompensated (tension) pneumothorax, following urgent needle decompression
Definitions
- Primary spontaneous pneumothorax is pneumothorax occurring when there is no known underlying pathology, and no precipitant such as trauma or surgery
- Secondary spontaneous pneumothorax is pneumothorax occurring as a complication of underlying lung disease
- Traumatic pneumothorax occurs in the setting of trauma (iatrogenic or otherwise)
- Bronchopleural fistula connection between bronchial tree and pleura; usually refers to persistent air leak into the pleura
- Causes pneumothorax with ongoing re-accumulation if drained
Assessment
Differentials to consider in Traumatic Pneumothorax
- C-spine injury - always assumed in MVA trauma
- Head injury
- Haemothorax
- Blunt cardiac injury
- Cardiac tamponade
- Ruptured diaphragm
- Ruptured oesophagus
- Ruptured tracheobronchial tree
- Faciomaxillary injury
- Neck/larynx/chest trauma
- Foreign body obstruction
History
- Chest pain is sudden, described as stabbing, radiating to ipsilateral shoulder and pleuritic
- Nearly all patients have chest pain
- Sudden onset shortness of breath
- Commonly present
- Anxiety, cough and vague chest symptoms
Examination
- Involved hemithorax is hyperexpanded, hyperresonant and has ↓ breath sounds and air entry
- The affected side may have
- Decreased lung expansion
- Decreased or absent breath sounds
- Hyper-resonance on percussion
- Tracheal deviation is difficult to assess in real life. It’s dubious whether this adds anything of value to other clinical findings1
Presentation in Ventilated Patients
- Often do not complain of pain or dyspnoea due to sedation and analgesia
- Hypoxaemia with increasing FiO2 requirement
- Impaired chest wall compliance (greater pressures required for same volumes) indicated by:
- Volume cycled mode will lead to high peak and plateau airway pressures
- Pressure cycled mode will lead to low tidal volumes
- Ventilator mode also affects how rapidly the pneumothorax evolves
- Volume-cycled modes of ventilation continue to force same volume into pneumothorax which may cause aggressive increase in pneumothorax
- Pressure-cycled modes of ventilation provide smaller tidal volumes as the pneumothorax grows and since airway pressure is fixed, the pneumothorax may reach equilibrium with the ventilator causing the pneumothorax to present in a more gradual fashion
Other Considerations
- Differential diagnosis of spontaneous pneumothorax in women of childbearing age
- Primary spontaneous pneumothorax.
- LAM (Lymphangioleiomyomatosis).
- Pneumocystis.
- Catamenial pneumothorax (accounts for ~25%)
Investigations
Imaging
- Bedside ultrasound2
- Demonstrates the absence of lung sliding (barcode sign); note that presence of lung sliding excludes pneumothorax at that point on the thorax and absence may also be seen in:
- Adhesions between the lung and the chest wall (e.g. pleurodesis, infection or fibrosis)
- Right mainstem intubation
- Mucous plugging and/or severe atelectasis
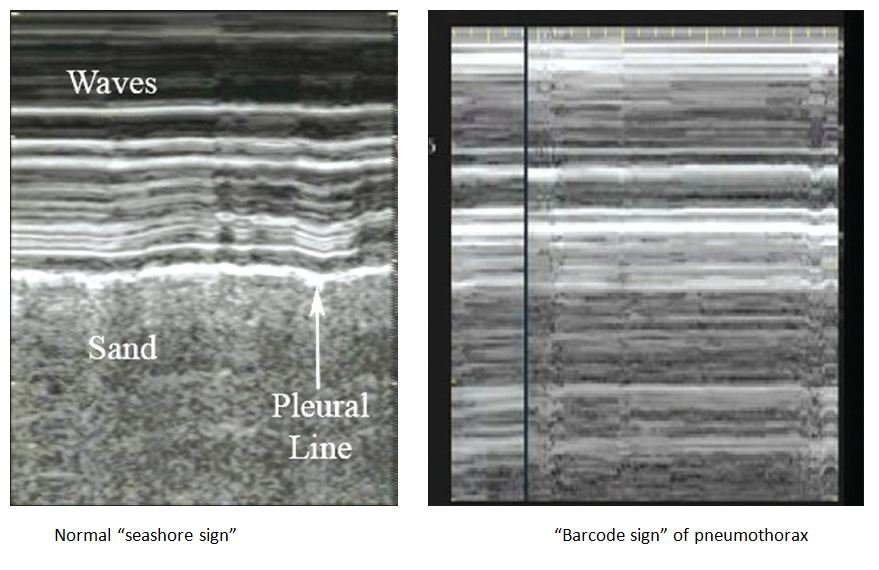
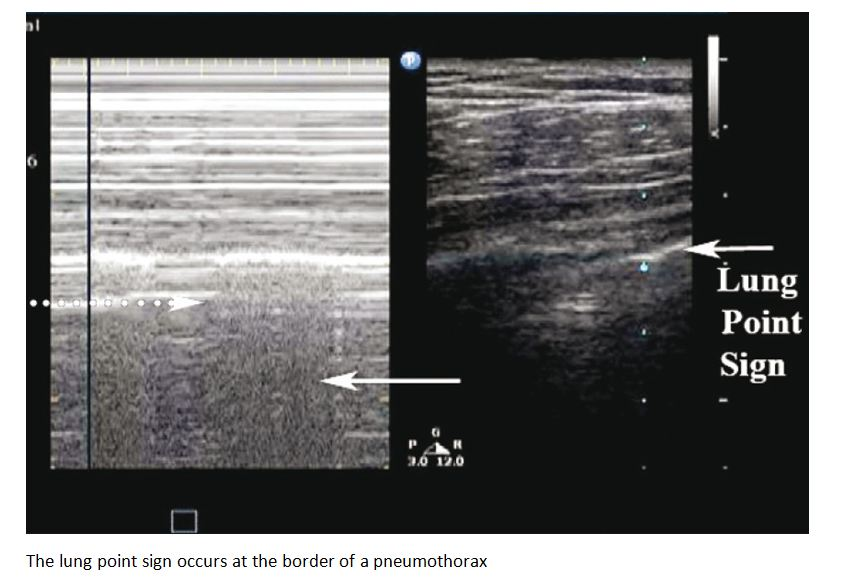
- Lung point which refers to a dynamic transition point between pneumothorax (A-line pattern) and sliding lung
- Strong evidence for a pneumothorax
- Demonstrates the absence of lung sliding (barcode sign); note that presence of lung sliding excludes pneumothorax at that point on the thorax and absence may also be seen in:
- Inspiratory erect CXR (standard CXR)3 but can request expiratory CXR if in doubt; findings include:
- Subcutaneous emphysema
- Visceral pleural line which should have the following features
- Line should be continuous and traceable for a long distance
- Line should be thin and often subtle
- Lung markings should be absent beyond the pleural line
- Do not mistake it for a skin fold
- Deep sulcus sign
- Assess size:
- Small = visible air rim <2cm
- Large = visible air rim ≥2cm around all the lung edge
- CT scanning is recommend for uncertain or complex cases
Management
Decompensated (Tension) Pneumothorax
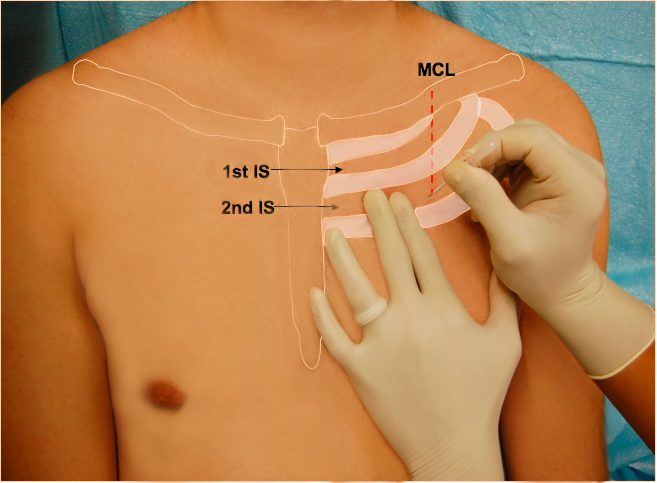
- Treat immediately with needle decompression of haemithorax:
- Prepare the skin with antiseptic and infiltrate local anaesthetic to the skin adjacent to periosteum and pleura (if time allows)
- Insert a 14G IV cannula over the 3rd rib into the 2nd intercostal space in the midclavicular line on the affected side but noting that:
- In larger patients, it may be difficult to penetrate into the pleura
- The clavicle extends to the shoulder, so midclavicular should be towards the lateral edge of the theorax; if the needle is inserted too medially it may lacerate the internal mammary artery
- Issues with emergent needle decompression:
- If there isn’t a large pneumothorax, the needle will lacerate the lung tissue
- If there is a sizable bronchopleural fistula (e.g. mechanically ventilated patients), a small bore needle may nto be sufficient to drain air from the pneumothorax
- Drainage of the pneumothorax may actually make it harder and more dangerous to insert a chest tube
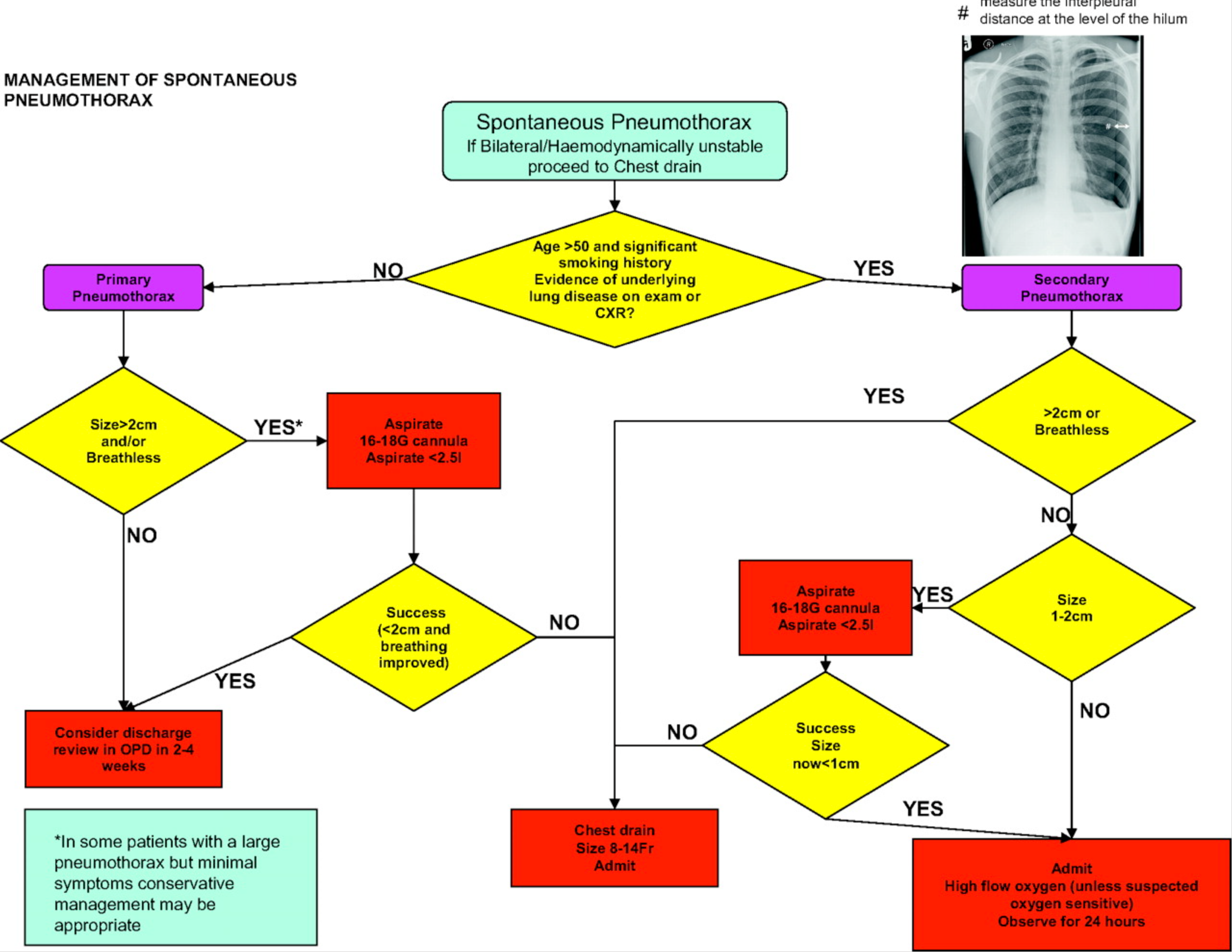
Spontaneous Pneumothorax
- Determine degree of breathlessness
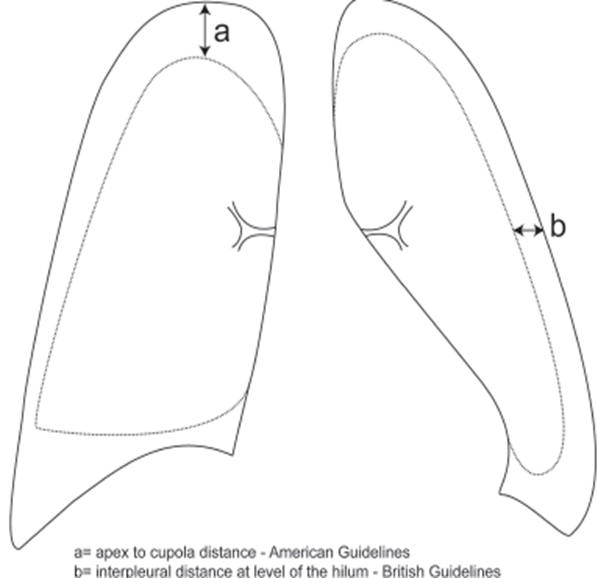
- Determine size of pneumothorax
- British thoracic guidelines: large = >2cm between lung margin and chest wall at level of hilum
- Americal college of chest physicians = >3cm between lung apex and cupola
Disposition and Follow Up
- Patients should receive verbal and written advice to return immediately to ED if they develop further breathlessness
- All patients should have follow up ideally by a respiratory physician to ensure resolution of pneumothorax and institute optimal care
- Recurrence of pneumothorax may warrant a referral for pleurodesis
- Those managed by Observation or needle aspiration should return for a follow up CXR after 2-4 weeks to monitor resolution
- Normal physical activities can be resumed once all symptoms have resolved but avoid extreme exertion until full resolution
- Patients should be advised to stop smoking as it is an associated factor in recurrence
- Air travel should be avoided until at least 1 week after the CXR shows full resolution
- SCUBA diving should be discouraged permanently
Sources
- Agency for Clinical Innovation
- https://aci.health.nsw.gov.au/networks/eci/clinical/tools/respiratory/spontaneous-pneumothorax
- https://aci.health.nsw.gov.au/networks/eci/clinical/tools/respiratory/spontaneous-pneumothorax/spontaneous-pneumothorax-management-options
- https://aci.health.nsw.gov.au/networks/eci/clinical/tools/respiratory/spontaneous-pneumothorax/spontaneous-pneumothorax-treatment-options
- Derranged physiology
- eTG Pleural Disease | Pneumothorax
- IBCC: https://emcrit.org/ibcc/pneumothorax/
Footnotes
-
Unfortunately, commonly taught in ALS workshops to use RATES when assessing breathing and hence look for tracheal deviation (often late sign). Personally, I think more attention should be placed to auscultation skills ↩
-
More sensitive than CXR ↩
-
Some sources say can request an expiratory CXR if in doubt, but eTG says it is not recommended because it may exaggerate the size of the pneumothorax ↩