- More common in women than men
Clinical Presentation
- Sudden onset of rapid, regular palpitations
- Associated symptoms:
- Presyncope or syncope due to a transient fall in blood pressure
- Chest pain (esp. if underlying coronary artery disease)
- Dyspnoea
- Anxiety
- Polyuria from elevated atrial pressure causing release of atrial natriuretic peptide
Pathophysiology
The following is the pathophysiology for the ‘slow-fast’ varient of AVNRT
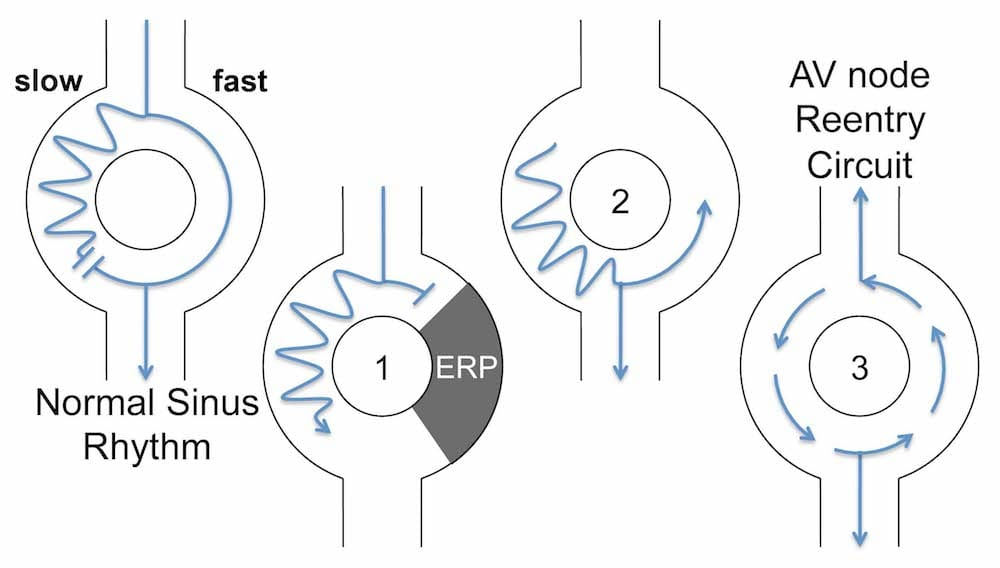
- Requires two specific pathways within the AV node:
- Slow conducting pathway (alpha) with a short refractory period
- Fast conducting pathway (beta) with a long refractory period
- PAC arrives while fast pathway is refractory and goes down the slow pathway
- When the effective refractory period in the alpha pathway ends, the impulse travels retrogradely up the fast pathway
- Impulse continually cycles around the two pathways
ECG Features
- Regular tachycardia ~140-280 bpm
- Narrow QRS complexes (<120ms) unless there is a co-existing bundle branch block, accessory pathway, or rate related aberrant conduction
- P waves if visible exhibit retrograde conduction with P-wave inversion in leads II, III, aVF; they may be buried within or visible after the QRS complex (very rarely before) causing a pseudo R’ or S wave
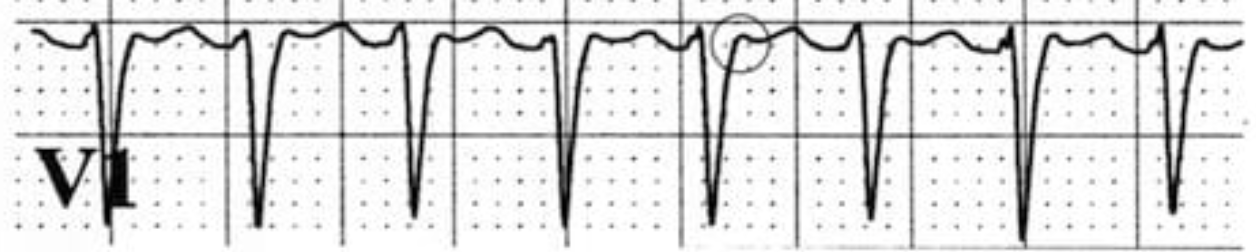
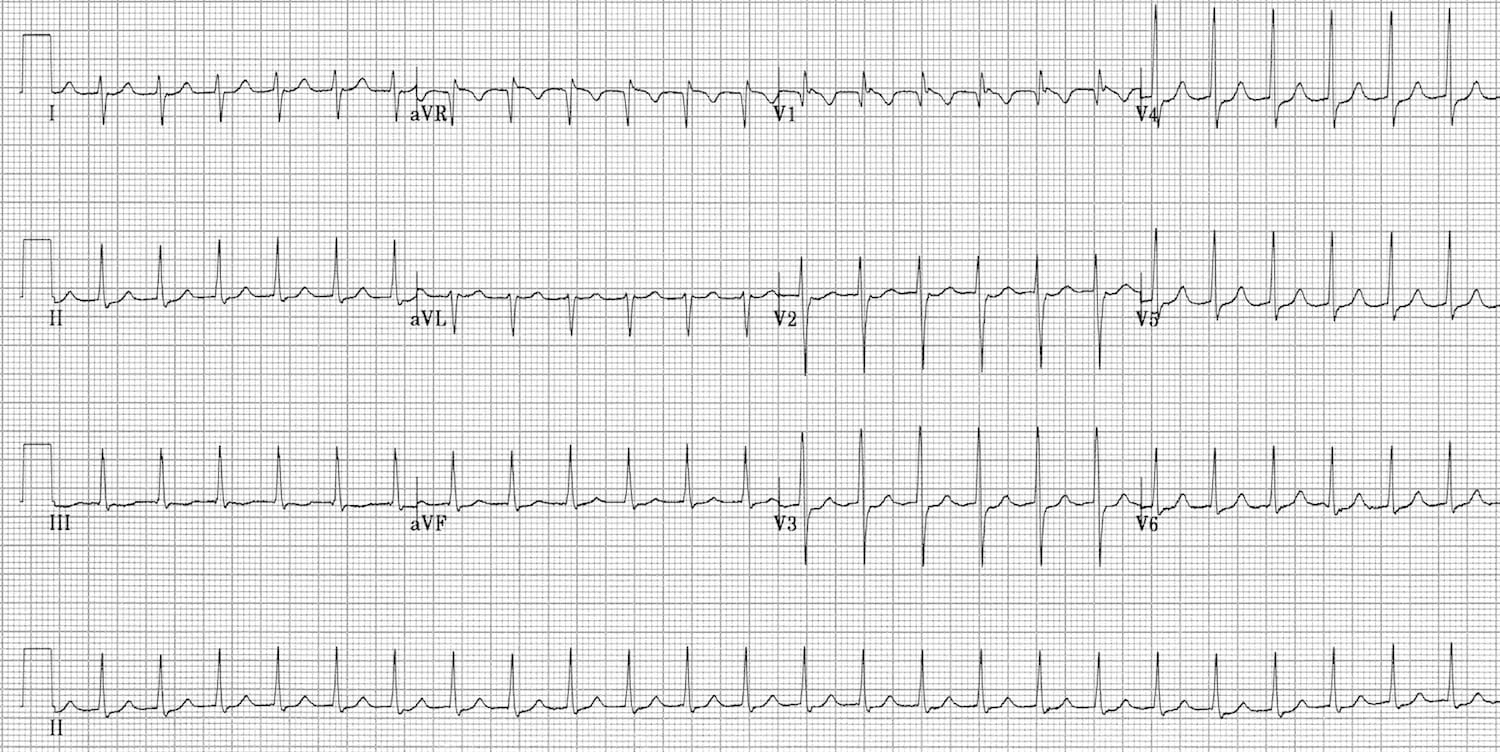
- Narrow complex tachycardia at 150 bpm with no visible P waves
- Pseudo R’ waves in V1-2
ST Depression in AVNRT
Widespread ST depression is a common ECG finding in AVNRT and does not necessarily indicate myocardial ischaemia, provided the changes resolve once the rhythm is sinus
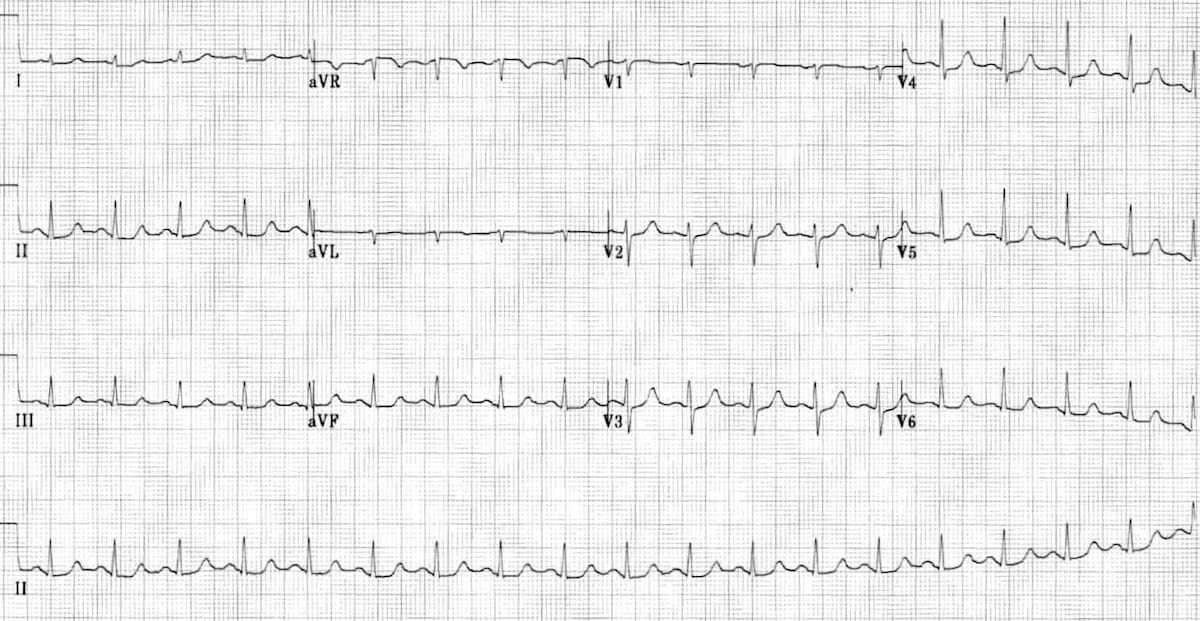
After resolution of the AVNRT:
- Here there is residual ST depression in inferior and lateral leads (V4-6) ⇒ patient had rate-related myocardial ischaemia
Differentiating orthodromic AVRT and AVNRT
Link to original
- Typically AVNRT has retrograde P waves that occur early (typically buried in the QRS or pseudo R’ waves at the terminal portion of the QRS)
- In AVRT, retrograde P waves occur later, with a longer RP interval (typically >70 ms)
- Management however is the same between the two conditions and may reveal the underlying accessory pathway in AVRT once reverted
Management
- See SVT Management