- Also see Adrenal Crisis
Definitions
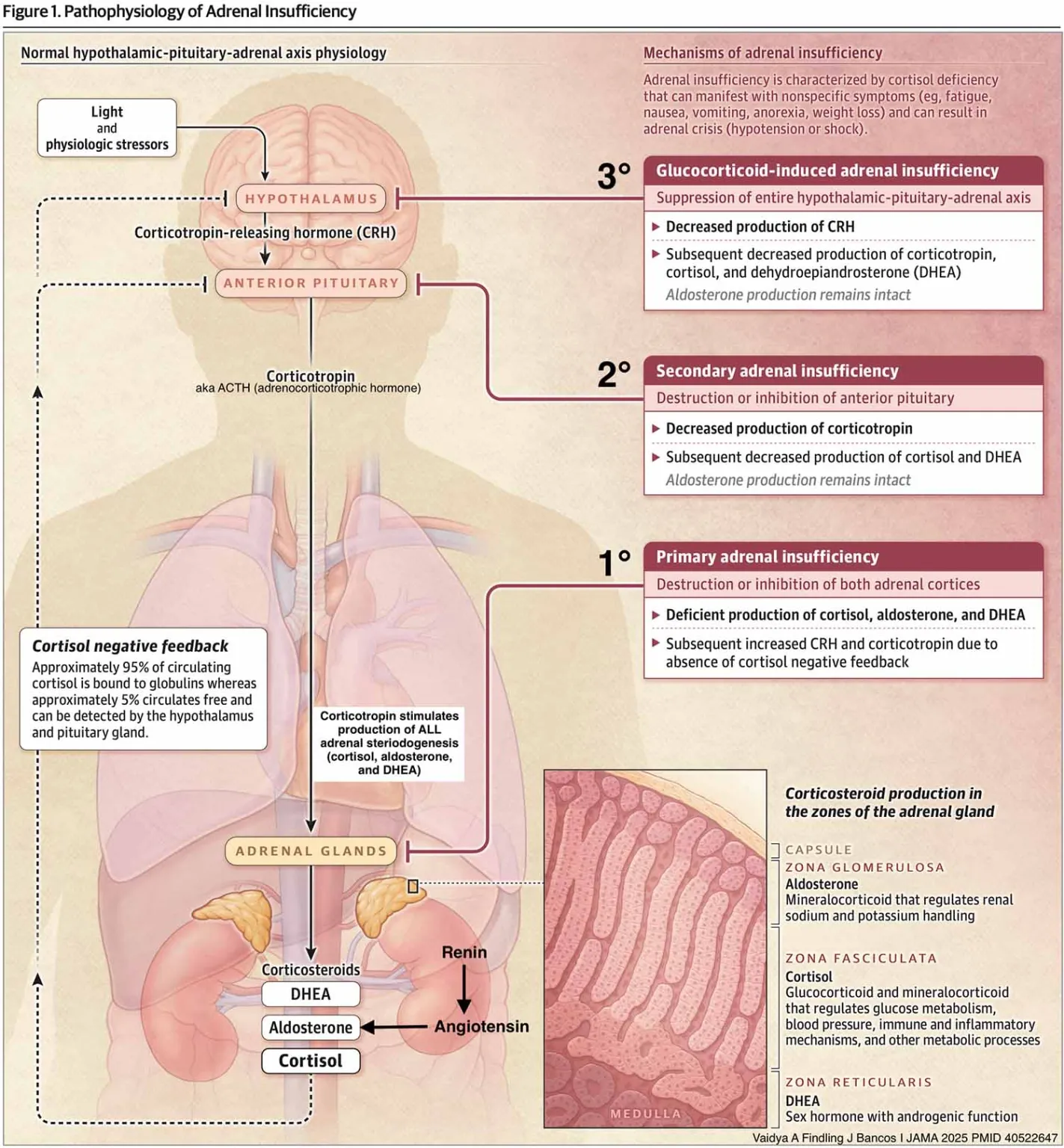
- Adrenal gland hormones:
- Adrenal cortex
- Glucocorticoids (eg cortisol)
- Mineralocorticoids (eg aldosterone)
- Androgens (eg dehydroepiandrosterone DHEA)
- Adrenal medulla
- Catecholamines (eg adrenaline)
- Adrenal cortex
- Adrenal insufficiency = insufficient production of glucocorticoids and mineralocorticoids by the adrenal cortex
- Androgen production may also be decreased
- Primary adrenal insufficiency = Addison disease; usually caused by autoimmune-related atrophy of the adrenal cortex although other causes include infection and metastatic cancer
- Secondary adrenal insufficiency = Pituitary or hypothalamic disorder causes ↓ adrenocorticotropic hormone (ACTH)
- Tertiary adrenal insufficiency = exogenous steroid use → ↓ CRH and ↓ ACTH → atrophy of hypothalamus/pituitary/adrenal axis so it is unable to respond to acute stress
Clinical Features
- Fatigue
- Anorexia
- Weight loss
- Postural hypotension
- Skin and mucosal hyperpigmentation1
Diagnosis
- Combination of:
- Positive short Synacthen test (i.e. an absent or severely blunted plasma cortisol response to tetracosactide 30 to 60 minutes after injection)
- Elevated ACTH
- Elevated plasma renin (measured by direct concentration or plasma renin activity)
Management
- Primary adrenal insufficiency
- Replacement of glucocorticoid and mineralocorticoid
- Androgen replacement not often required
- Secondary adrenal insufficiency
- Glucocorticoid replacement only as renal-angiotensin-aldosterone axis intact
- A patient with adrenal insufficiency should:
- Increase glucocorticoid dose during intercurrent illness
- Recognise early features of adrenal crisis (eg nausea, vomiting, dehydration, hypotension)
- Carry injectable hydrocortisone when away from medical care
- Wear an alert bracelet or necklace
- Carry a wallet card with details about their condition and treatment
- Ongoing monitoring assess for symptoms of:
- Glucocorticoid excess: weight gain, facial puffiness, peripheral oedema, insomnia, low bone mineral density (measure every 2 years), elevated blood pressure, hyperglycaemia
- Glucocorticoid deficiency: weight loss, lack of appetite, progressive skin pigmentation, lethargy
- Mineralocorticoid excess: elevated blood pressure, peripheral oedema, hypokalaemia, low plasma renin concentration
- Mineralocorticoid deficiency: postural hypotension, tachycardia, hyperkalaemia
- Patient with autoimmune adrenal insufficiency have increased risk of other autoimmune disorders (e.g. coeliac disease, autoimmune thyroid disease, type 1 diabetes, pernicious anaemia); monitor accordingly
Glucocorticoid Dosing During Illness
- The dose of glucocorticoid must be increased at the onset of a systemic illness or before a surgical procedure
- The patient should increase their glucocorticoid dose promptly without regard for time of day or waiting for a doctor
- Higher dose should be continued for 2-3 days and if the illness has not resolved after 3 days, then the patient should seek medical advice
- Suggested doses for increasing glucocorticoid dose are on eTG and are based on adult/child and choice of glucocorticoid for maintenance therapy
- If the patient has features of impending adrenal crisis (e.g. abdominal pain, dehydration, hypotension) give hydrocortisone 100mg intramuscularly (for adults)
Glucocorticoid Dosing During Surgery
- Minor procedure that does not require general anaesthetic, sedation or fasting ⇒ double dose of patient’s usual glucocorticoid on the morning of the procedure
- For root canals double the dose of usual glucocorticoid for a further 24 hours postoperatively
- For invasive dental procedures not requiring general anaesthetic use a double dose of usual glucocorticoid on the morning of the procedure and for a further 24-48 hours post-operatively
- For patients with postoperative complications or inability to take oral intake or vomiting, follow as per illness above and administer parenteral hydrocortisone
- For procedures requiring general anaesthetic, sedation or fasting ⇒ start IV hydrocortisone at induction of anaesthesia and continue until oral intake can be tolerated following the procedure
- Hydrocortisone 100mg IV initially then 50 mg IV 6 hourly until oral therapy is tolerated
Mineralocorticoid Replacement
- Symptoms of aldosterone deficiency:
- Postural vertigo/syncope
- Salt craving
- Fatigue and weakness
- Sometimes polyuria/noctuiria
- Hyperkalaemia
- Replace with fludrocortisone: fludrocortisone 100 micrograms orally, daily. Adjust dose according to postural blood pressure, and serum potassium and plasma renin concentrations. Usual dose 50 to 300 micrograms daily
- Monitor: BP, serum sodium and potassium concentrations, plasma renin concentration
- If a patient has hypertension and a plasma renin concentration at the lower end of normal, reduce the fludrocortisone dose
- If a patient has hypertension and a plasma renin concentration at the higher end of normal or elevated and the patient does not have any other signs that suggest mineralocorticoid excess (e.g. oedema, hypokalaemia), start antihypertensive therapy (usually ACE-i, ARB or CCB)
- In concurrent Acute Heart Failure, most heart failure therapy can be used except the aldosterone antagonist (spironolactone); instead fludrocortisone dose should be reduced or stopped
Sources
- eTG: Adrenal Insufficiency. Accessed 25/12/2025
- Adrenal gland & steroid pharmacology - EMCrit Project
Footnotes
-
Hyperpigmentation may be absent if adrenal insufficiency develops rapidly ↩