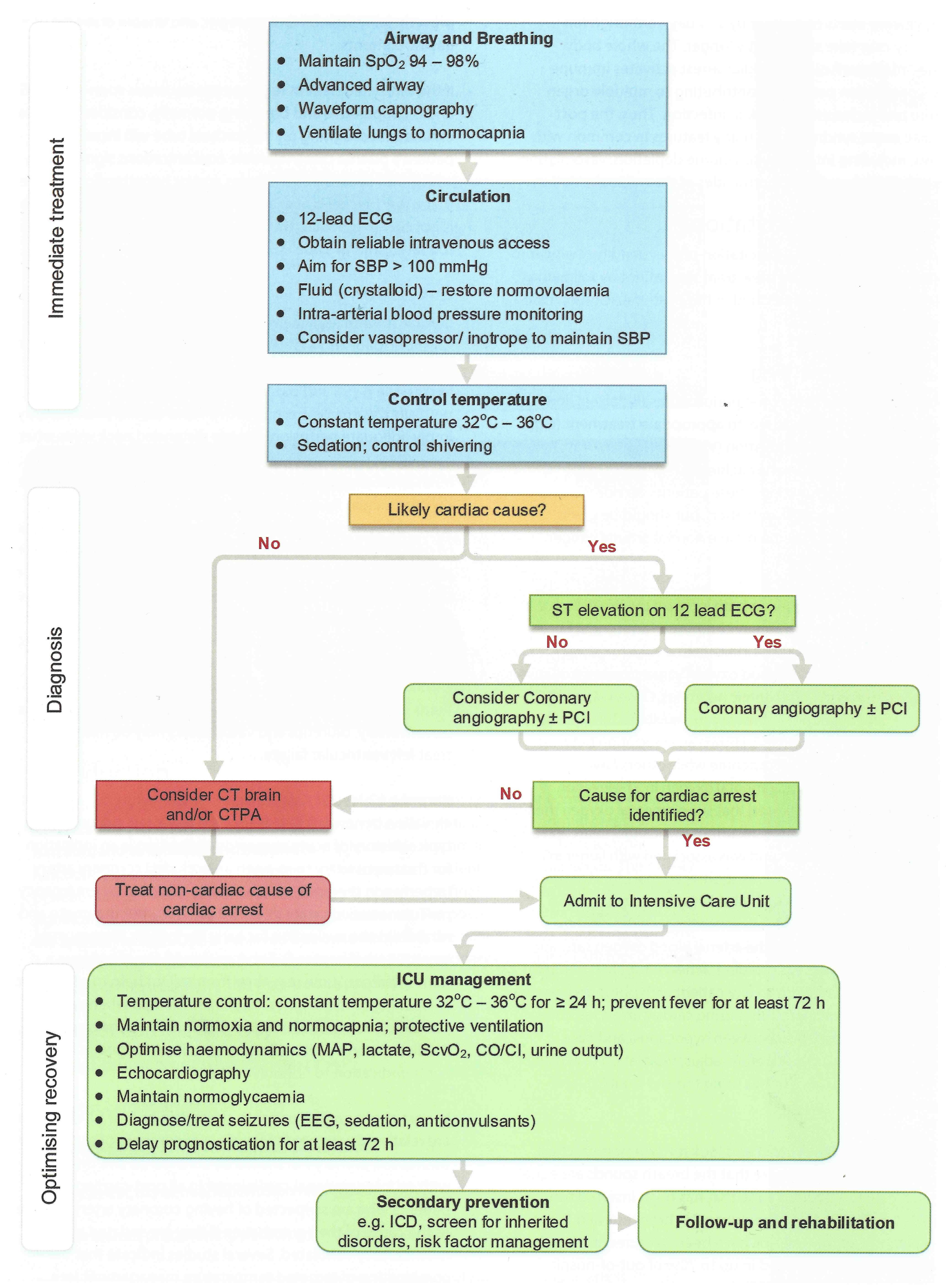
Immediate Priorities at ROSC
- Secure and confirm airway (intubate if comatose; waveform capnography)
- Obtain IV/IO access, continuous ECG, SpO₂, invasive arterial BP
- 12-lead ECG immediately post-ROSC
- Identify and treat reversible causes (4Hs & 4Ts)
- Transfer to ICU
Pathophysiology
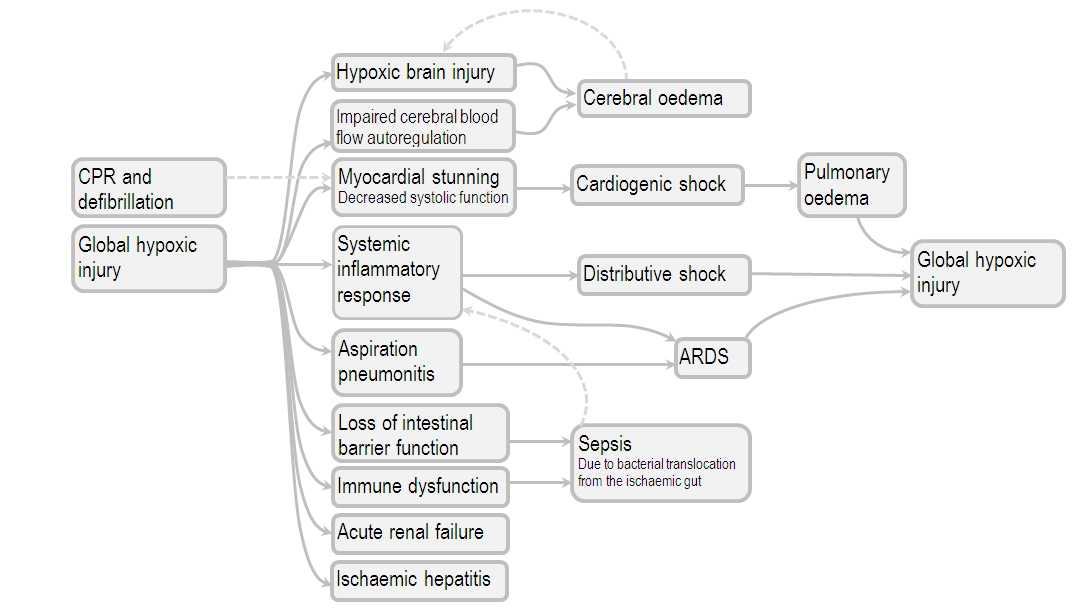
- Endothelial response to prolonged hypoxia is pro-inflammatory mimicking Septic Shock; the hypotension is similarly responsive to noradrenaline
- There is post-cardiac arrest myocardial stunning for 48-72 hours during which period the heart is responsive to inotropes
- Adrenal dysfunction may exist despite elevated cortisol levels (i.e. relative adrenal insufficiency); can consider administration of corticosteroids in patients unresponsive to vasopressors
- Hypoxic brain injury
- After restoration of circulation, the cerebral bloodflow autoregulation mechanism is impaired resulting in cerebral vasodilation and hyperaemia
- Excess oxygen can genereate free radicals and neuronal lipid peroxidation
- Renal failure
- Ulceration of the gastric mucosa from hypoxia and other CPR related stomach injuries
- ARDS
- Which can occur in a plethora of ways probably in tandem:
- Failing left ventricle
- Aspirated stomach contents
- Pulmonary contusion from CPR Endothelial dysfunction
- Lowering body temperature to result in lower means lower minute volume requirements which means lower tidal volumes (protective lung ventilation)
- Which can occur in a plethora of ways probably in tandem:
- Ischaemic Hepatitis
Aetiologies
- Cardiac arrest is the common pathway of any severe illness and therefore the differentials remain quite broad, nontheless here is a list of common causes:
- Arrhythmia
- VT/VF related to structural heart disease (remote MI, acute MI, HOCM, ARVC, myocarditis, cardiac sarcoidosis, amyloidosis)
- VT/VF with a structurally normal heart (Torsades de pointes, WPW plus AF, Brudgada syndrome, Commotio cordis)
- Bradycardia (e.g. heart block)
- Primary respiratory arrest - note that agonal respirations are nonspecific and do not necessarily indicate a primary respiratory aetiology
- Upper airway obstruction
- Severe asthma or COPD
- Tension pneumothorax
- Primary neurologic arrest
- Intracranial haemorrhage
- Seizures (SUDEP = sudden unexpected death in epilepsy), status epilepticus
- Toxicologic/metabolic
- Overdose (e.g. opioids)
- Hypoglycaemia
- Hyperkalaemia, hypokalaemia, hypomagnesaemia
- Any cause of profound shock
- Arrhythmia
Assessment
- ECG immediately post ROSC with particular attention to:
- Ischaemia
- Brugada pattern
- ARVC
- QT interval (long QT syndrome)
- Early repolarisation
- Wolff-Parkinson-White pattern
- Hypertrophic Cardiomyopathy
- Evidence of PE
- Labs
- Glucose
- Basic labs (CMP, EUC, FBC, Coags, LFTs)
- ABG/VBG
- Troponin
- Troponins at 12 hours post arrest (with a cut-off of 0.6 ng/ml, or 600 ng/L) had 96% sensitivity and 80% specificity for myocardial infarction which is probably not very useful
- Mainly for monitoring for reinfarction
- CRP
- Blood cultures if concern for sepsis
- B-HCG if required
- Urine toxicology
- X-ray chest
- POCUS:
- Lung POCUS
- Echocardiogram
- Abdominal USS evaluating for peritoneal blood or ascites
- CT head to pelvis
- Purpose:
- Find cause of cardiac arrest
- Evaluate for complications of CPR (e.g. liver laceration)
- CT head may provide information about neuroprognostication
- Evaluate for evidence of aspiration/pneumonia
- Protocol
- Head CT: non-contrast is often adequate unless concern for a primary CNS pathology in which case consider CT angiography
- Chest CT: Obtain CT angiography to exclude PE if this is a possibility
- CT abdomen/pelvis with contrast is usually adequate
- Timing
- After initial resuscitation and stabilisation
- Purpose:
- EEG
Management
Targets
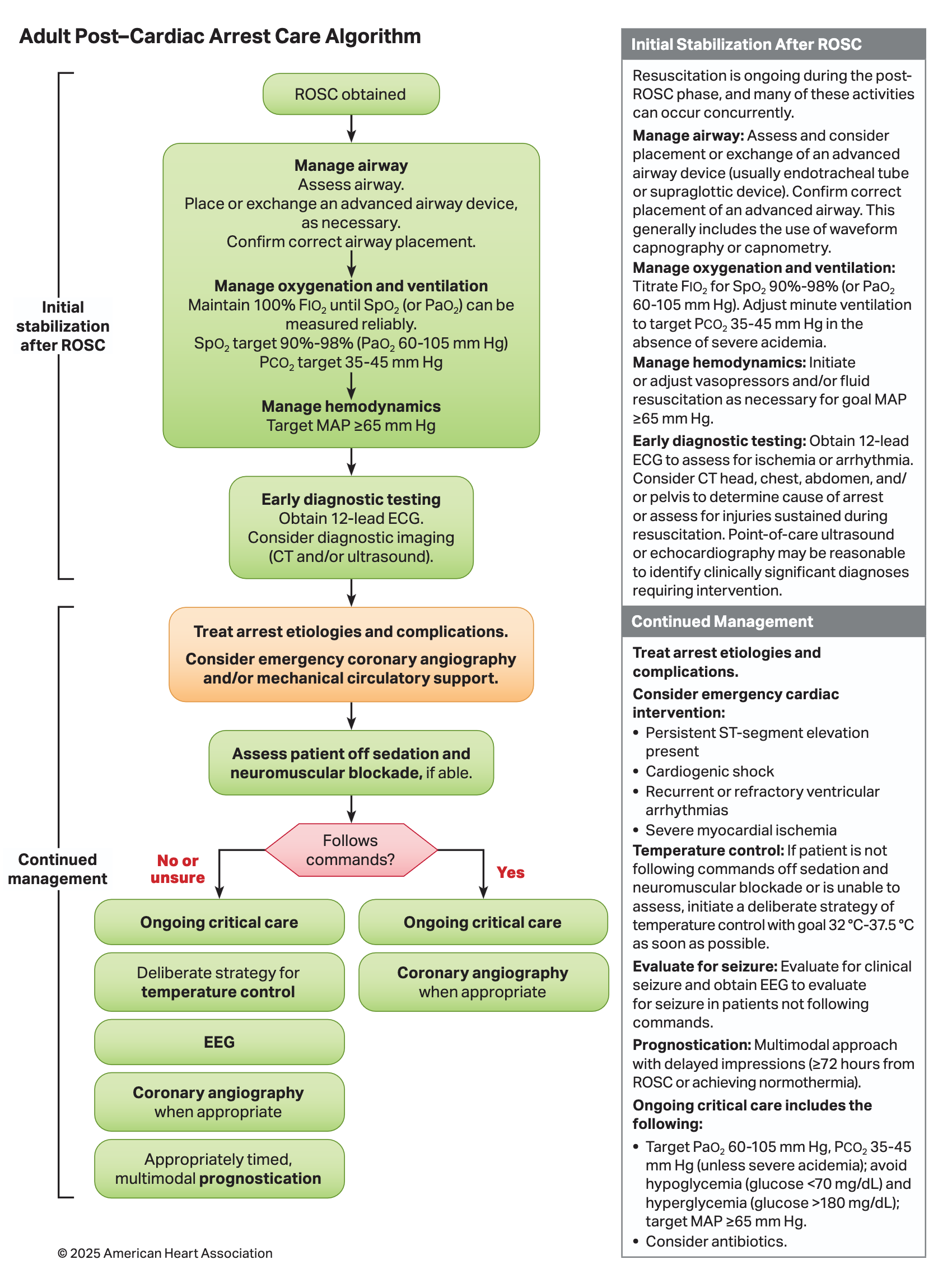
| Domain | Target / Recommendation | Guideline Source |
|---|---|---|
| O₂ (initial) | 100% FiO₂ until SpO₂ measurable | AHA 2025, RCUK 2025 |
| O₂ (maintenance) | SpO₂ 94–98% / PaO₂ 60–105 mmHg | AHA 2025, RCUK 2025 |
| Ventilation | PaCO₂ 35–45 mmHg | AHA 2025, RCUK 2025 |
| MAP | ≥65 mmHg | AHA 2025, RCUK 2025 |
| Temperature (comatose) | ≤37.5°C (fever prevention); hypothermia 32–34°C uncertain benefit | ANZCOR 2024, RCUK 2025 |
| Fever avoidance duration | ≥72 hours post-ROSC | ANZCOR 2024, RCUK 2025 |
| Glucose | 4–10 mmol/L (avoid hypo and hyperglycaemia) | AHA 2025, RCUK 2025 |
| ECG post-ROSC | Immediate 12-lead | AHA 2025 |
| Coronary angiography | Immediate if STEMI; delayed if no ST↑ (OHCA) | RCUK 2025, BMJ BP |
| Neuroprognostication timing | ≥72 hrs post-ROSC or post-rewarming | AHA 2025, ERC/ESICM 2021 |
| Seizures (treatment) | Levetiracetam or valproate; no prophylaxis | RCUK 2025 |
| Antibiotics | Not routine; low threshold if pneumonia suspected | AHA 2025, RCUK 2025 |
- Normoxia:
- Aim for a of around 100 mmHg
- Aim for normocapnoea
- In the first 24 hours aim for a termpature of 32-36 degrees (targeted temperature management) except in:
- Those with obvious good neurology
- Those with uncontrollable bleeding (colder temperatures cause less platelet aggregation)
- Aim for a MAP ≥ 65 mmHg and a SBP > 100 mmHg
- Aim for a BSL between 8-10
- NG feeding can commence during TTM
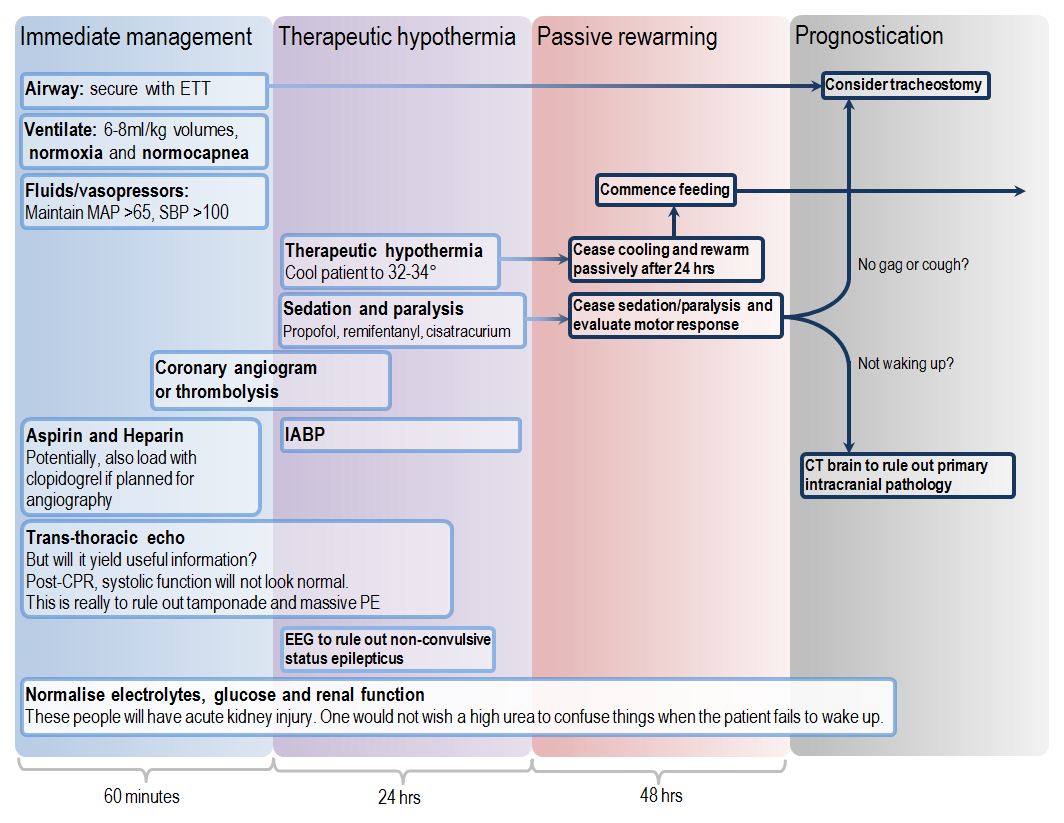
- Sedation
- Avoid benzodiazepines as their clearance is decreased with hypothermia
- Propofol and ramifentanil may be the most suitable combination
Ventilator Management
- Comatose patients post-ROSC should be intubated with waveform capnography confirmation
- Use 100% initially and once reliable /ABG available titrate for normoxia ( 94-98%, 75-100 mmHg)
- Aim for normocapnoea 35-45 mmHg with lung protective tidal volumes and avoid hypocapnoea (causes cerebral vasoconstriction)
- Strategy
- Immediately after intubation, adjust the minute ventilation to achieve an end-tidal of 30-25 mmHg
- Since > end-tidal , this will generally put in the safe range
- Then obtain an ABG/VBG to verify that is within the target range
- Immediately after intubation, adjust the minute ventilation to achieve an end-tidal of 30-25 mmHg
- Exceptions
- Patients with chronic hypercapnoea may benefit from being maintained at their chronic baseline
- Patients with severe metabolic acidosis may benefit from a degree of respiratory comepensation if necessary to maintain a safe pH
- Strategy
- Nursing position 30° head up
- If significant aspiration can consider early antibiotics
- Do not routinely give bicarbonate for all cardiac arrest as it may cause increased intracellular acidosis as the bicarbonate is converted to with the release of ions
- Give bicarbonate in cardiac arrest associated with hyperkalaemia or tricyclic overdose
Haemodynamic Management
- Target MAP ≥ 65 mmHg
- MAP goals can later be adjusted and individualised for example:
- A higher MAP goal in a patient with oliguria and chronic hypertension
- A lower MAP goal in a patient with cardiogenic shock
- Additionally ARC guidelines recommends a MAP required to achieve a urine output > 1 mL/kg/hr and normal or decreasing plasma lactate
- MAP goals can later be adjusted and individualised for example:
- Initiate vasopressors and fluid resuscitation as needed
- Noradrenaline and fluid with/without dobutamine is usually most effective
- ARC ALS 2 guidelines suggest insertion of an IABP where the above is inadequate
- Obtain continues ECG monitoring, invasive arterial BP and central venous access in comatose patients
- Avoid steroids routinely for post-arrest shock
Coronary Investigation
- ACS accounts for ~65% of out of hospital cardiac arrests with a shockable rhythm
- Indications for emergent angiogram
- OMI on ECG
- Cardiogenic shock attributable to coronary artery disease
- Recurrent ventricular arrhythmias
- Evidence of significant ongoing myocardial ischaemia
- Indications for delayed angiogram prior to discharge
- Those with suspected cardiac aetiology especially in the presence of
- An initial shockable rhythm
- Unexplained left ventricular systolic dysfunction
- Evidence of severe myocardial ischaemia
- Those with suspected cardiac aetiology especially in the presence of
- Medical therapies may be indicated for patients with probably/definite type 1 MI
Temperature Control
- Actively prevent fever by targeting temperature ≤37.5°C for comatose patients post-ROSC
- Avoid fever ≥ 37.7°C for at least 72 hours post-ROSC in comatose patients
- Duration of termpature control should be at least 24 hours from achieving target and fever prevention should continue for 36-72 hours
Antiarrhythmic Therapy
- For most patients observation without antiarrhythmic therapy is recommended however consider in:
- Recurrent arrhythmias
- VT/VF arrest pending catheterisation
- Persistent hypertension (e.g. propranolol)
- Electrolyte repletion
- Aggressive magnesium repletion may be useful for shivering prevention and for some arrhythmias
- Potassium repletion
- Refer all patients who had cardiac arrest in a shockable rhythm outside the context of STEMI or non-cardiac arrhythmogenic causes for ICD insertion prior to discharge
Seizure Management
- Use EEG to diagnose seizures
- First line anti-epileptic medications are levetiracetam and sodium valproate but routine seizure prophylaxis is not recommended
Targeted Temperature Management
- Patients who are able to follow commands only require supportive care, for those unable to follow commands the following applies
- Temperature control is recommended for:
- OOHCA with initially shockable rhythm who remain unresponsive after ROSC
- Temperature control is suggested for:
- OOHCA with initial non-shockable rhythm who remain unresponsive after ROSC
- IHCA with any intiial rhythm who remain unresponsive after ROSC
- Temperature control
- Target a temperature of 37.5°C in most patients especially if those who shiver when targeting lower temperatures (e.g. 36°C)
- Methods
- Simple ice packs and/or wet towels
- Cooling blankets or pads
- Transnasal evaporative cooling
- Intravascular heat exchanger placed in the femoral or subclavian veins
- Infusion of cold saline or Hartmann’s solution
- Paracetamol 1000 mg q6hrly as an antipyretic, analgesic and anti-shivering agent
- If temperature control is used it should continue for at least 24 hours
- Rewarming should occur at 0.25-0.5°C/hour
Neuromanagement
- Sedation:
- Typically propofol is the agent of choice initially; other alternatives include dexmedetomidine
- Ketamine infusion (0.1-0.3 mg/hr) is often helpful for both analgesia and shivering
- Avoid benzodiazepines or opioids as they may delay awakening and confound neuroprognostication
- EEG monitoring
Gastrointestinal Management
- Nutrition should be managed as usual
- Patients are at high risk of stress ulcerations so prophylaxis is recommended
Neuroprognostication
- Should not occur earlier than 72 hours post-ROSC or ≥72 hours from rewarming in cooled patients
- Examination
- Pupillary and corneal reflexes
- Between 0-24 hours:
- A lack of pupillary response is nonspecific.
- The presence of pupillary responses may be an encouraging sign (especially if they occur rapidly after cardiac arrest).
- If both pupillary and corneal reflexes are present soon after ROSC, this suggests a favorable outcome.
- After 72 hours:
- The absence of any pupillary response is ~20% sensitive and ~99% specific for poor neurological outcome1
- The absence of any corneal reflex is ~30% sensitive and ~97-100% specific for poor neurologic outcome.
- After 96 hours:
- The lack of any pupillary response bilaterally approaches 100% specificity for poor neurological outcome.
- The absence of corneal reflexes may approach 100% specificity for a poor neurologic outcome.
- Between 0-24 hours:
- Pupillary and corneal reflexes
- Somatosensory evoked potentials
- In short, the idea is that Per nerve stimulation should evoke a response in the cortical central neurons
- EEG at 24 hours after arrest
- Hold any sedative infusions
- Administer paralytics if necessary
Sources
- Deranged Physiology
- IBCC
- Resuscitation Council (UK):
- American Heart Association
- Australia Resuscitation Guidelines: Advanced Life Support Level 2. Third Australian Edition. Gale M. et. al. March 2016
Footnotes
-
i.e. If the pupillary reflex is absent, then there’s a 99% change the patient will have a poor neurological outcome. If the pupillary reflex is present, then it does not say much (only 20% of patients with poor outcomes show absent pupils at 72 hours) ↩