Definitions
- KDIGO AKI workgroup defined AKI as any of the following:
- ↑ Cr by 26.5 µmol/L
- ↑ Cr to ≥ 1.5 x baseline
- Urine output < 0.5 mL/kg/h for 6 hours
- KDIGO AKI Stages
- Stage I AKI
- Cr 1.5-1.9 times baseline over 7 days
- Cr increase >26.4 µmol/L over 48 hours
- Urine output <0.5 ml/kg/hr for 6-12 hours
- Stage II AKI
- Cr 2-2.9 times baseline
- Urine output <0.5 ml/kg/hr for 12-24 hours
- Stage III AKI
- Cr >3 times baseline
- Cr >354 µmol/L
- Initiation of renal replacement therapy
- Urine output <0.3 ml/kg/hr for >24 hours
- Anuria >12 hours
- Stage I AKI
- Other classifications exist (see Deranged Physiology: A comparison of classification systems for acute kidney injury)
Risk Factors
- Age >65
- Infection on admission
- Heart failure
- Cirrhosis
- Respiratory failure
- Haematological malignancy
- Post cardiac arrest
- Pre-existing renal failure
Prevention
- Maintain a Hb > 70
- Ensure intravascular volume is adequate
- Avoid chloride-rich fluids
- Avoid using hydroxyethyl starch
- Achieve satisfactory haemodynamic parameters (e.g. MAP > 70 mmHg)
- In chronically hypertensive septic patients, aim for a higher MAP (eg. 75-80mmg)
Aetiologies
- Medications:
- Cardiovascular
- Direct:
- ACEi & ARBs
- Indirect:
- For patients with borderline cardiac output, medications that reduce cardiac output may be nephrotoxic (e.g., beta-blockers, diltiazem).
- For patients with borderline hypotension, antihypertensives may be nephrotoxic.
- Direct:
- Antibiotics
- Aminoglycosides
- Trimethoprim-Sulfamethoxazole (and other sulfonamides).
- Vancomycin
- Beta-lactams rarely cause interstitial nephritis (especially penicillins such as nafcillin, piperacillin, and ampicillin).
- Antifungals
- Amphotericin*
- Antivirals (not exhaustive)
- Acyclovir, ganciclovir, valacyclovir, valganciclovir (crystal deposition).
- Indinavir.
- Tenofovir
- Chemotherapy
- Miscellaneous
- Antiepileptics (topiramate, zonisamide).
- Bisphosphonates (pamidronate, zoledronic acid).
- Immunosuppressives:
- Calcineurin inhibitors (cyclosporine, tacrolimus).
- mTOR inhibitors (sirolimus, everolimus).
- Inflammatory bowel disease medications (mesalamine, sulfasalazine).
- Intravenous immunoglobulin (IVIG).
- Mannitol
- NSAIDs
- Cardiovascular
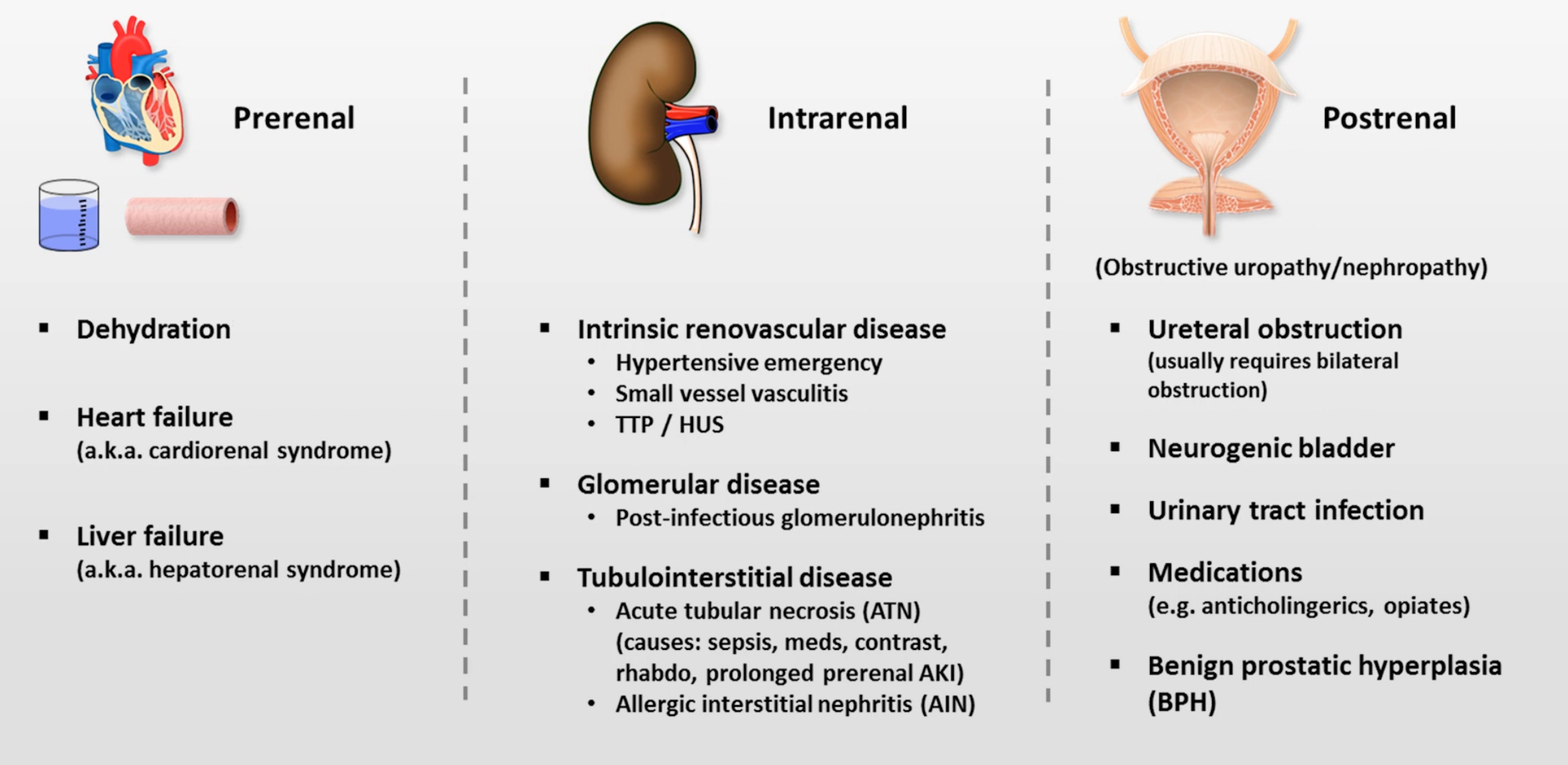
Distinguishing Pre/Intra/Post Renal Failure
| Intra-renal | Pre-renal | |
|---|---|---|
| Urine osmolality | <400-450 mOsm/kg | >450-500 mOsm/kg |
| Urine sodium | High (>40 meq/L) | Low (<20 meq/L) |
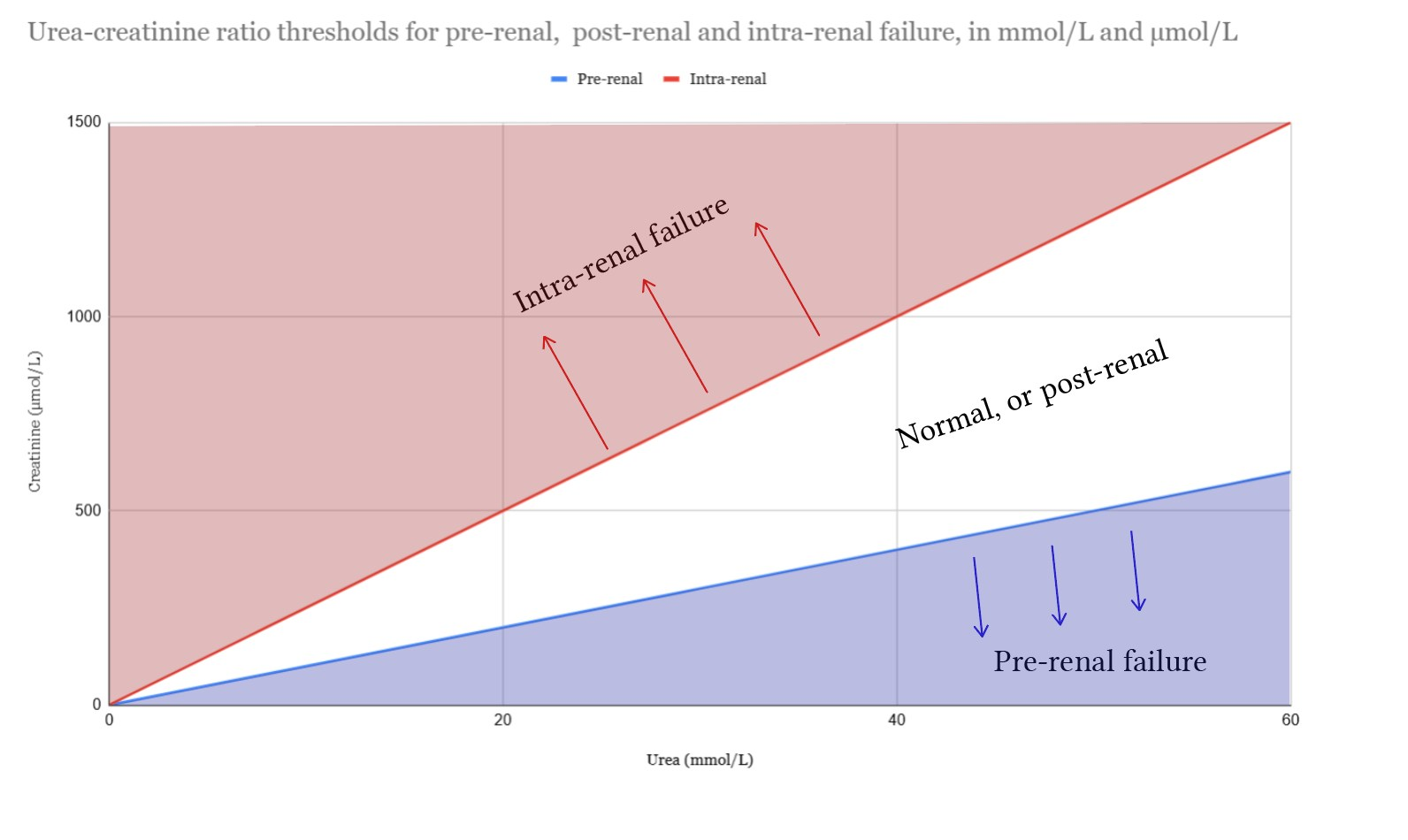
| Urea:Cr (mmol:µmol) | <0.04 | >0.1 |
| Urine/serum creatinine ratio | >40 | <20 |
| Urine/serum osmolality | >1.0 | >1.5 |
| Fractional excretion of urea | >25% | <25% |
| Fractional excretion of sodium1 | >2% | <1% |
| Urine microscopy | Muddy brown granular casts, epithelial casts, epithelial cells | Nothing, hyaline casts |
Diagnostic Approach
- Labs
- EUCs
- CK
- Urinalysis and sediment analysis
- Additional labs to consider
- Relevant drug levels (e.g. vancomycin, aminoglycoside, cyclosporine, tacrolimus levels)
- Uric acid level
- Plasma-free haemoglobin
- Urine albumin/creatinine ratio
- Evaluate for post-renal causes
- POCUS of kidneyes and bladder
- Flushing or changing IDC
- If oliguric, treat and assess for renal hypoperfusion:
- History review (e.g. diuresis, fluid balance)
- Perfusion evaluation (e.g. relative hypoperfusion, shock index, fluid responsiveness, Rush Exam)
- Resolve renal hypoperfusion:
- Volume excess + congestive nephropathy → diurese
- Volume depletion → fluid
- Cardiogenic shock → trial inotrope or inopressor
- Hypotension → trial noradrenaline
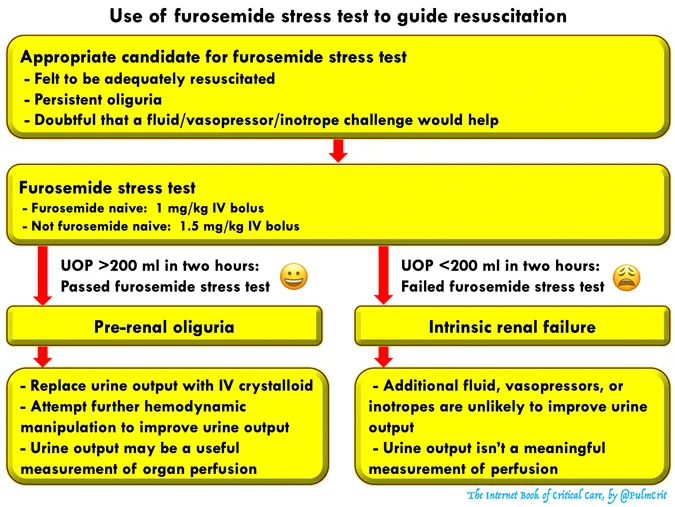
- If evaluation doesn’t suggest hypoperfusion or failure to improve urine output consider a furosemide stress test where adequate urine production following a furosemide stress tests suggests pre-renal aetiology and inadequate urine production suggests intrinsic renal failure
- If non-oliguric evaluate for intrinsic renal failure
Furosemide Stress Test
- Administration of a defined dose of furosemide:
- 1 mg/kg for patients who are furosemide naive.
- 1.5 mg/kg for patients with prior exposure to furosemide.
- Monitoring urine output
More than 200 ml within two hours indicates adequate response.
Management
- Treat the underlying cause as per diagnostic approach (above)
- Discontinue nephrotoxins and dose-adjust renally cleared medications
- Optimise haemodynamics
- Discontinue anti-hypertensives and negative inotropes
- Optimise vasopressors (MAP > 65 mmHg and MAP > 80 mmHg in patients with chronic hypertension or hepatorenal physiology)
- Consider a vasopressor challenge
- Fluids management
- Fluid is beneficial under the following circumstances:
- Pre-renal AKI
- Patient is fluid responsive
- Patient is hypovolaemic
- Hypovolaemia + uraemic acidosis give isotonic bicarbonate (5% dextrose with 150 mEq/L sodium bicarbonate)
- Hypovolaemia + normal bicarbonate give a balancved crystalloid (e.g. hartmann’s or plasmalyte); avoid normal saline
- Fluid is beneficial under the following circumstances:
- Potassium management
- Replace potassium conservatively targeting > 3.5 mmol
- Renal diet to reduce potassium intake
- Treat hyperkalaemia if present
- Acid-Base support
- Providing bicarbonate for uraemic acidosis aiming for a pH > 7.2
- Can be given as:
- Isotonic bicarbonate (glucose 5% with 150 mEq/L ) in patients who are hypovolaemic
- Hypertonic bicarbonate ampules (50 mL ampules of 1 mEq/mL bicarbonate) in patients who are hyponatraemic
- Oral bicarbonate tablets
- Phosphate binding
- If phosphate > 1.94 mmol/L treat with calcium acetate (in hypocalcaemic patients) or sevelamer
- Haemodialysis
- Indicated for patients with
- Acidosis refractory to IV bicarbonate
- Diuresis-refractory electrolyte abnormalities (e.g. hyperkalaemia)
- Fluid overload refractory to diuretics
- Symptoms of uraemia (e.g. delirium, asterixis, pericardial effusion)
- Indicated for patients with
Hepatorenal Syndrome
- Clinical presentation:
- Typically in advanced cirrhosis with ascites but also in acute liver failure or alcoholic hepatitis especially those with chronic hypotension and hyponatraemia (i.e. borderline perfusion due to vasodilation)
- A precipitating factor may be present such as a haemodynamic stressor (e.g. infection, volume depletion or overload) or deterioration in liver function (e.g. acute on chronic liver failure)
- Presentation is one with oliguria and bland urine sediment findings (i.e. no evidence of glomerulonephritis or tubular necrosis)
- In addition to the above management options consider:
- Albumin
- Vasopressors (noradrenaline remains first line)
- Aim MAP > 15 mmHg above baseline
- Therapeutic large volume paracentesis
NOTE
- Importantly, these patients have low muscle mass and enhanced renal creatinine secretion leading to artificially low creatinine values; therefore:
- Creatinine level tends to over-estimate renal function
- Small changes in creatinine may be significant and meet AKI criteria
Source
- Acute Kidney Injury (including HRS-AKI) - EMCrit Project
- Acute Kidney Injury • LITFL • CCC Renal
- Deranged Physiology:
Footnotes
-
IBCC says that fractional excretion of sodium performs poorly in differentiating pre-renal and intrinsic renal failure ↩