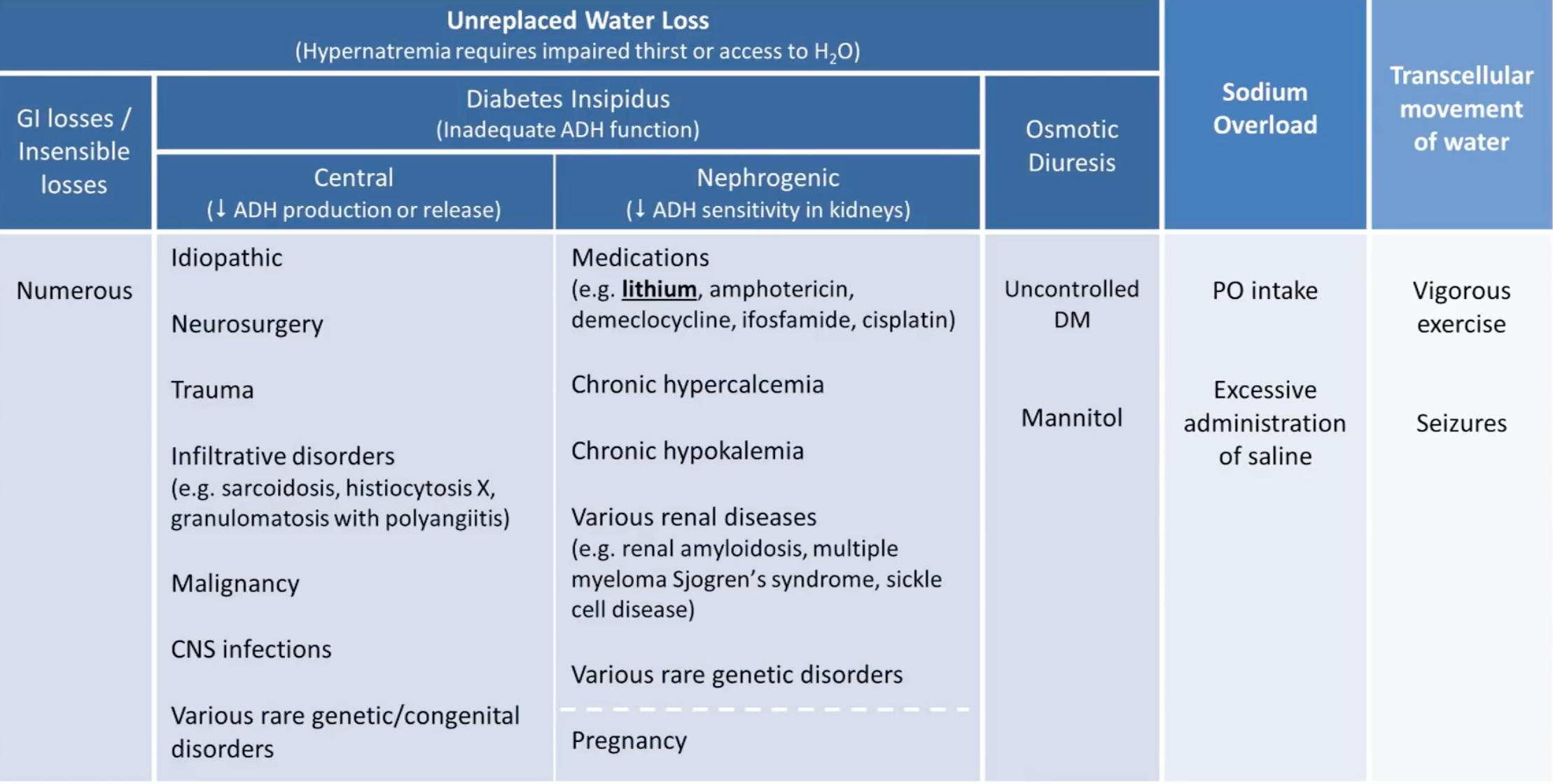
Aetiologies
Clinical Features
- Similar to Hyponatraemia, mostly neurological:
- Increased temperature
- Restlessness
- Irritability
- Confusion
- Drowsiness
- Coma
- Seizures
- Subarachnoid haemorrhage (due to brain shrinkage and vascular rupture)
Workup
- Consider history
- Loss of solute poor water + primary neurologic disease or lack of access to water
- As a result most patients are very young or very old
- Urine osmolality
- Low urine osmolality (<300 mOsm/kg): Diabetes insipidus
- High urine osmolality (>600 mOsm/kg): impaired thirst or access to water
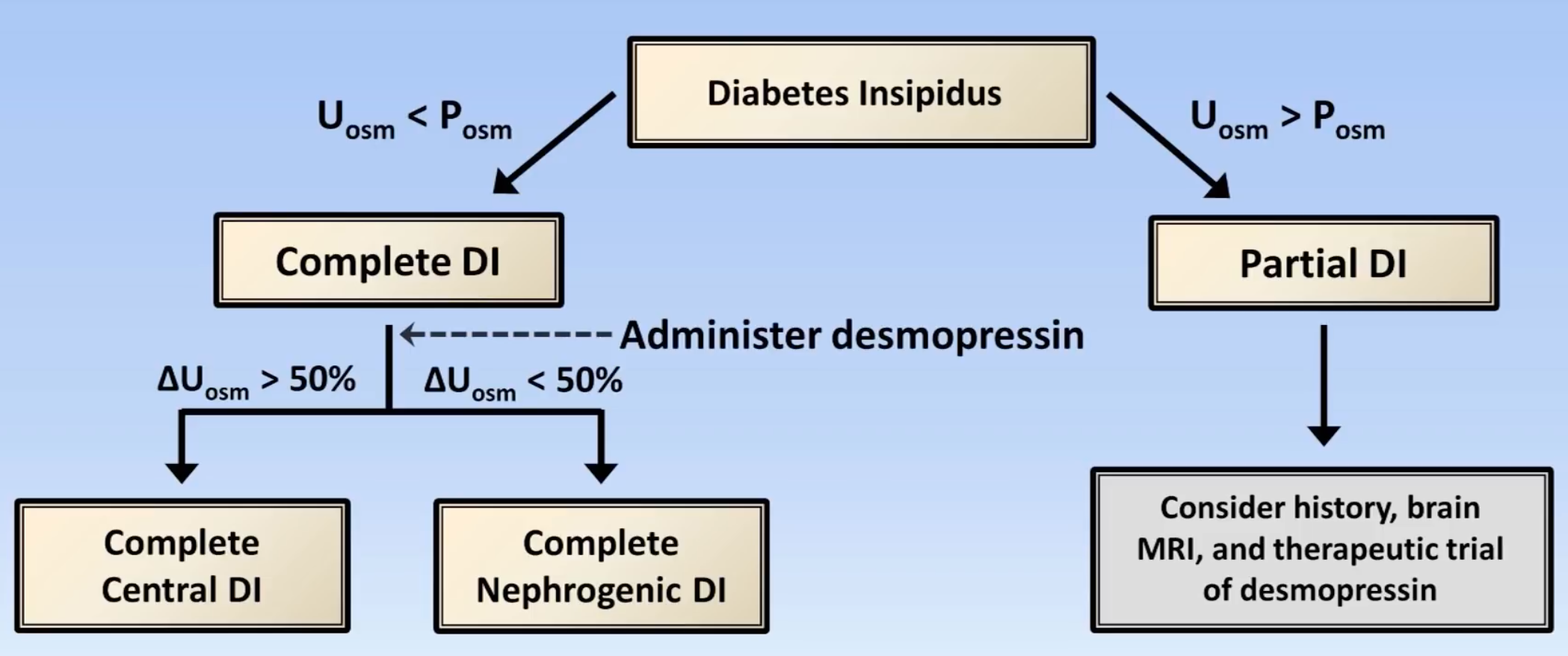
- If Diabetes insipidus, determine type using response to administration of desmopressin
Management
- Chronic hypernatraemia (>48 hours): correction rate ≤10 mmol/L each 24 hours
- Acute hypernatraemia (<48 hours): correction to normal over 24 hour period
- Choice of fluid
- Normal saline should be used only as initial therapy in patients with end-organ dysfunction secondary to depletion
- 5% glucose should be used in situations of pure water loss (e.g. Diabetes insipidus)
- Hypotonic fluid (e.g. half normal saline, quarter normal saline) should be used in situations with hypotonic fluid losses (e.g. diarrhoea)
- Calculate rate
EXAMPLE
An 85 year old woman 70kg with dementia develops diarrhoea while living at a nursing facility. After 4 days, she is unrousable by staff and brought to the emergency department. She appears hypovolaemic on examination and has a serum sodium of 170 mmol/L and a serum potassium of 2.8 mmol/L. What rate of what fluid should be chosen to correct this?
- Hypotonic fluid loss without mention of end-organ dysfunction with hypokalaemia ⇒ 1/2 normal saline + 20 mmol/L
- Rate calculation as follows:
To reduce her sodium by 5 mmol/L over 12 hours, we would therefore need to give of fluid. To account for ongoing losses via diarrhoea, we might want to give another 1 L resulting in a total of 3.3 L over 12 hours giving an infusion rate of 275 mL/hr
Example
A 45 year old 75kg man with diabetes insipidus presents tot he hospital after 4 days of worsening abdominal pain and fever. He is in early shock with HR 115, BP 85/55, creatinine of 140 and undetectable JVP. His serum sodium on presentation is 165 mmol/L. What is the appropriate IV fluid therapy?
- Bolus of isotonic fluid to restore haemodynamics (e.g. MAP > 60 mmHg, urine output > 30 mL/hr) ⇒ 1 L normal saline every 30 minutes x 4 L
- Appropriate fluid in diabetes insipidus is glucose 5%
- Calculate the expected sodium change per litre of glucose 5%:
To reduce sodium by 5 mmol/L over 12 hours, we therefore need to give of fluid. To account for ongoing losses due to DI, we might want to give another 2L, for a total of 3.2 L over 12 hours which is approximately 260 mL/hr
- We can therefore give both fluids simultaneously or give the boluses of normal saline first then the glucose 5%
- Alternatively and much easily use the free water calculator on MDCalc making sure to plugin in an appropriate desired sodium target (i.e. 10 mmol/24 hours)
- Assess volume status and resuscitate appropriately with normal saline
- Establish acute vs chronic to determine rate (acute ≈ 1 mmol/L/hr and chronic < 24 mmol/L over 24 hours); when in doubt assume chronic
- Set a safe 24-hour target sodium (i.e. in chronic )
- Use this as the sodium desired value in the above calculator in MDCalc
- Divide this volume by 24 hours to get the mL/hr of pure free water
- Add maintenance and ongoing free water losses
- Insensible losses (skin + respiratory) is roughly 0.5-1 mL/kg/hr and are electrolyte free so also contribute to hypernatraemia
- Add 10% per °C above 37°C for fever, and more for tachypnoea, burns, open abdomen or unhumidified ventilation
- Determine the electrolyte free water clearance by the kidney
- A positive EFWC is the volume of pure water the kidney is dumping per unit time and should be matched by the IVF replacement
- Do not add isotonic losses to this (e.g. GI output, drain fluid, blood)
- Insensible losses (skin + respiratory) is roughly 0.5-1 mL/kg/hr and are electrolyte free so also contribute to hypernatraemia
- Adjust this for the fluid’s actual free-water fraction: 5% dextrose = 1.0 (rate unchanged), 0.45% saline = 0.5 (double it), 0.18–0.225% saline = ~0.75. This gives the volume of that fluid to run
- For example, 2.8L of free water over 24h via 0.45% saline is or 230 mL/hr
- Cross check with formula above
- Recheck sodium at 4-6 hours and titrate
Sources
- Youtube Videos
- Deranged Physiology: Hypernatraemia