Setup
- Ensure probe marker is on the right of the image to indicate that the echocardiogram is in ‘cardiac mode’ and not ‘standard mode’
- The left ventricle should always be on the left of the screen in parasternal long-axis view
- Can ask the patient to lay on the left lateral decubitus position
Approach
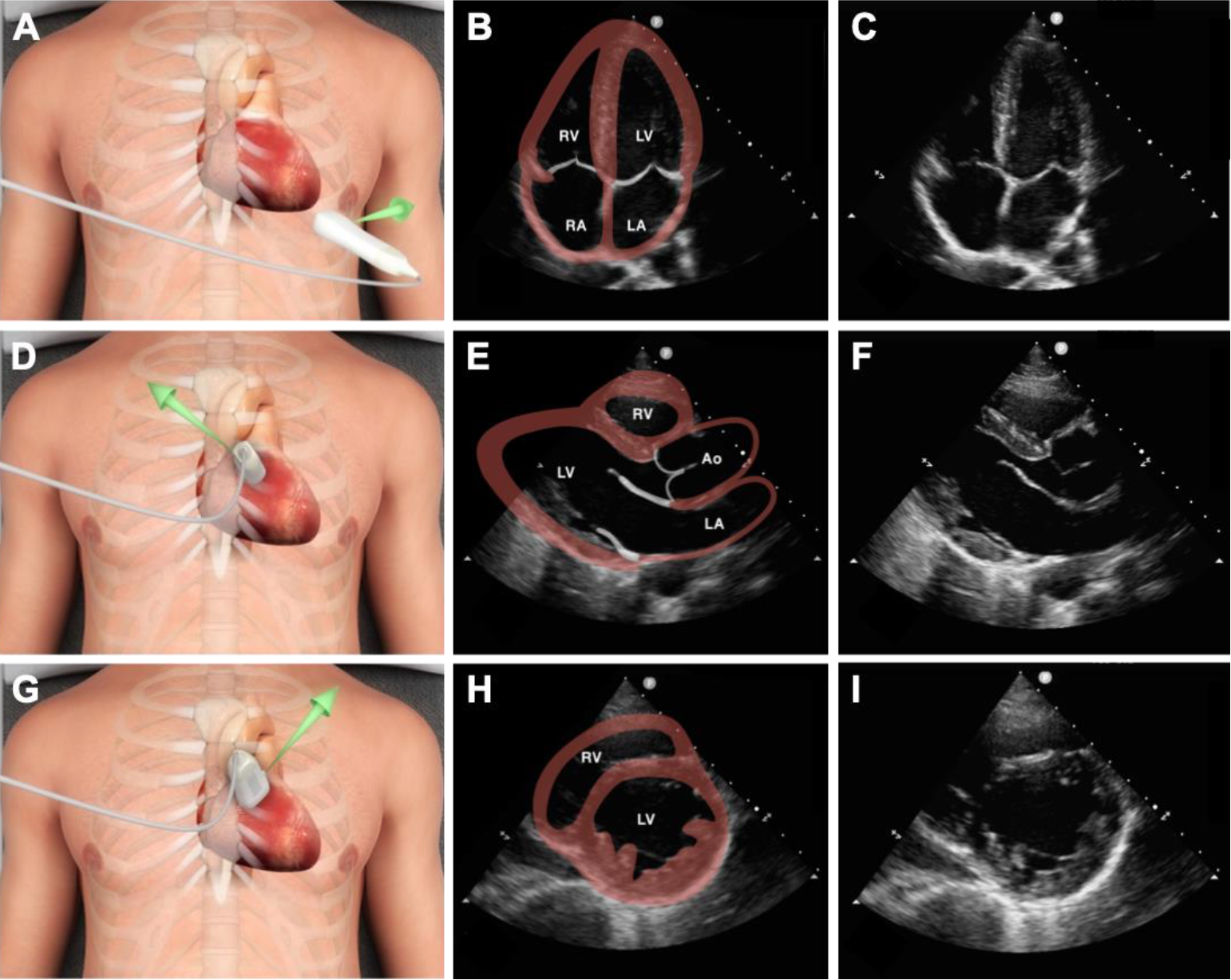
- Parasternal long axis
- Parasternal short axis
- Apical 4 chamber
- Sub-xiphoid
Focused Cardiac Echocardiography
- If possible place the patient in the left lateral decubitus position before beginning
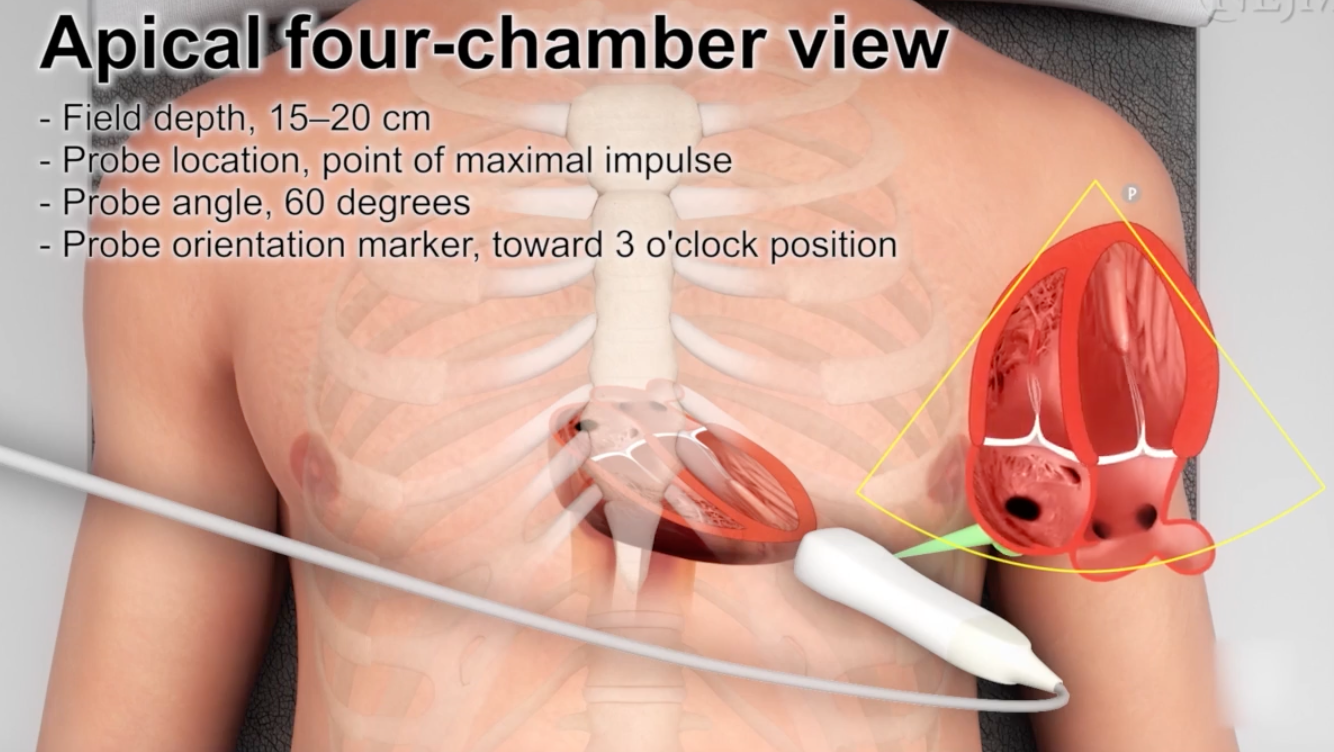
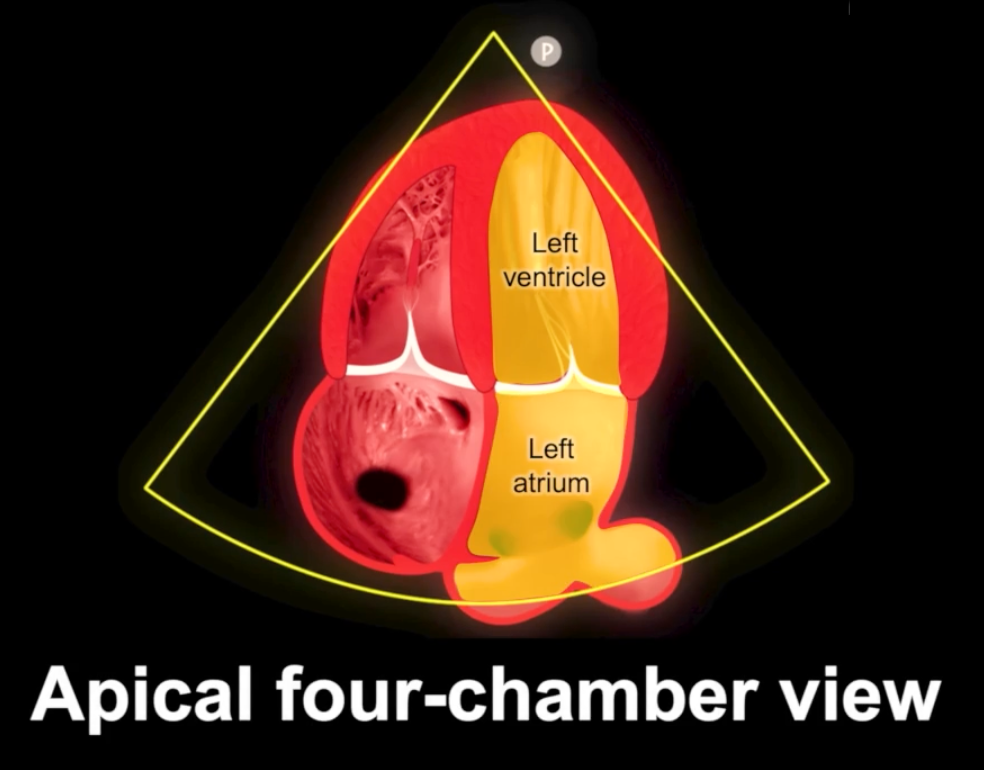
Apical Four Chamber View
-
Set field depth to 15-20 cm
-
Place the probe at:
- The point of maximal impulse or
- Anterior axillary line and move towards the nipple in a Z shape pattern
-
Probably easier to go from the para-sternal short axis to the apical four chamber:
- Point the probe marker towards the left axilla
- Slide down toward the apex and you should see the chamber size getting smaller and smaller
- When you get to the apex, fan up towards the patient’s head
-
Keep the probe at 60 degrees relative to the chest wall with the orientation marker pointing towards the 3 o’clock position
-
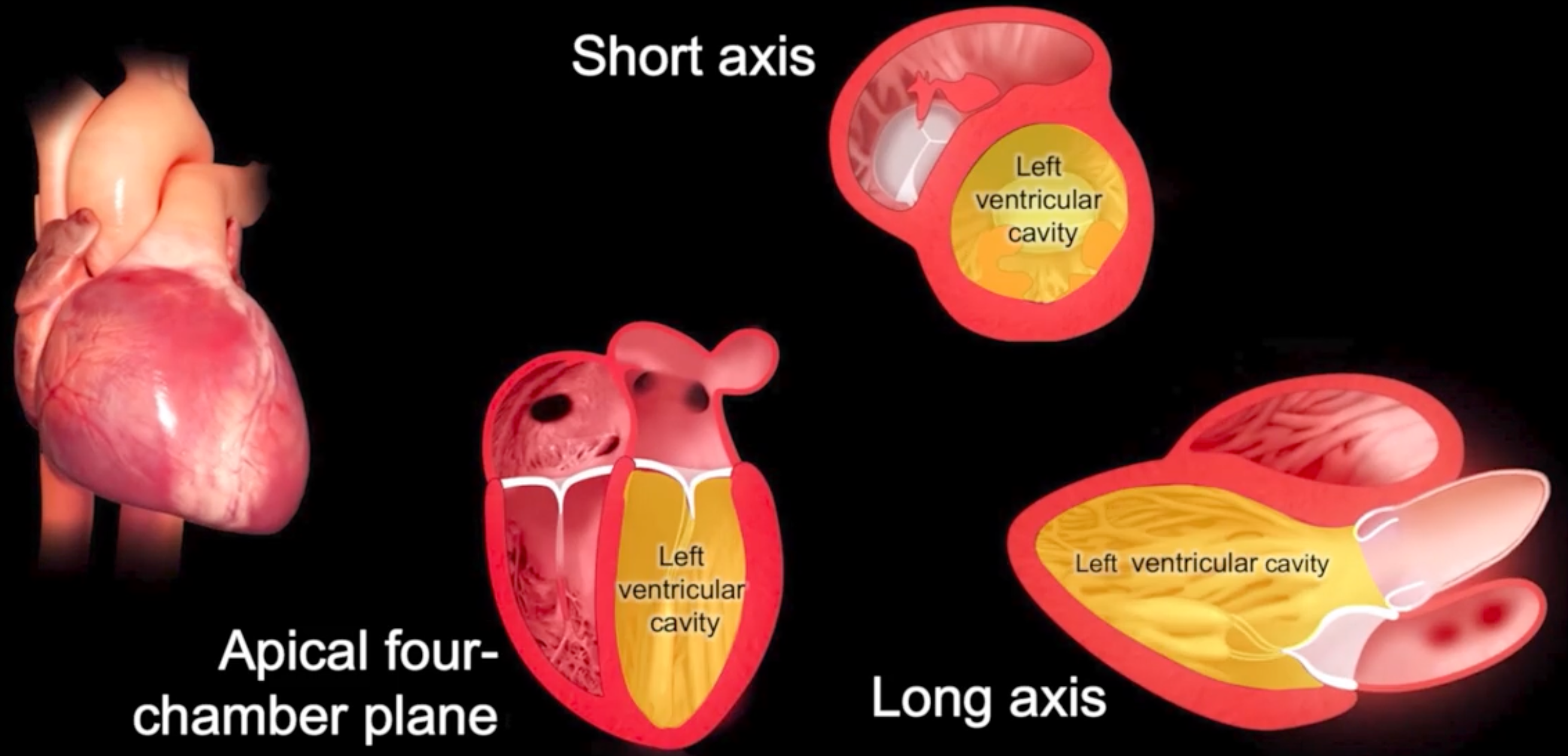
Identify the structures of interest:
- Lateral and septal mitral annulae
- Apex
- Endocardial and epicardial borders
-
In this view the LV should take up 2/3 and the RV should take up 1/3
- Use this view to assess longitudinal shortening with a ruler or M-mode vector line
- Then assess thickening of wall segments
- Then assess change in left ventricular cavity area
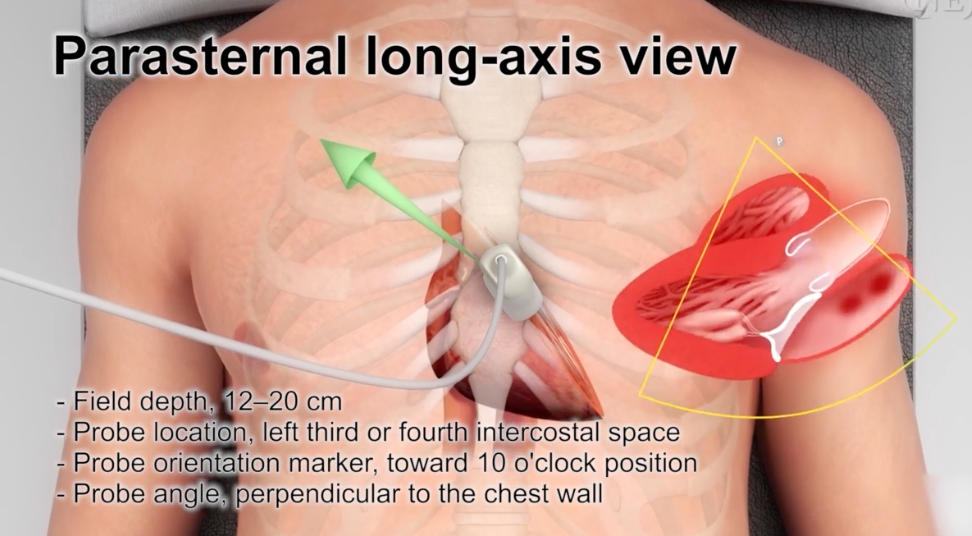
Parasternal Long Axis
- Set the field depth to 12-20 cm
- Place the probe at the the left third or fourth intercostal space
- Point the orientation marker toward the 10 o’clock position (right shoulder) with the probe perpendicular to the chest wall
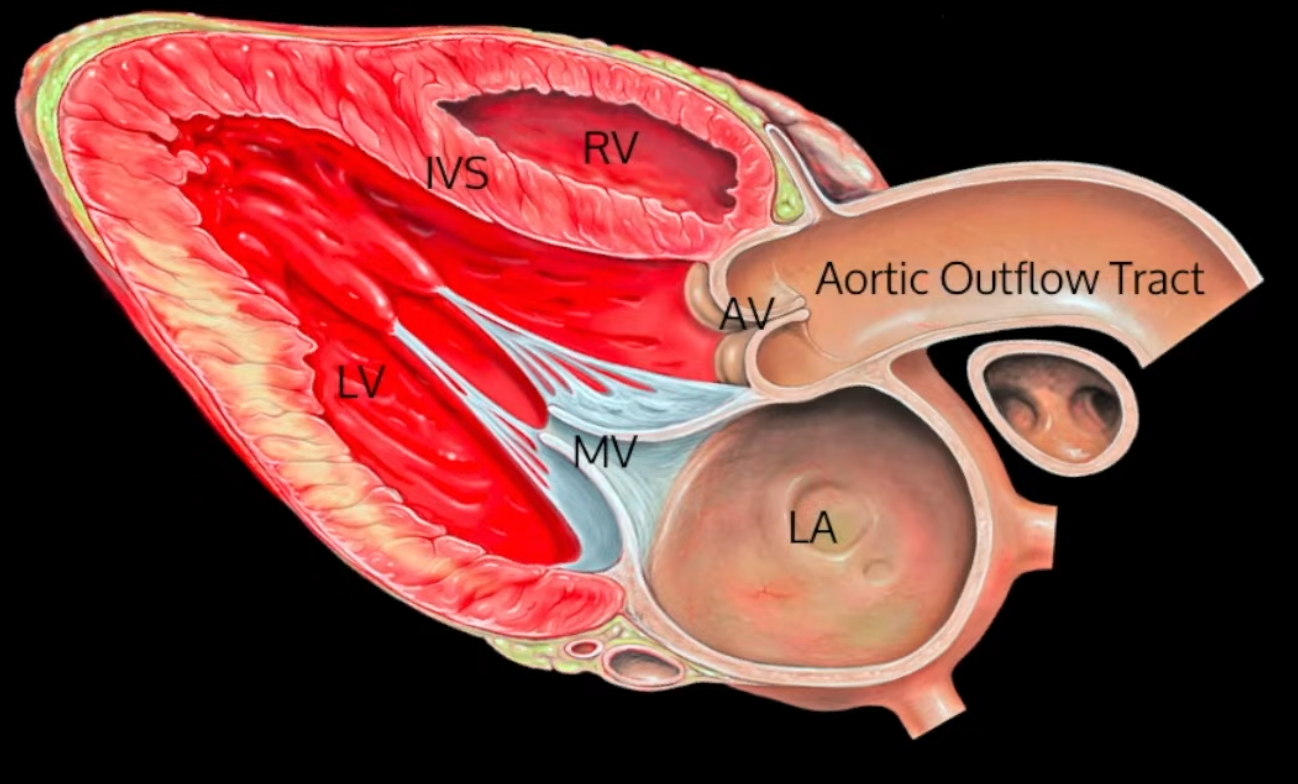
- Identify the areas of interest including:
- Anterior mitral-valve leaflet
- Endocardial and epicardial borders
- Midline of the left ventricular cavity
- Assess anterior mitral valve leaflet motion, wall thickening, area of cavity change and longitudinal shortening
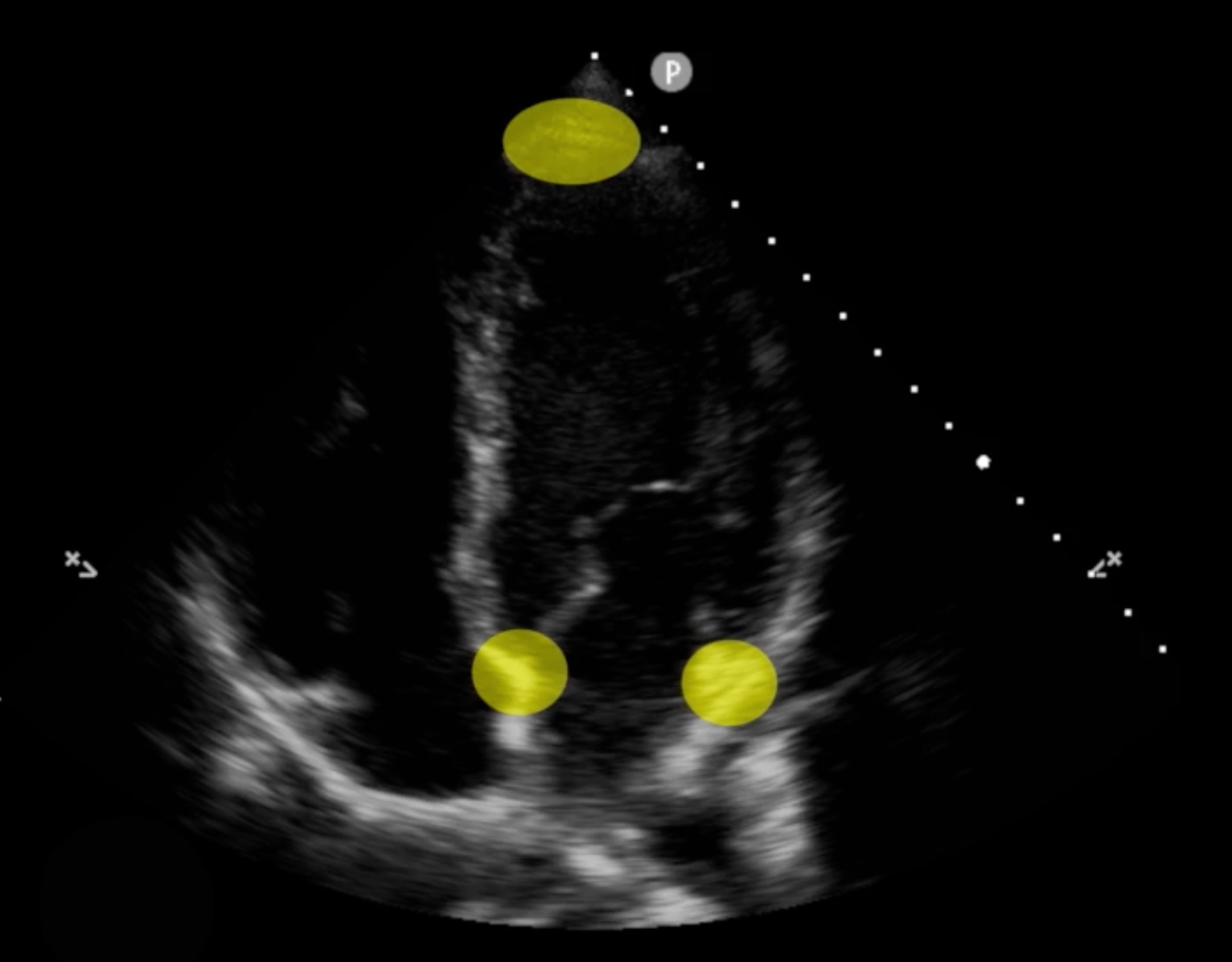
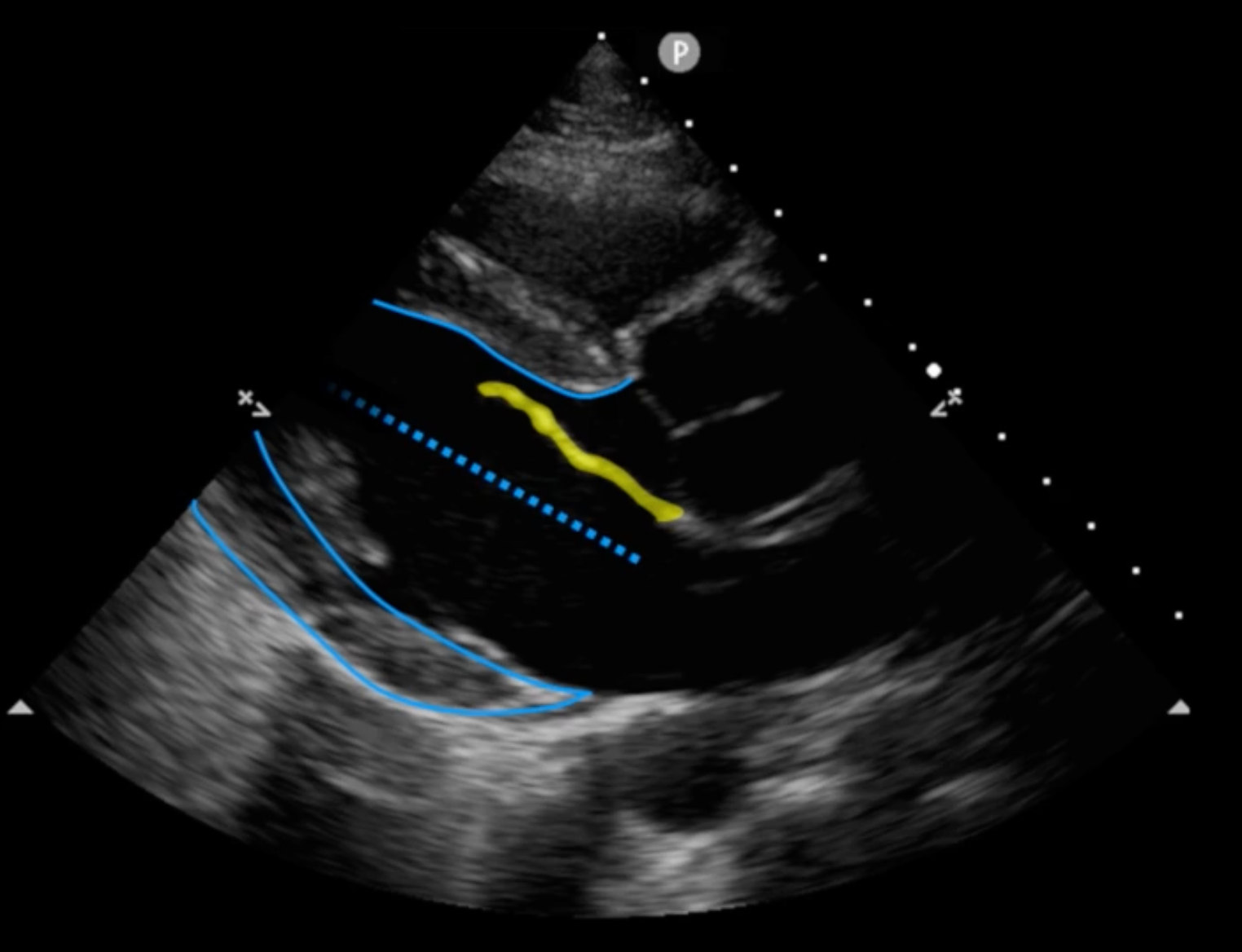
- One can quantify the EF in this view by taking the M-mode line across the mitral valve septum:
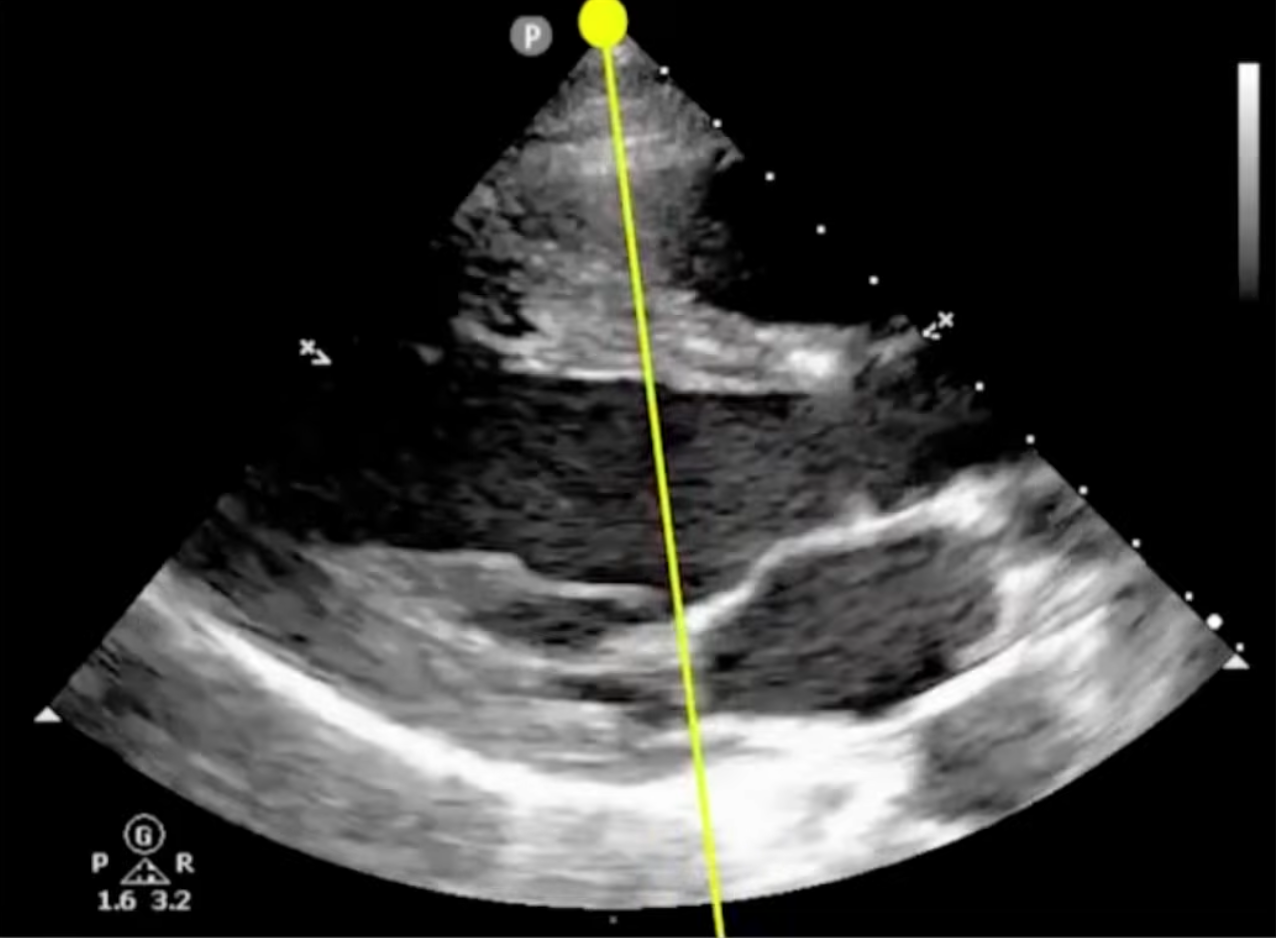
- Freeze the frame and identify:
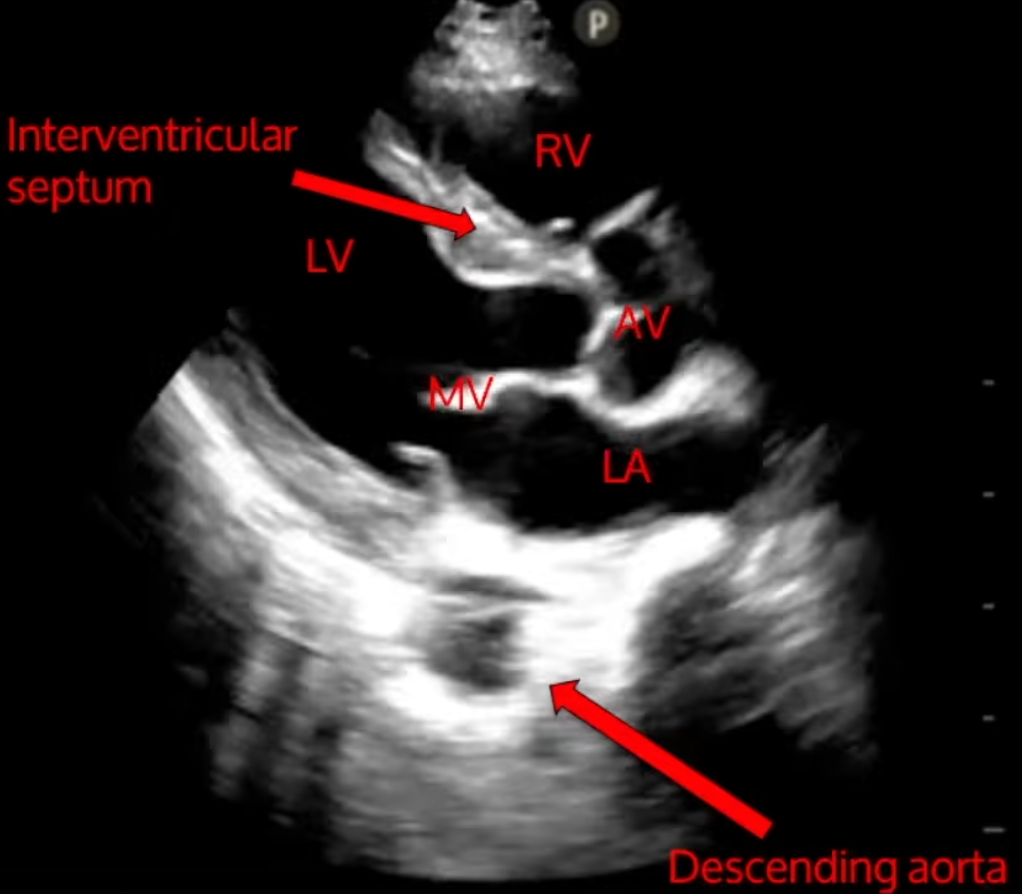
- interventricular septum and mitral valve
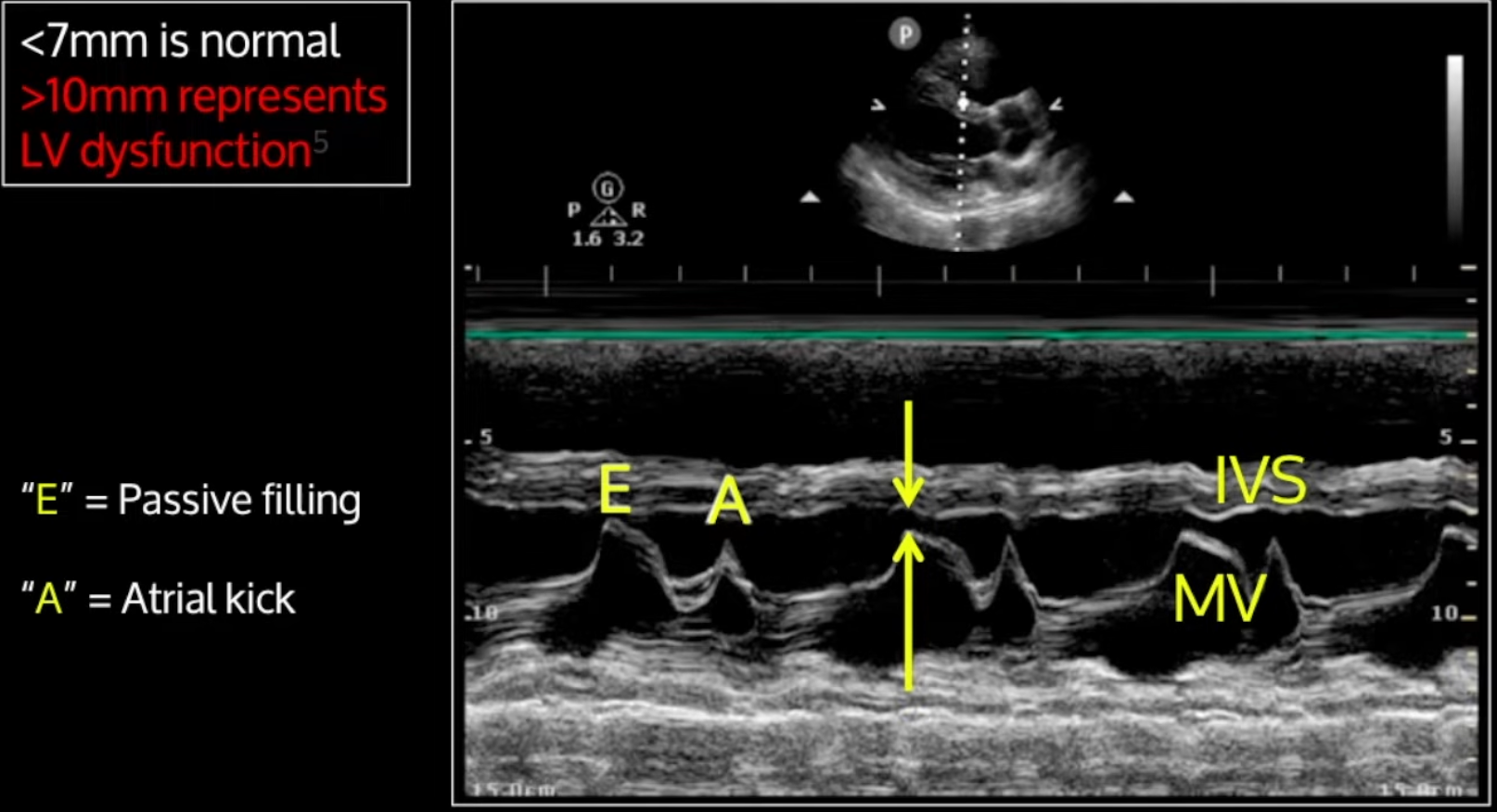
- The distance between the mitral valve and the interventricular septum can be used to observe for LV dysfunction <7 mm is normal and >10 mm represents dysfunction
- This study is susceptible to aortic regurgitation and mitral stenosis which will falsely predict LV dysfunction
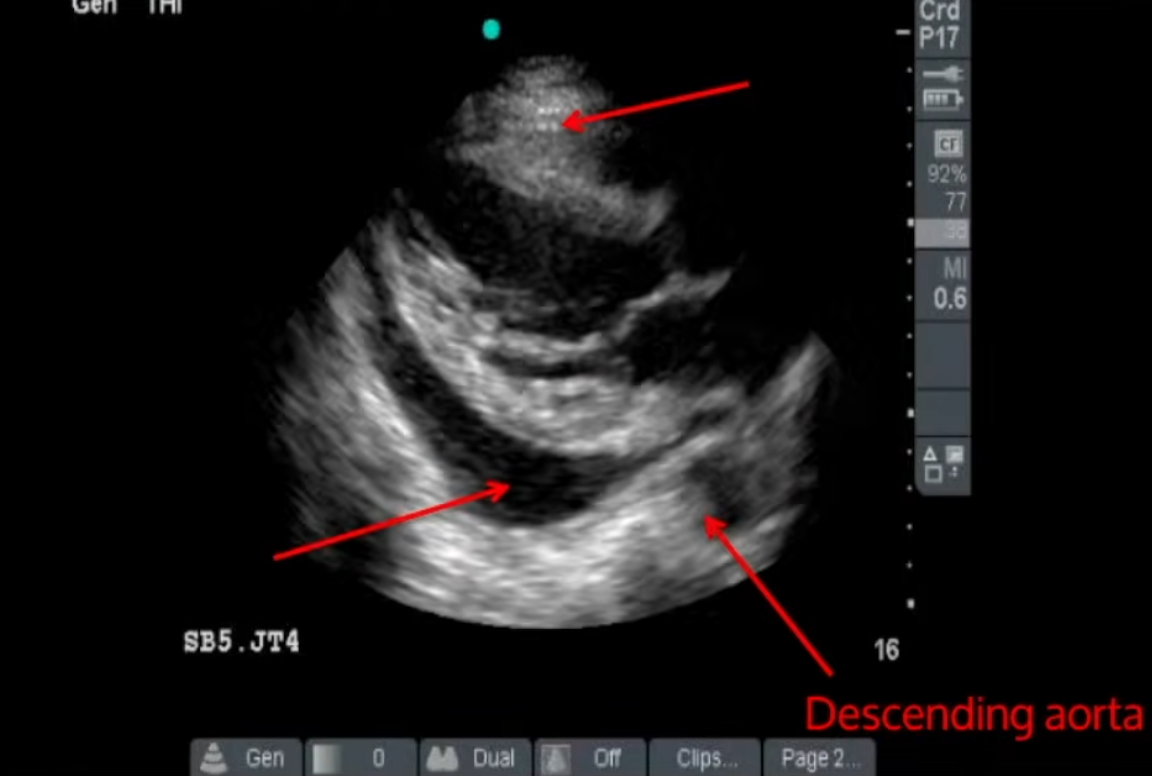
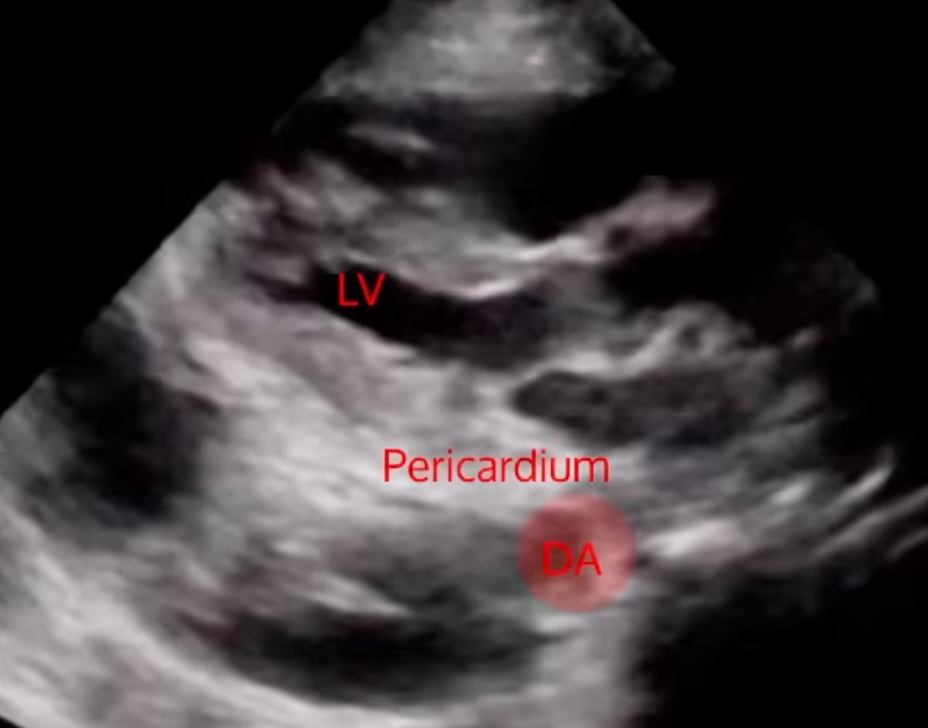
- This view can be used to differentiate a pericardial effusion from a pleural effusion
- A pericardial effusion will show fluid build up anterior to the descending aorta
- A pleural effusion will show fluid build up posterior to the descending aorta
- A pericardial effusion will show fluid build up anterior to the descending aorta
- Pericardial tamponade
- Requires diastolic collapse of the right ventricle with clinical symptoms (e.g. hypotension, tachycardia, chest pain)
- Can identify that collapse of the RV occurs during diastole as during this point in time the mitral valve leaflets are open
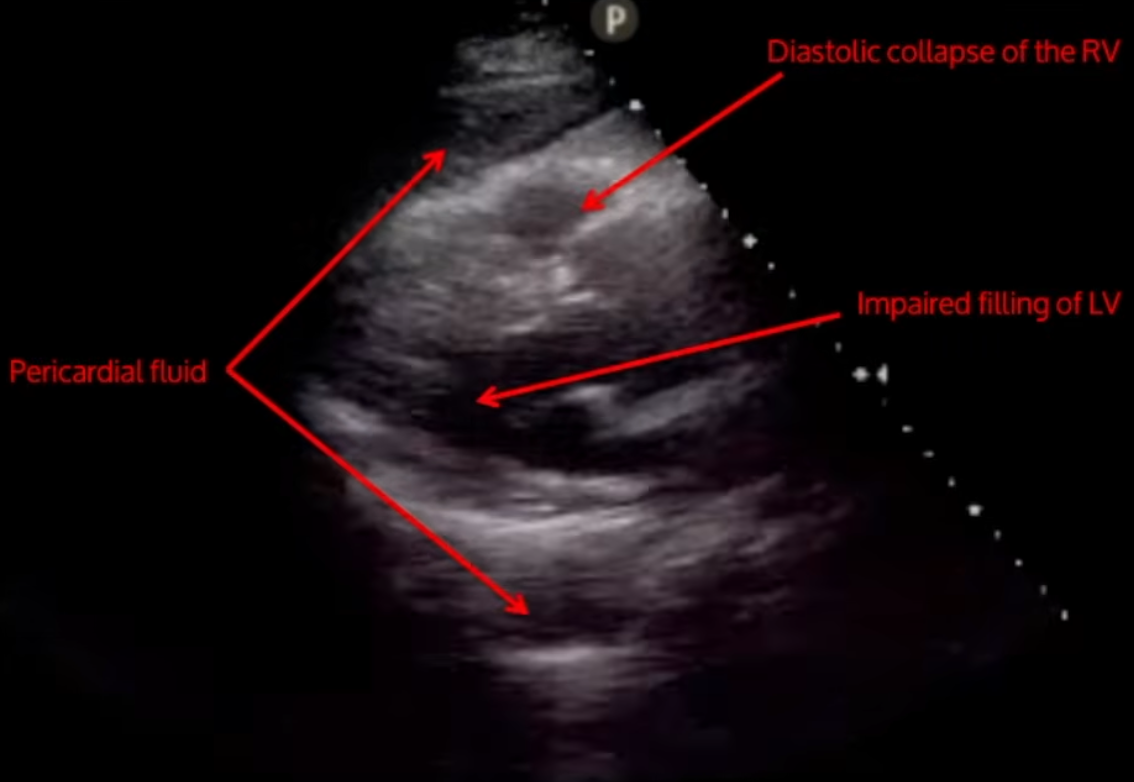
- Requires diastolic collapse of the right ventricle with clinical symptoms (e.g. hypotension, tachycardia, chest pain)
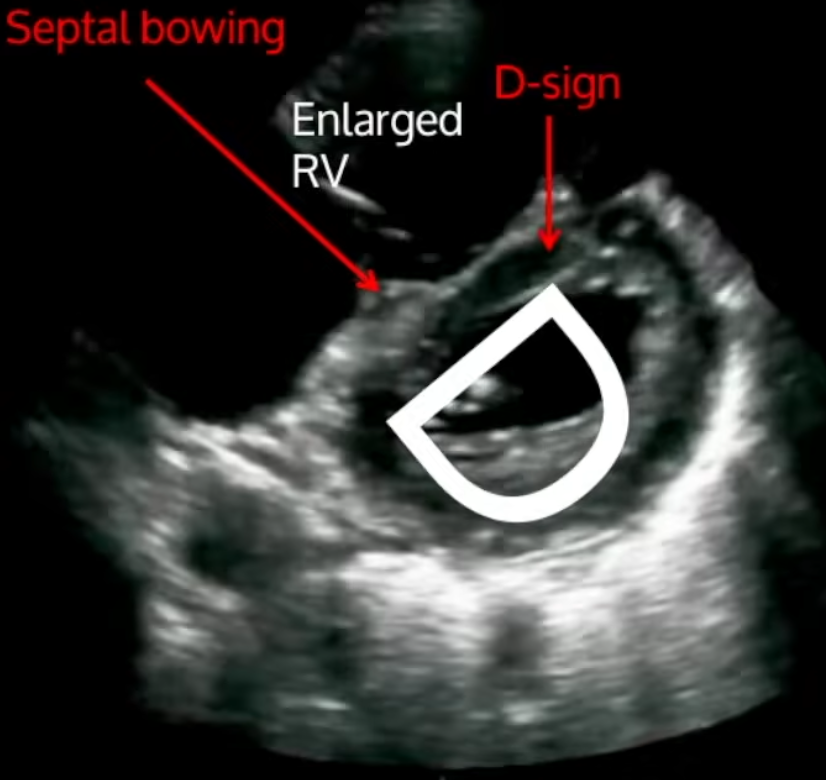
- RV strain
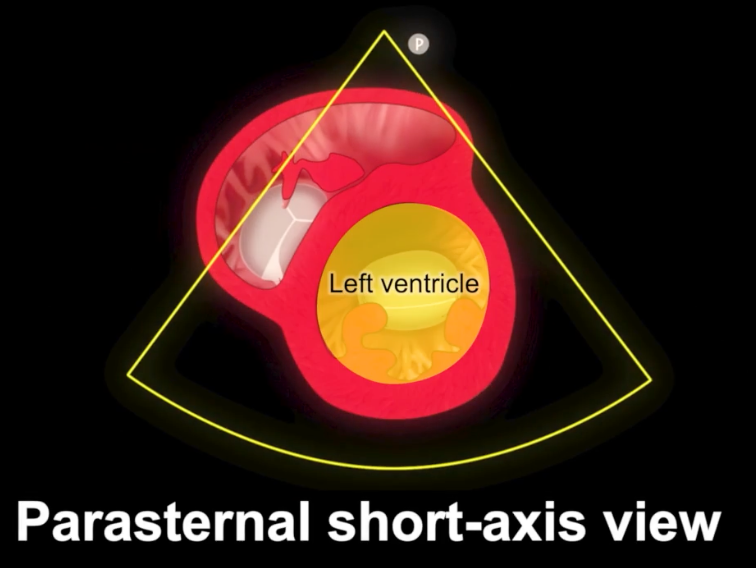
Parasternal Short Axis
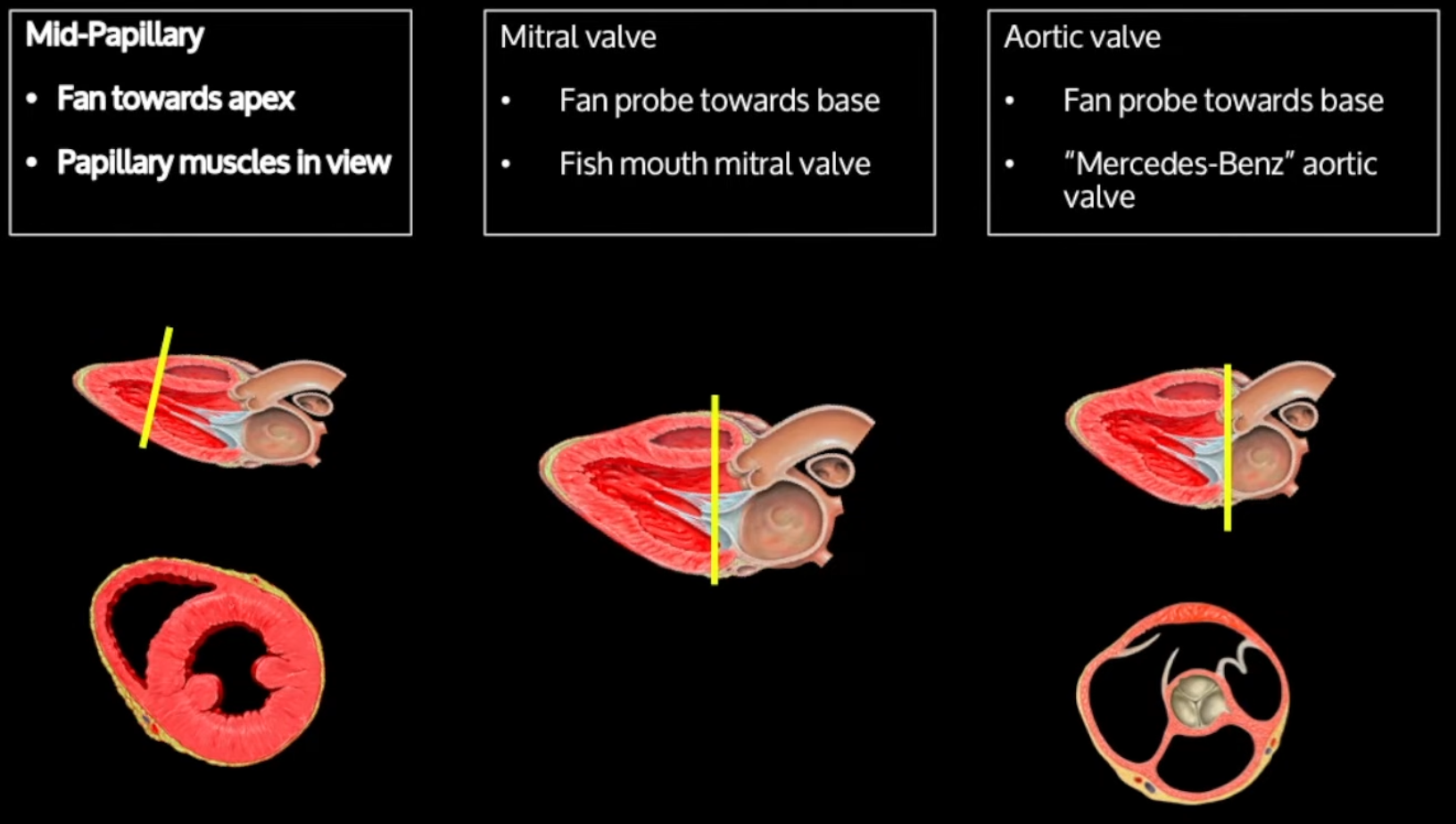
- First obtain the long axis view (above), then point the orientation marker toward the 2 o’clock position (left shoulder), fan towards the apex and base and decrease the field of depth to 10-14 cm
-
Identify the structures of interest:
- Endocardial and epicardial borders
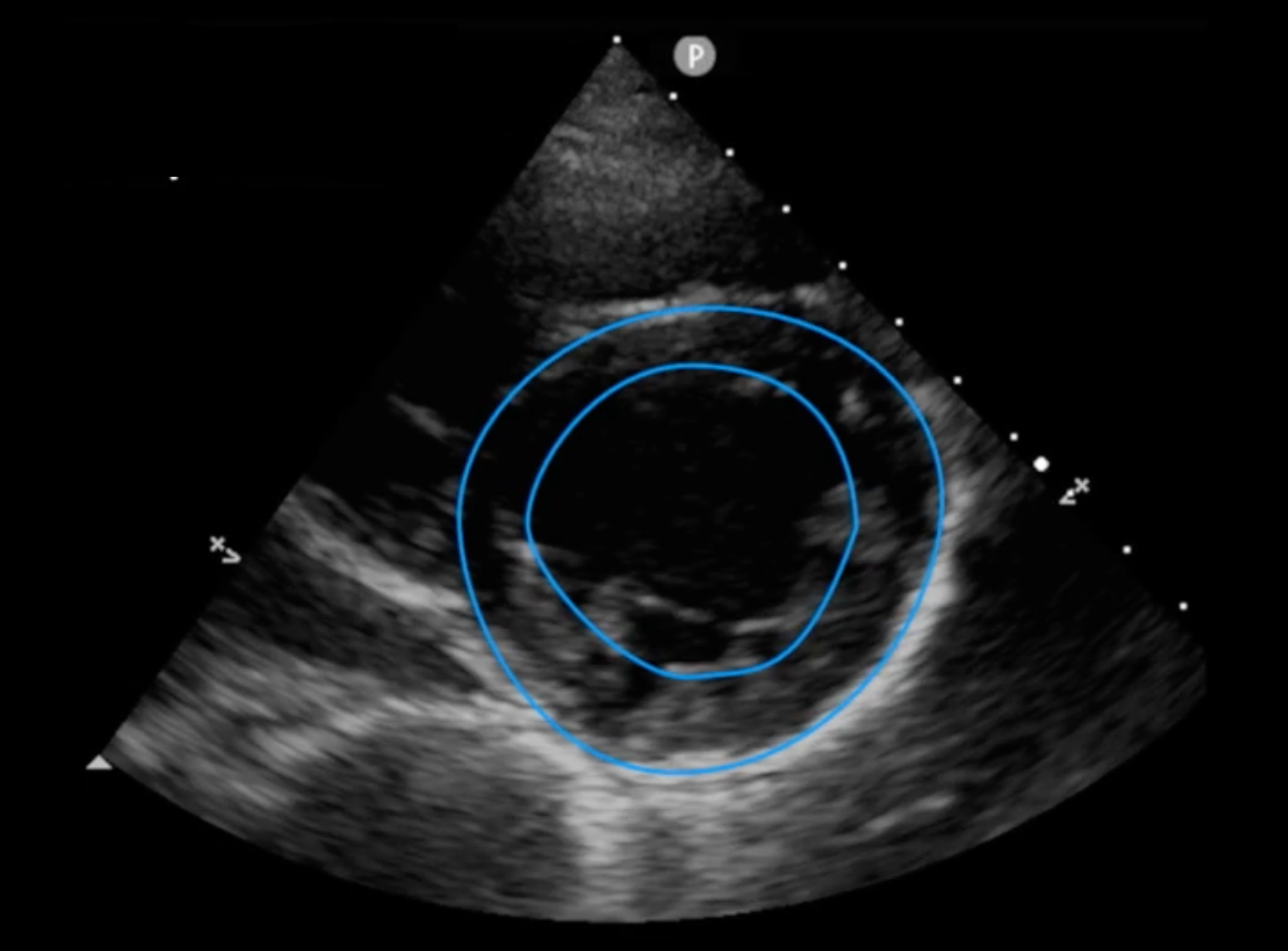
- Endocardial and epicardial borders
-
Assess wall thickening and change in area of cavity
-
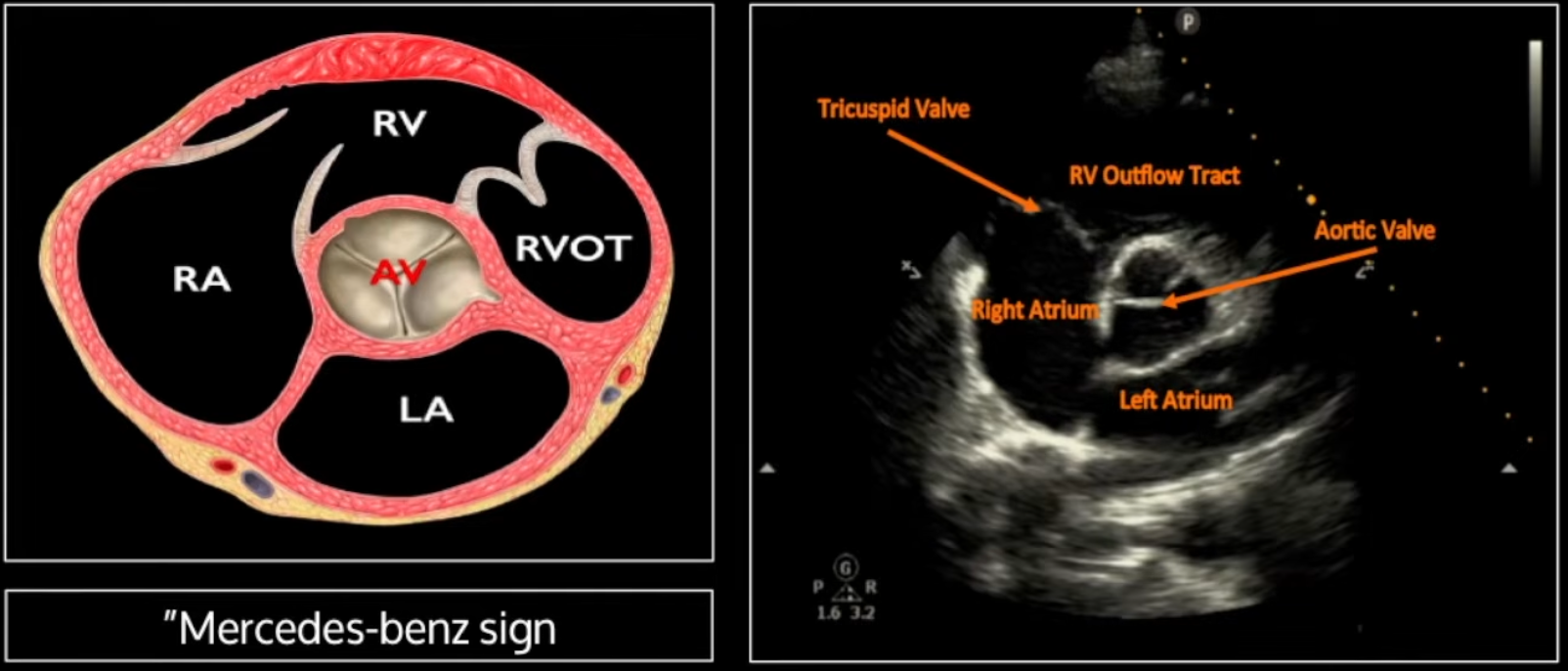
Can go more superiorly (towards the base) to see the aortic valve in its classic mercedes-benz sign configuration
-
-
Can also assess for right ventricular strain
- In RV strain will see: enlarged RV and septal bowing causing the LV to take the appearance of a ‘D’
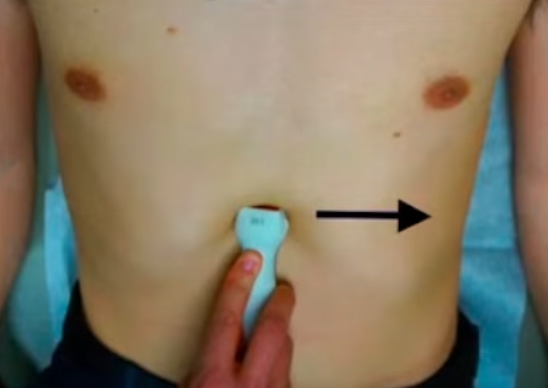
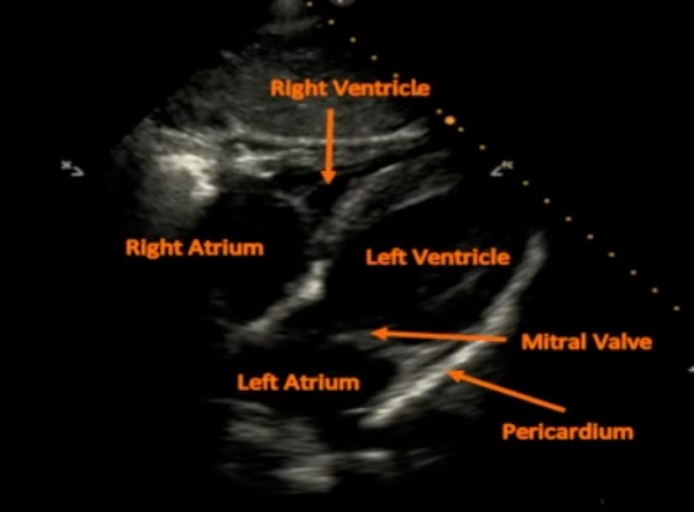
Subxiphoid View
- With patient’s knees bent place the probe in the subxiphoid region with the indicator to the left
- Use an overhand grip on the probe to obtain a lower angle (probe is almost parallel to the skin)
- Start on the patient’s right, identify the liver and sweep to the left using the liver as an acoustic window
Echocardiographic Measures of Left Ventricular Systolic Function
- If all 4 measures (below) are normal, it is reasonable to grade the estimated left ventricular systolic function as normal (with LVEF > 55%)
- If all 4 measures (below) are abnromal, it is reasonable to grade the estimated left ventricular systolic function as abnormal (with LVEF < 30%)
Longitudinal Shortening
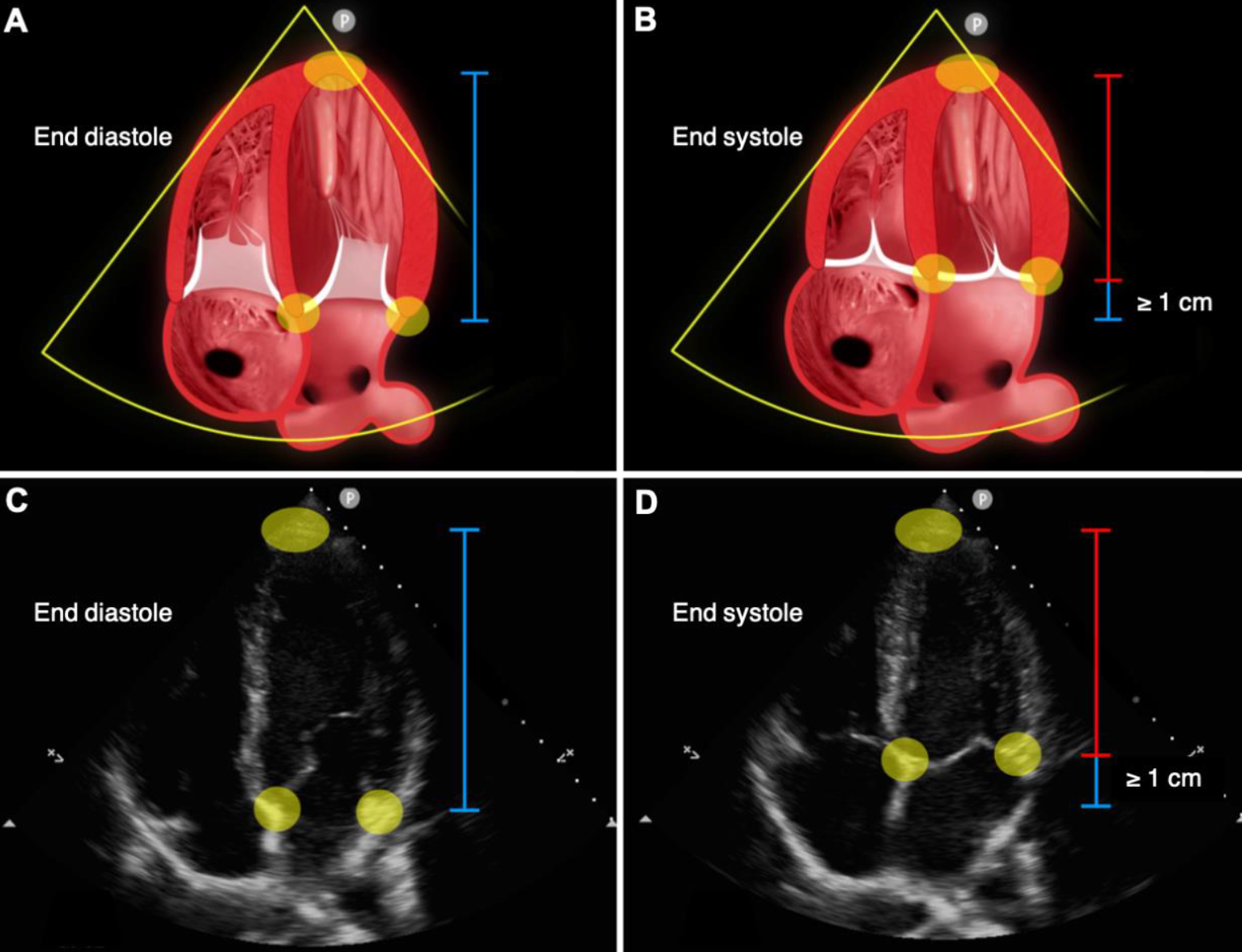
- Best evaluated int he apical 4 chamber view but should also be evaluated in the parasternal long axis view
- Identify a segment between the base (lateral and septal mitral annulae used as reference) and the apex of the heart
- Compare maximum length at end-diastole and end-systole using a ruler or M-mode vector lien
- A difference of ≥1 cm indicates normal left ventricular systolic function
Anterior Mitral-Leaflet Motion
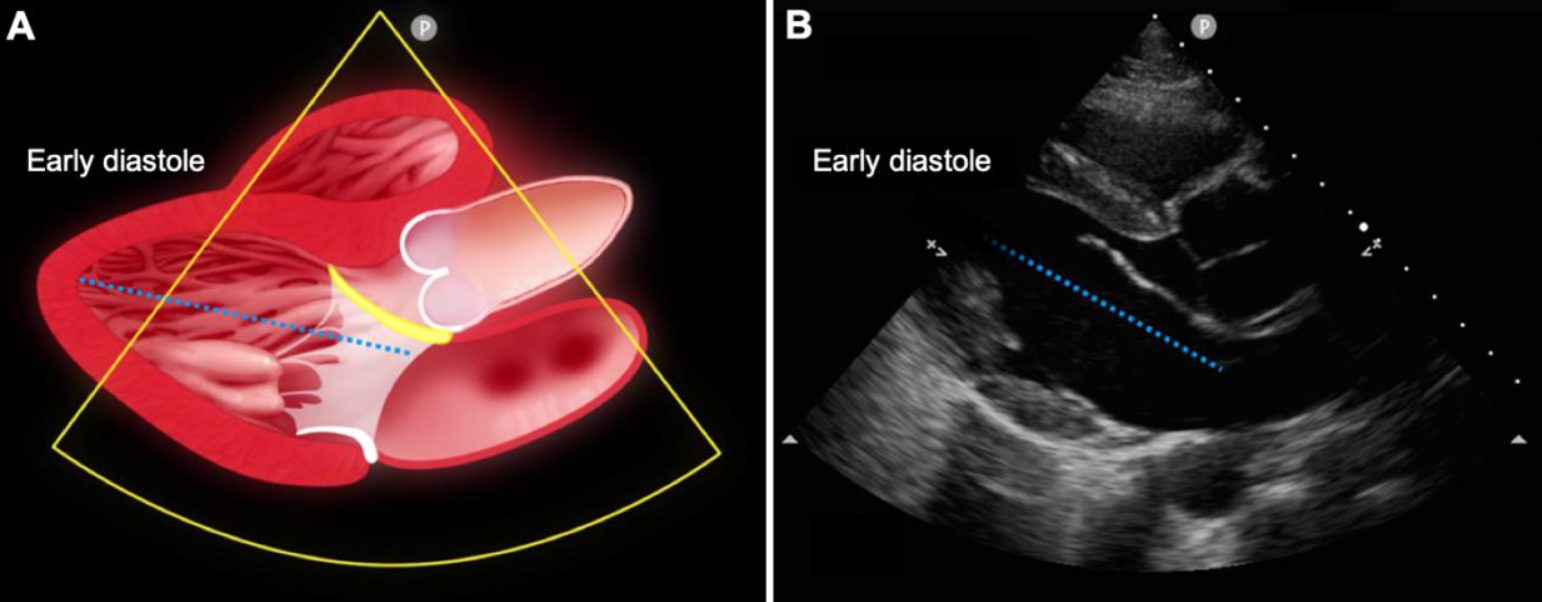
- Can only be evaluated int he parasternal long-axis view
- Imagine a line from the base to the apex of the heart along the midline of the left ventricular cavity
- In early diastole, the mitral valve leaflets separate widely
- When the anterior leaflet extends beyond the midline, it indicates normal left ventricular systolic function
- When it does not, it suggests severely reduced left ventricular systolic function
Thickening of Wall Segments
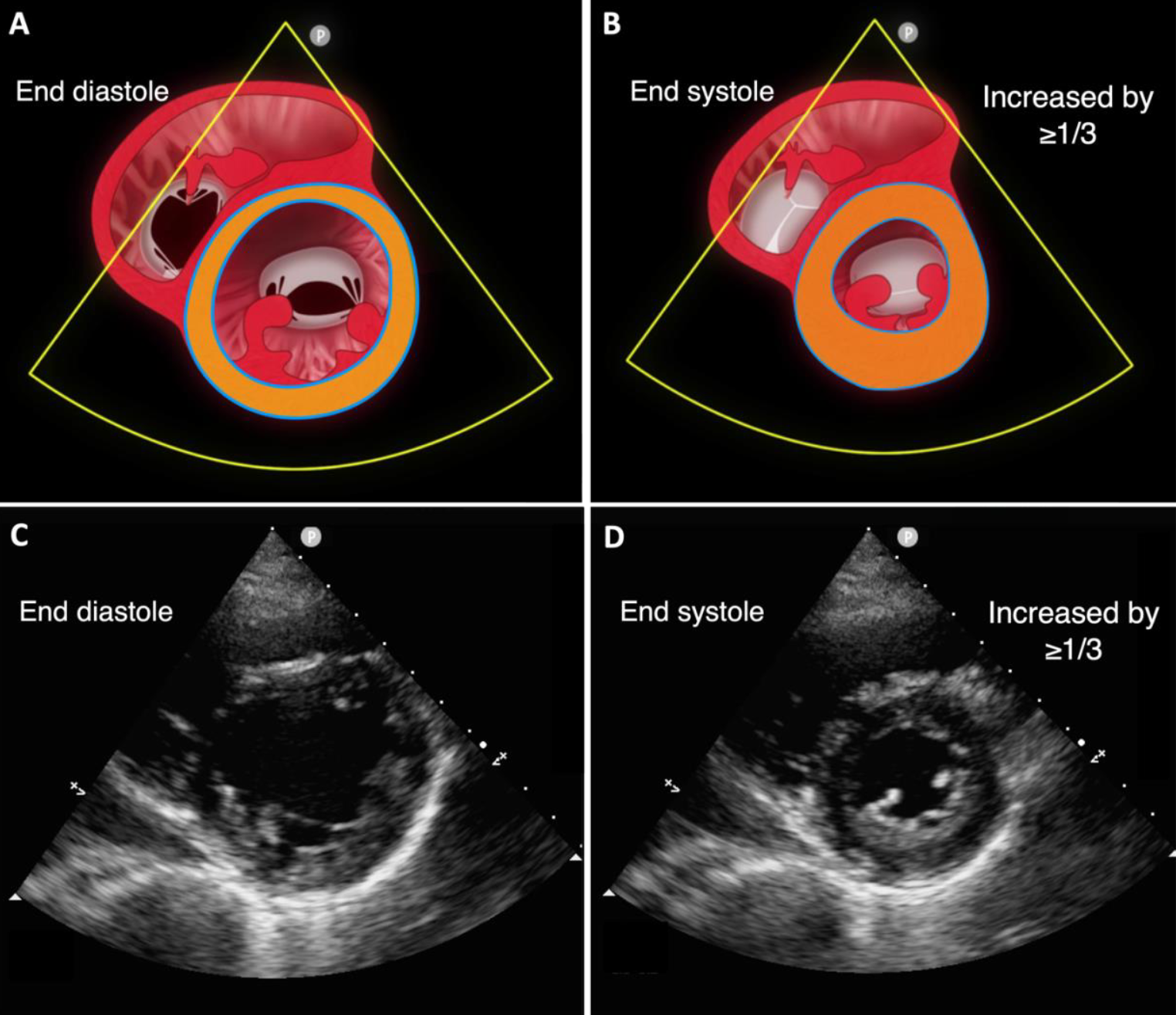
- Best assessed in the parasternal short axis view but should also be assessed in the parasternal long axis and apical four chamber views
- Wall thickness is minimal at end-diastole; during systole contraction of the myocardium causes wall thickness to increase
- Uniform wall thickening with an increase in wall thickness by at least ≥1/3 indicates normal left ventricular systolic function
Change in the Area of the Cavity
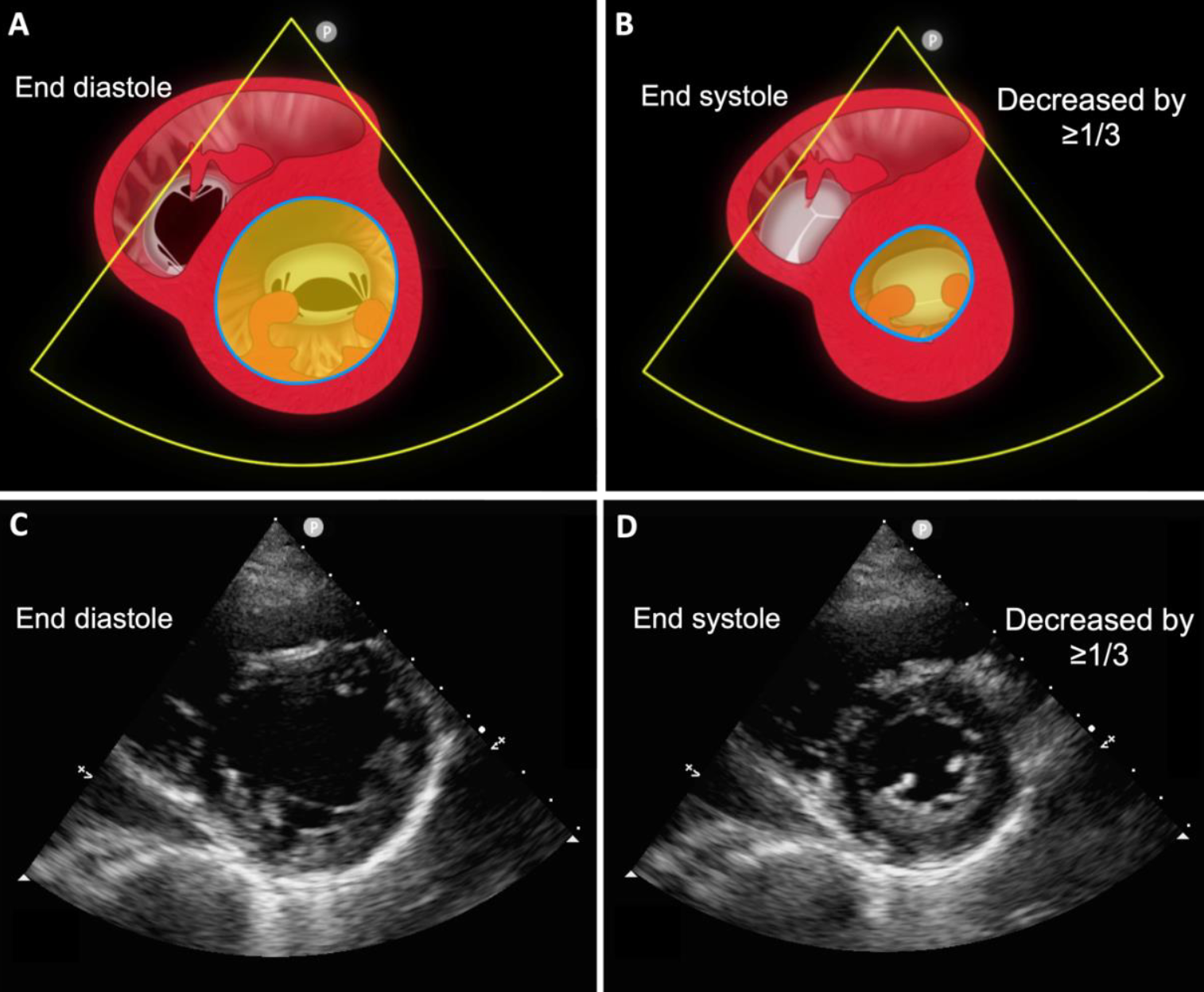
- Best evaluated in the parasternal short axis view but should also be assessed in the parasternal long axis and apical four chamber views
- Review the area enclosed by the endocardial border between end-diastole and end-systole
- A decrease by ≥ 1/3 indicates normal left ventricular systolic function
Sources
- Prada, G., Fritz, A.V., Restrepo-Holguín, M., Guru, P.K., Díaz-Gómez, J.L., 2019. Focused Cardiac Ultrasonography for Left Ventricular Systolic Function. New England Journal of Medicine 381, e36. https://doi.org/10.1056/NEJMvcm1802841
- Basic Transthoracic Echocardiography (Cardiac Ultrasound) - TTE Made Simple - YouTube