Part of: Mechanical Ventilation
Complications from Intubation
- Dental trauma
- Aspiration
- Laryngeal damage
- Bronchospasm
- Oesophageal intubation
- Right main bronchus intubation
Physiological Consequences
Effects on Gas Exchange
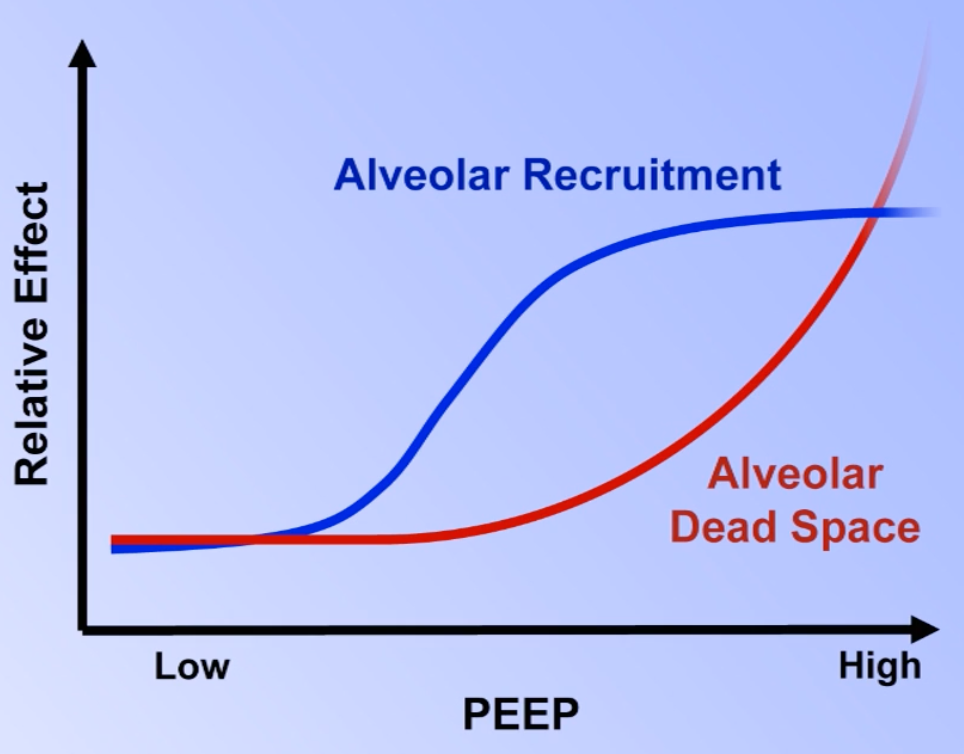
- At low and medium levels of PEEP: ↑ alveolar recruitment → larger surface area for gas diffusion → ↑ oxygenation
- At high levels of PEEP: alveolar dead space increases dramatically
- PEEP has a greater effect on normal compliant alveoli than on stiff/fluid-filled alveoli
- At high PEEP, healthy alveoli become overdistended → ↑ resistance to blood flow → blood shunts towards poorly ventilated alveoli → ↑ physiologic dead space → worsened V/Q mismatch
- High PEEP can also increase pulmonary vascular resistance, worsening intracardiac R-L shunts
Effects on Haemodynamics
- Preload: PEEP can decrease preload because:
- ↑ CVP → ↓ venous return to RA
- ↑ RV afterload → ↓ blood exiting RV
- ↑ RV afterload → leftward displacement of the IV septum → impairs LV diastolic filling
- LV Afterload: PEEP decreases which leads to decreased afterload (as per law of Laplace)
- The effect on cardiac output and blood pressure is highly dependent on volume status:
- Hypovolaemic or euvolaemic → ↓ preload significantly → ↓ cardiac output and blood pressure
- Hypervolaemic → cardiac output increases, blood pressure may increase or remain unchanged
Effects on Monitoring
- High levels of PEEP impair the usual means of assessing cardiac preload (i.e. CVP and PCWP)
- Alternative strategies include:
- Calculating
- With normal lung compliance:
- With abnormal lung compliance:
- Right ventricular end diastolic volume
- Intrathoracic blood volume
- Respiratory variation in aortic blood velocity
- Calculating
Effects on Cerebral Perfusion
- PEEP can in some circumstances decrease cerebral perfusion (variable)
- PEEP increases ICP due to decreased venous return
Auto-PEEP (aka Intrinsic PEEP)
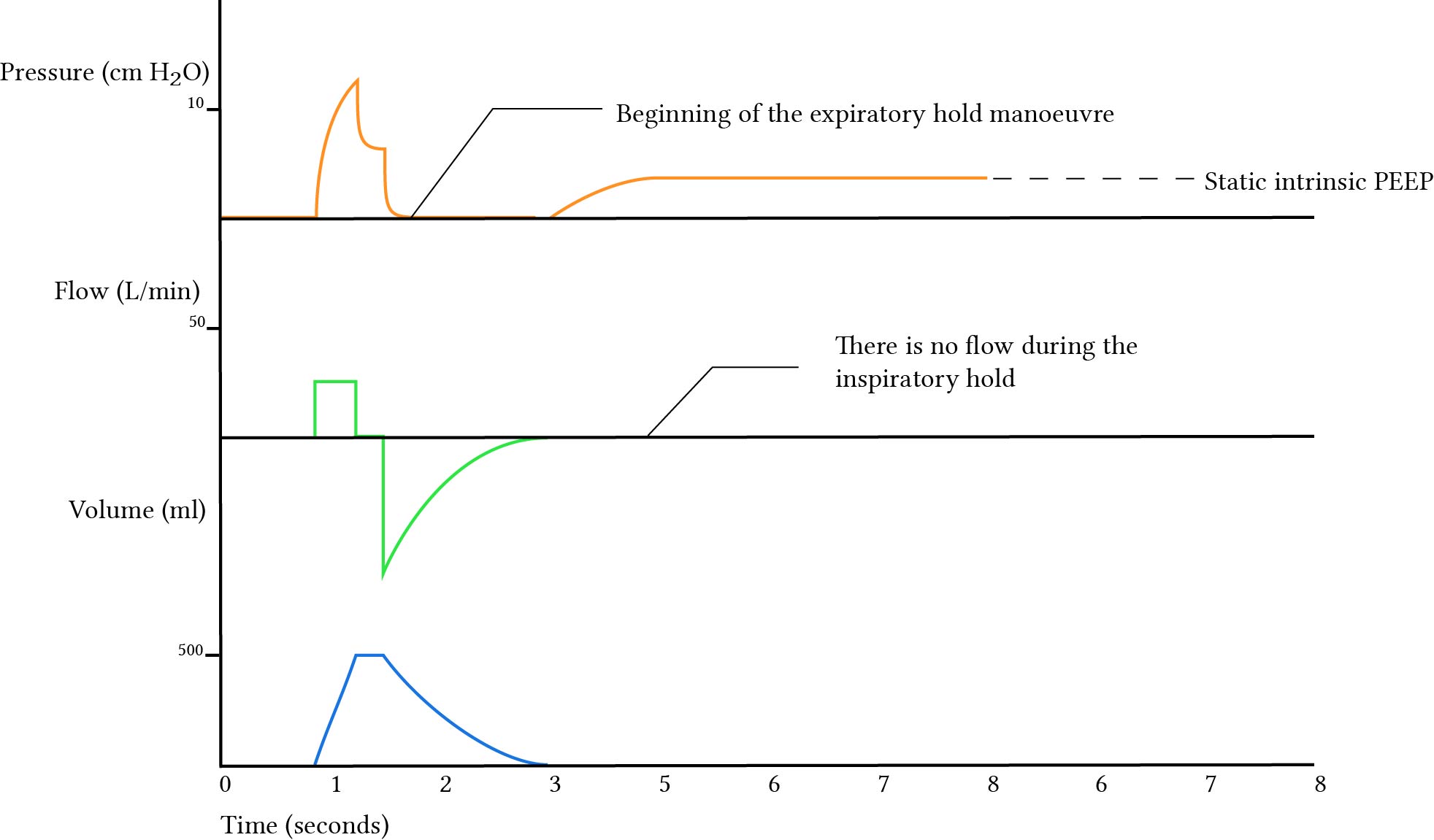
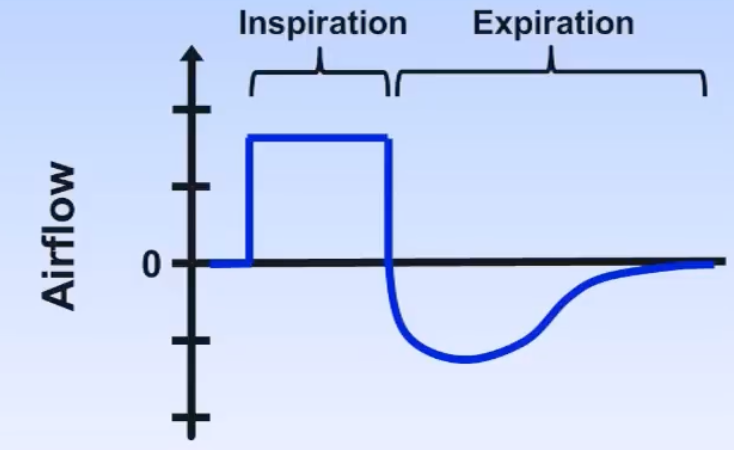
- Auto-PEEP is positive airway pressure that occurs at the end of expiration due to incomplete exhalation
- Consequences include:
- ↑ Risk of barotrauma
- ↓ Venous return → ↓ cardiac output → hypotension
- Worsened V/Q mismatch
- Patient-ventilator dyssynchrony
- ↑ Patient’s work of breathing
Mechanisms
| Mechanism | Examples |
|---|---|
| High minute ventilation | High and/or high respiratory rate |
| Expiratory flow limitation | High airway resistance in COPD |
| Expiratory resistance | Kinked ET tube, patient-ventilator dyssynchrony |
Detection
- Examine for audible air flow extending to the end of expiration on auscultation
- Quantify using an end-expiratory breath hold — the rise in pressure above the applied PEEP represents the auto-PEEP
Treatment
| Mechanism | Treatment |
|---|---|
| High minute ventilation | ↓ , ↓ respiratory rate, or ↓ I:E ratio (permits permissive hypercapnoea) |
| Expiratory flow limitation | Bronchodilators, secretion management, ↑ applied PEEP |
| Expiratory resistance | Upsize ET tube, ↑ sedation, paralytics |
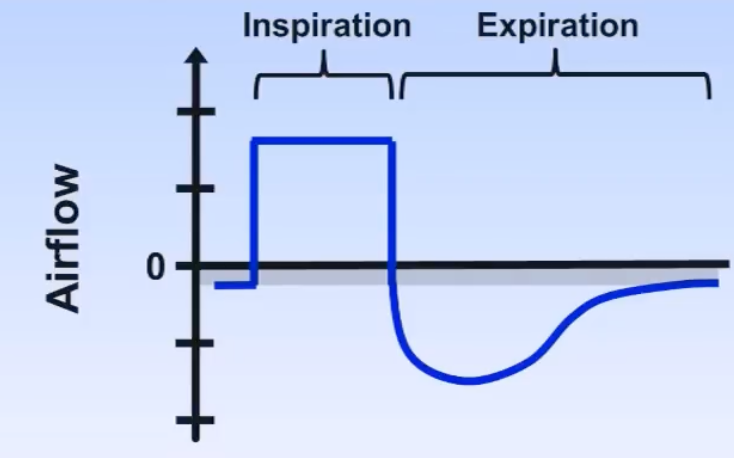
Patient-Ventilator Dyssynchrony
- Dyssynchrony is a state in which the respiratory cycle of the patient does not always match that of the ventilator
- General signs of possible dyssynchrony: increased HR, increased RR, decreased , increased expiratory muscle activity, coughing, agitation and visible inspiratory effort without triggering the ventilator
| Phase | Type | Fix |
|---|---|---|
| Inspiration | Trigger Delay — extra delay between patient effort and ventilator response | ↓ trigger pressure, ↓ sedation, correct electrolytes, bronchodilators, ↑ ETT size, correct auto-PEEP |
| Inspiration | Missed Trigger — insufficient effort to reach threshold | Same as above |
| Inspiration | Auto-Triggering — non-patient signals trigger a breath | ↓ triggering sensitivity, address noise |
| Inspiration | Double Triggering — two breaths delivered for one effort | Usually consequence of premature termination; ↑ inspiratory time |
| Inspiration | Flow Dyssynchrony — flow rate set too low for patient demand (volume control) | ↑ inspiratory flow rate, change flow pattern, change mode |
| Expiration | Delayed Termination — ventilator inspires longer than patient wants | ↑ cycling threshold (earlier), change to time cycling |
| Expiration | Premature Termination — ventilator ceases before patient has finished inspiring | ↓ cycling threshold (later), change to time cycling |
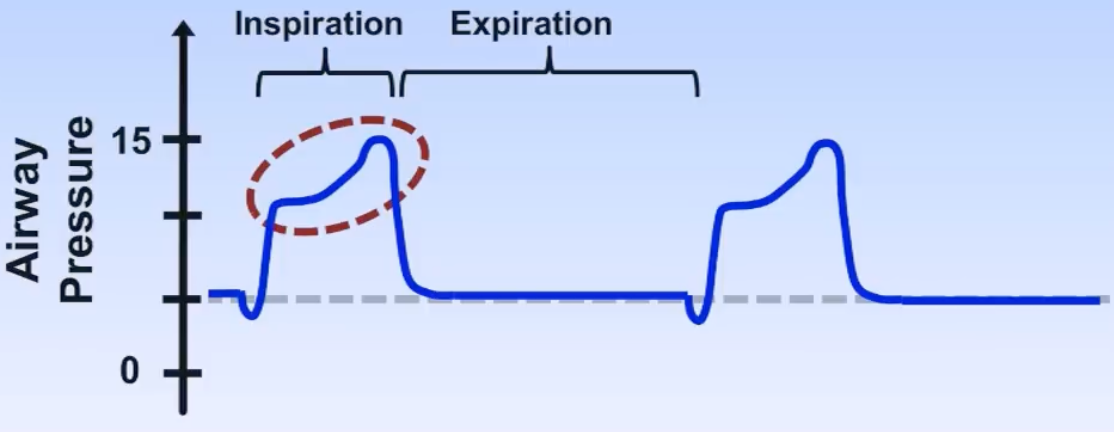
- Delayed termination identified by a sharp spike in airway pressure at the end of inspiration
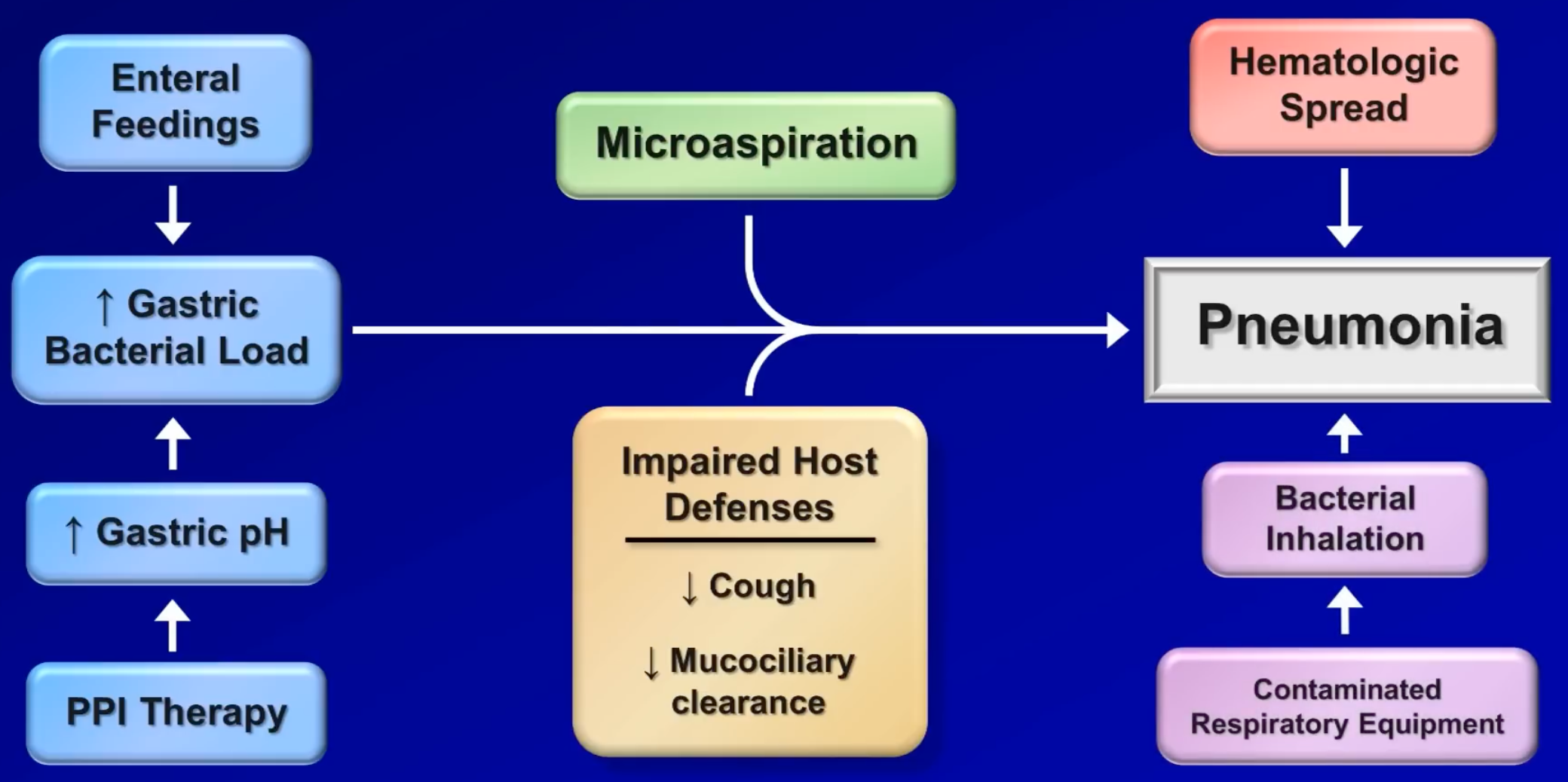
Ventilator-Associated Pneumonia (VAP)
- Any pneumonia that occurs >48 hours after intubation