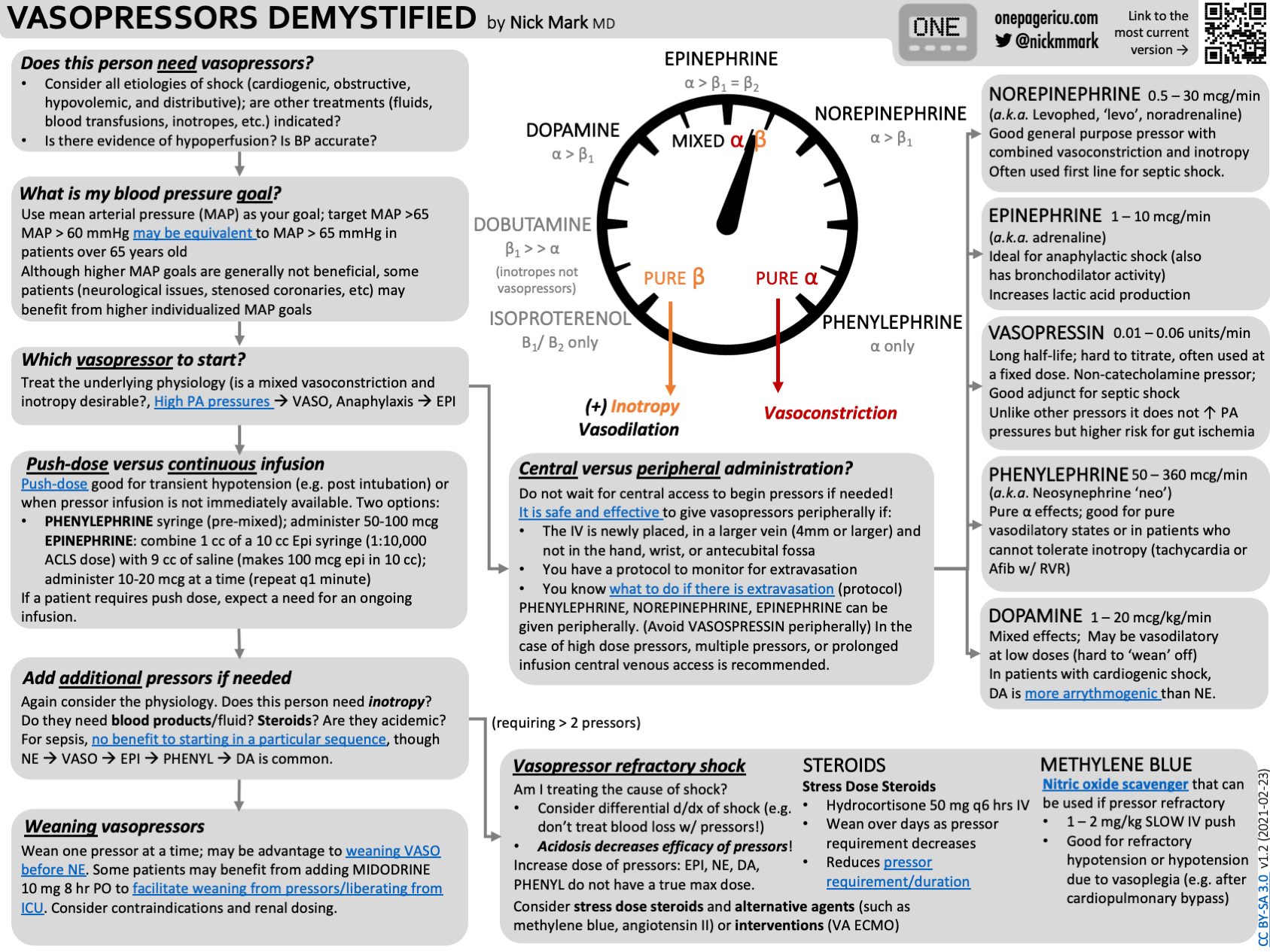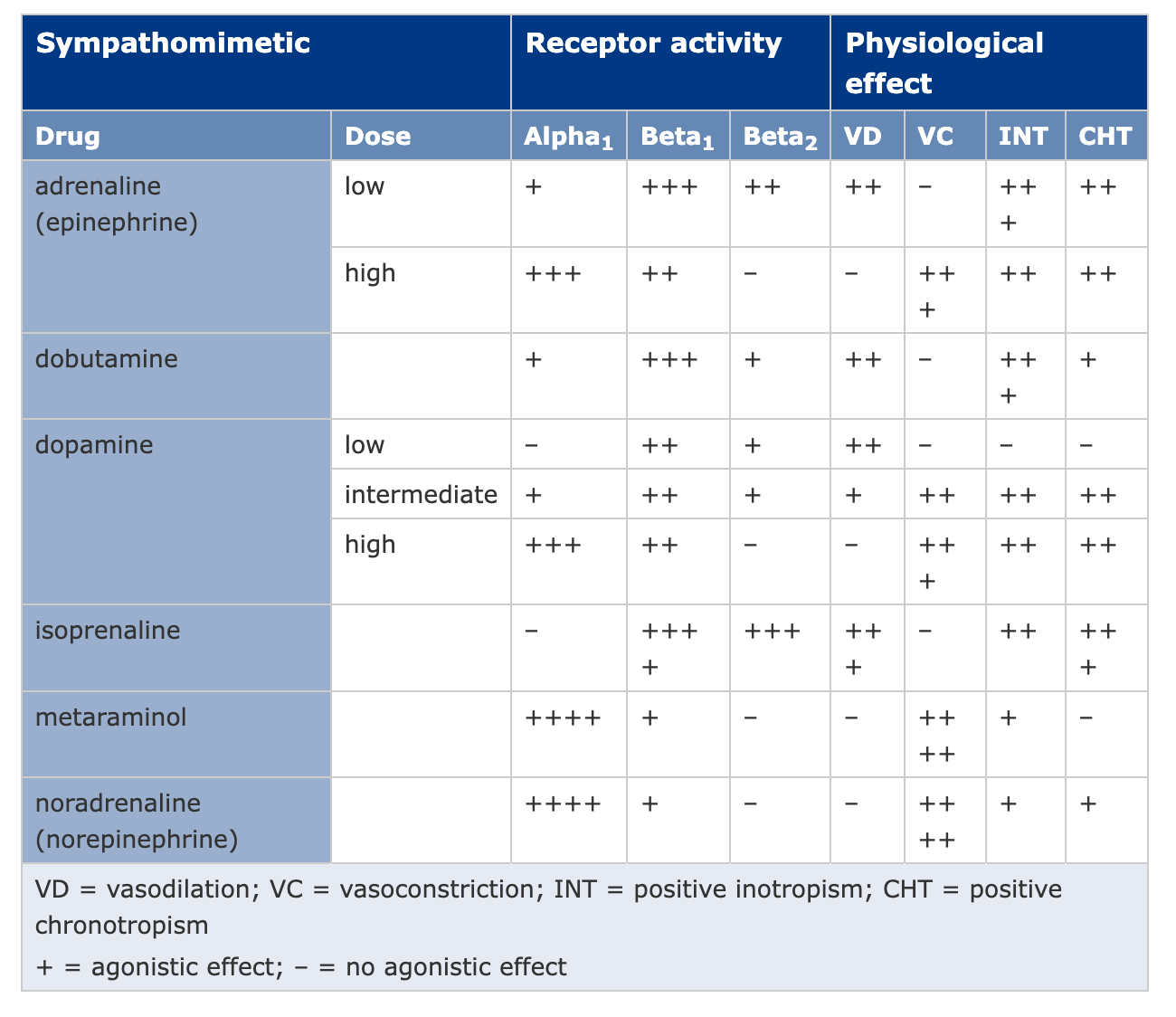
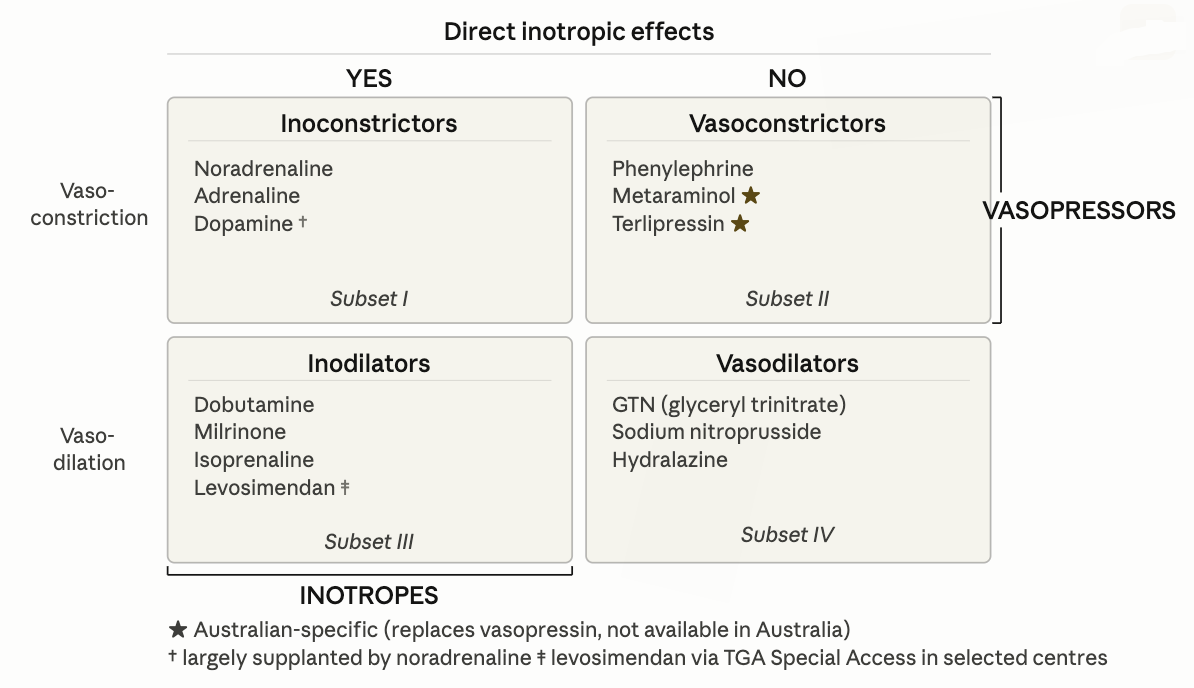
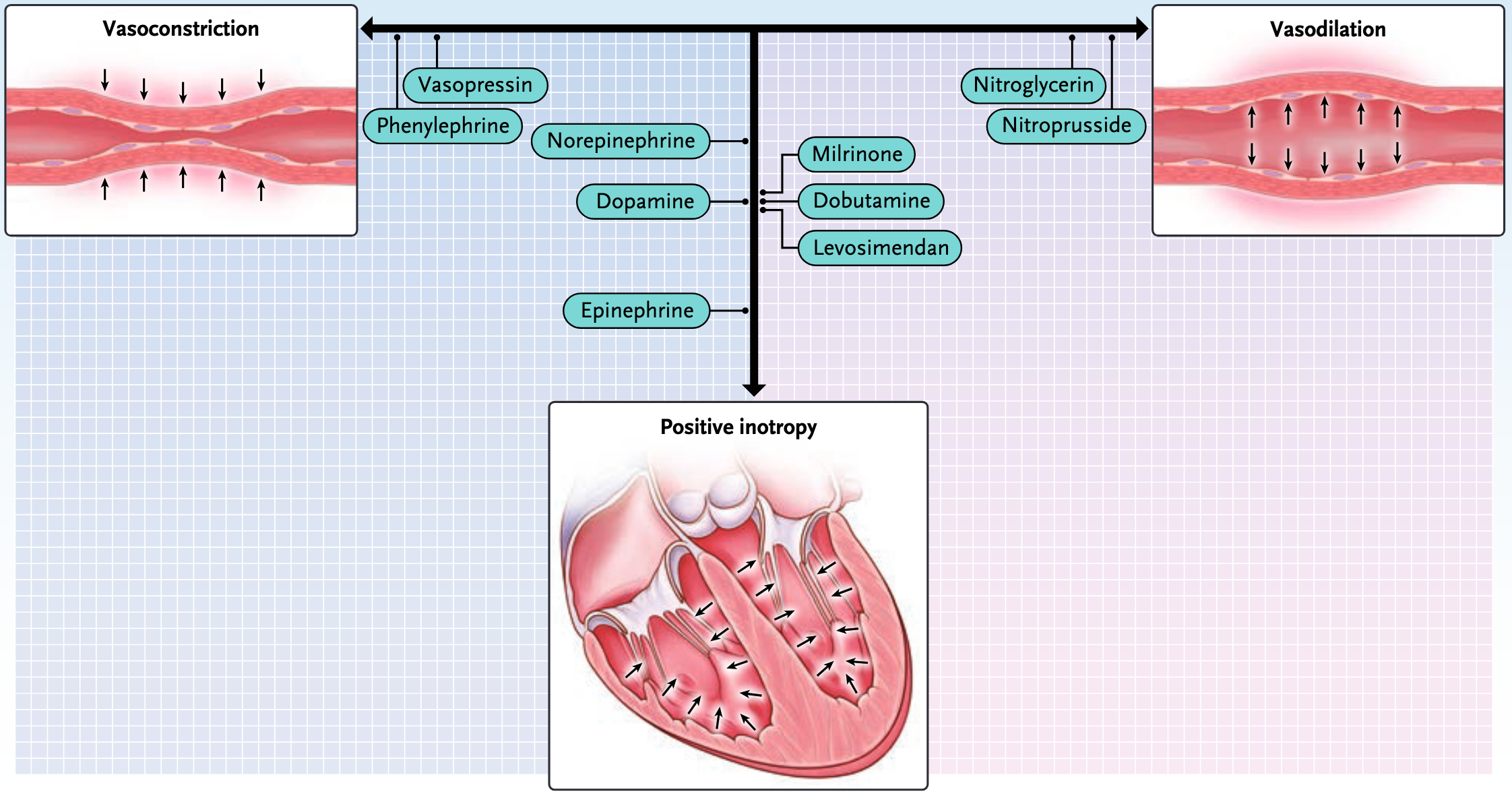
Noradrenaline
0.01-3 mcg/kg/min IV infusion (central line preferred)
First line vasopressor in distributive and most forms of shock
Predominantly agonist with some ⇒ ↑ SVR and mild ↑ HR/CO
Can be run peripherally short-term (forearm or antecubital) at low doses while CVC inserted

Metaraminol
Bolus: 0.5-2 mg IV PRN | Infusion: 15-30 mg in 500 mL at 15-60 mL/hr
Predominantly agonist; also causes indirect noradrenaline release
Used widely in peri-operative setting and as bridge vasopressor pre-noradrenaline
Can be given peripherally; suitable in ward or theatre setting
Tachyphylaxis with prolonged use
Reflex bradycardia can occur - treat with atropine
Less titratable than noradrenaline infusion

Adrenaline
Anaphylaxis: 0.3-0.5 mg IM (thigh) | Shock infusion: 0.01-1 mcg/kg/min IV
Anaphylaxis: IM adrenaline (Epipen 0.3 mg or ampoule 1:1000) is the drug of first choice
Septic shock: Second agent alongside noradrenaline when additional inotropic support needed; associated with increased lactate that does not reflect true worsening
Cardiogenic shock: Adrenaline has more arrhythmogenic risk than other inotropes
Cardiac arrest: 1 mg IV every alternate loop

Terlipressin
Bolus: 0.85–2.5 mg IV bolus q4–6h | Infusion: 1.3–5 mg/24h
- receptor agonist (smooth muscle vasoconstriction)
- Hepatorenal syndrome type 1: terlipressin + albumin is first line
- Variceal bleeding: 2mg IV bolus then 1 mg q4-6h for up to 5 days
- Used in refractory septic shock as noradrenaline-sparing agent (off-label in Australia)
- Risk: digital/skin ischaemia, bradycardia, mesenteric ischaemia — monitor carefully
- Avoid in ischaemic heart disease, peripheral vascular disease
Dobutamine
2–20 mcg/kg/min IV infusion
- and agonist - positive inotropy, chronotropy; reduces SVR (vasodilatory)
- Used in cardiogenic shock with adequate MAP (often combined with noradrenaline)
- Risk of tachycardia and arrhythmia; may worsen hypotension in true hypovolaemia

Milrinone
0.125–0.75 mcg/kg/min IV (load: 25–50 mcg/kg over 10 min, often omitted)
- Used in cardiogenic shock, especially post-cardiac surgery or when β-receptor downregulation limits dobutamine effect
- Useful in pulmonary hypertension (reduces PVR)
- Longer half-life — effects accumulate, harder to titrate; prolonged hypotension if overdosed
- Renally cleared — dose-reduce in AKI
Phenylephrine
Bolus 50–200 mcg IV | Infusion 10–300 mcg/min
Pure α₁ agonist — vasoconstriction without inotropic effect
Useful in tachycardia-associated shock where noradrenaline’s β₁ effect is undesirable (e.g., HOCM, AF with fast ventricular rate)
Reflex bradycardia — use cautiously in bradycardic patients
Can worsen cardiogenic shock by increasing afterload without supporting cardiac output