Subclavian Vein
- Line related infections appear to be lower with the subclavian approach
Contraindications
- Infection of area overlying the target vein
- Thrombosis of the target vein
- Fracture of the clavicle or proximal ribs
- Coagulopathy - applying direct pressure at the subclavian artery or vein is difficult
Method
- Place the patient in a 10-15 trendelenburg position
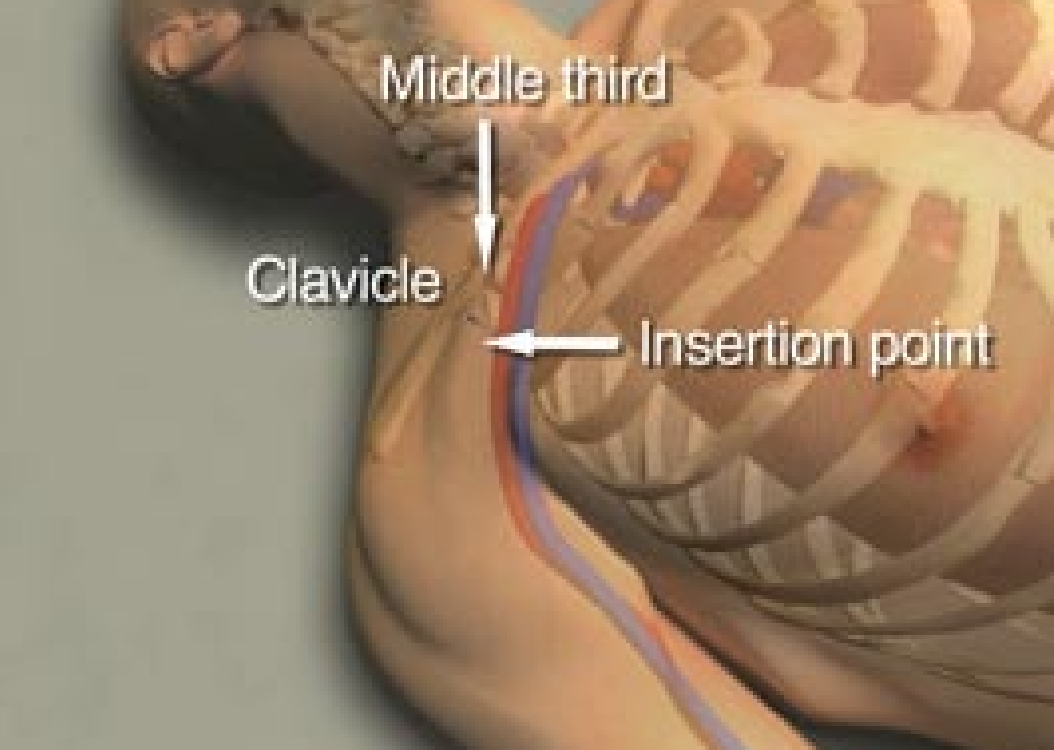
- Turn the head so the chin points away from the vein and place a small role under the scapula to make the calvicle more prominent
- Identify the posterior deviation (middle third) of the clavicle
- Clean and drape the site
- Flush the lines of the central line with heparin or saline
- Ensure the guidewire threads easily through the needle
- Remove the port through which the guidewire will be threaded (commonly the longer lumen)
- Use local anaesthetic to anaesthetise the area
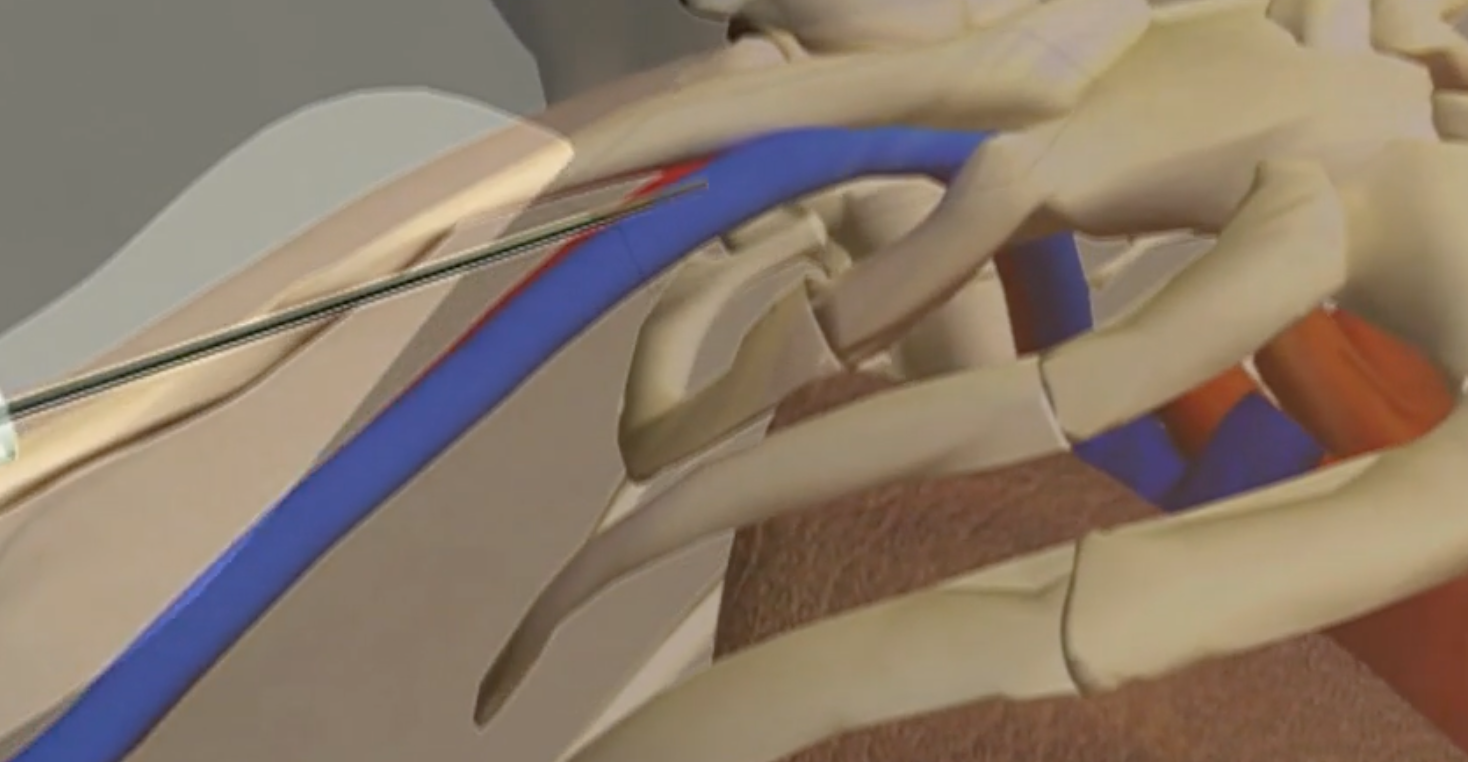
- Approach the site at a 30 degree angle to the skin with the long axis of the needle aimed towards the sternal notch
- Track the needle just below the clavicle
- Feed the wire through the needle
- Have an assistant watch the monitor watching for signs of arrhythmia; if they occur, withdraw the needle until the cease
- Withdraw the needle leaving the guidewire in place
- Make a small superficial incision at the insertion site to facilitate entry of the dilator
- Place the dilator over the wire ensuring to have control over the wire at all times
- Advance the dilator 1-2cm with a rotating motion, being careful not to cause a bend or kink in the wire
- Remove the guidewire and maintain a grip on the wire
- Feed the catheter over the guidewire making sure the end of the guidewire can be seen outside the catheter hub
- Grasp the external end of the guidewire, advance the catheter over the guidewire using a rotating motion
- If the catheter does not advance smoothly, the track may not have been adequately dilated; remove the catheter and insert the dilator
- If it is suspected that the catheter might be in the artery check by connecting to a pressure transducing system
- Remove the guidewire and check for blood return in all ports
- Flush all ports, place caps on the hub and secure the port before removing the drape
- Obtain a chest X-ray to assess for proper placement and ensure no haemothorax nor pneumothorax
Aftercare
- Minimise the number of times the lines is accessed
- Access the line under sterile or clean conditions
- Prepare access site with alcohol based solution
- Reassess need for central line daily
Sources
- Braner, D.A.V., Lai, S., Eman, S., Tegtmeyer, K., 2007. Central Venous Catheterization — Subclavian Vein. New England Journal of Medicine 357, e26. https://doi.org/10.1056/NEJMvcm074357