NOTE
POCUS should only be used in PEA & asystole only. VF and pulseless VT need cardioversion
- Place the probe in the relevant region during CPR to find your window
- Record the image over 8 seconds and interpret once CPR is resumed
- Have a towel in your non-dominant hand to wipe the gel immediately once finished
- Have someone count down from 10 during rhythm check (your probe should come off the patient at the 2 second mark)
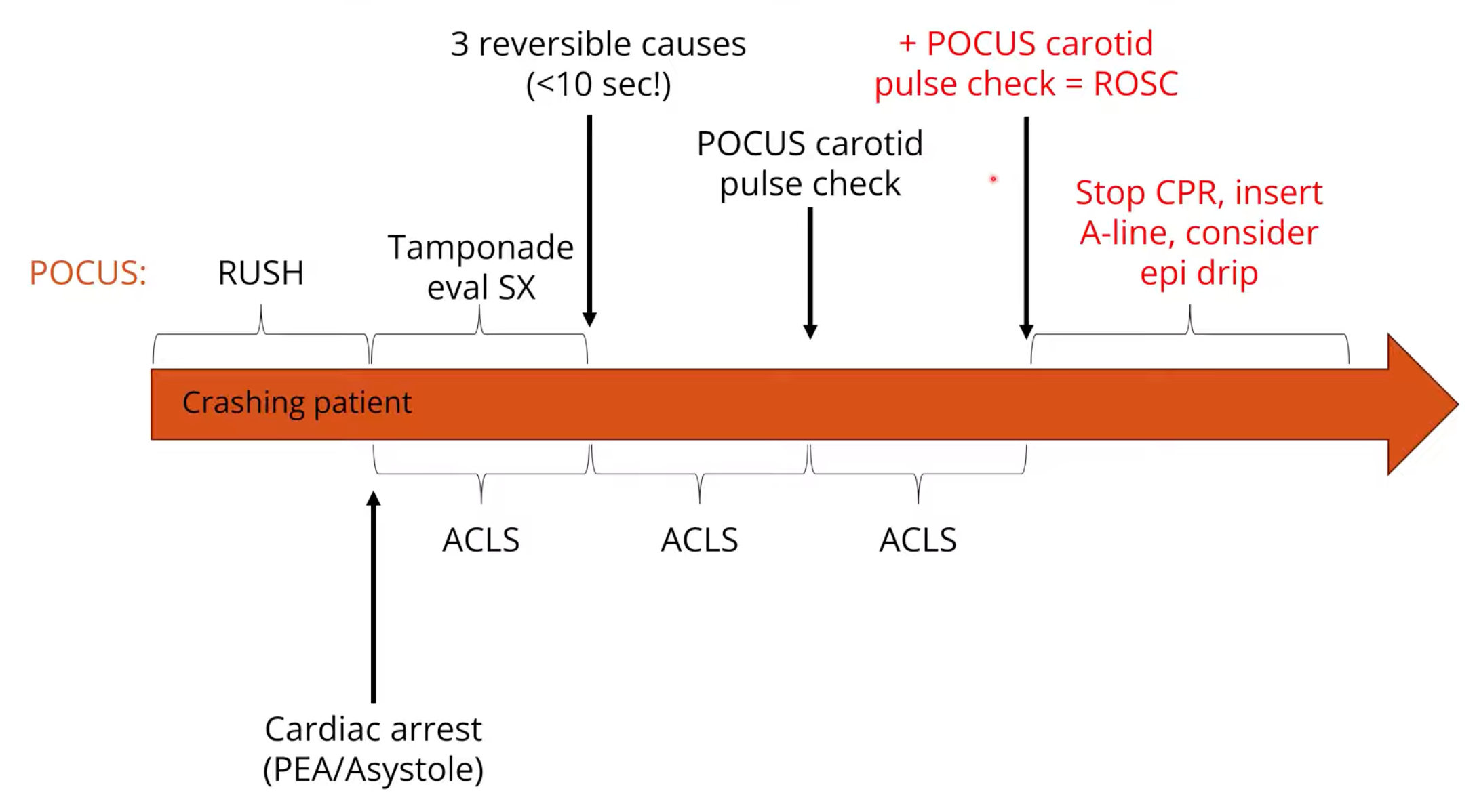
Reversible Causes
- Use a phase array probe in the subcostal/subxiphoid view (or a parasternal long axis but noting you only have about 8s on the chest) during a rhythm check
- Assess for
- Pericardial Effusion/tamponade (this can be assessed during CPR in the sub-xiphoid view)
- RV strain/dilation suggesting massive PE
- However, as soon as 1 minute after the arrest the RV can dilate
- Fine/occult Ventricular Fibrillation suggesting need for cardioversion
- Should see myocardium fibrillating
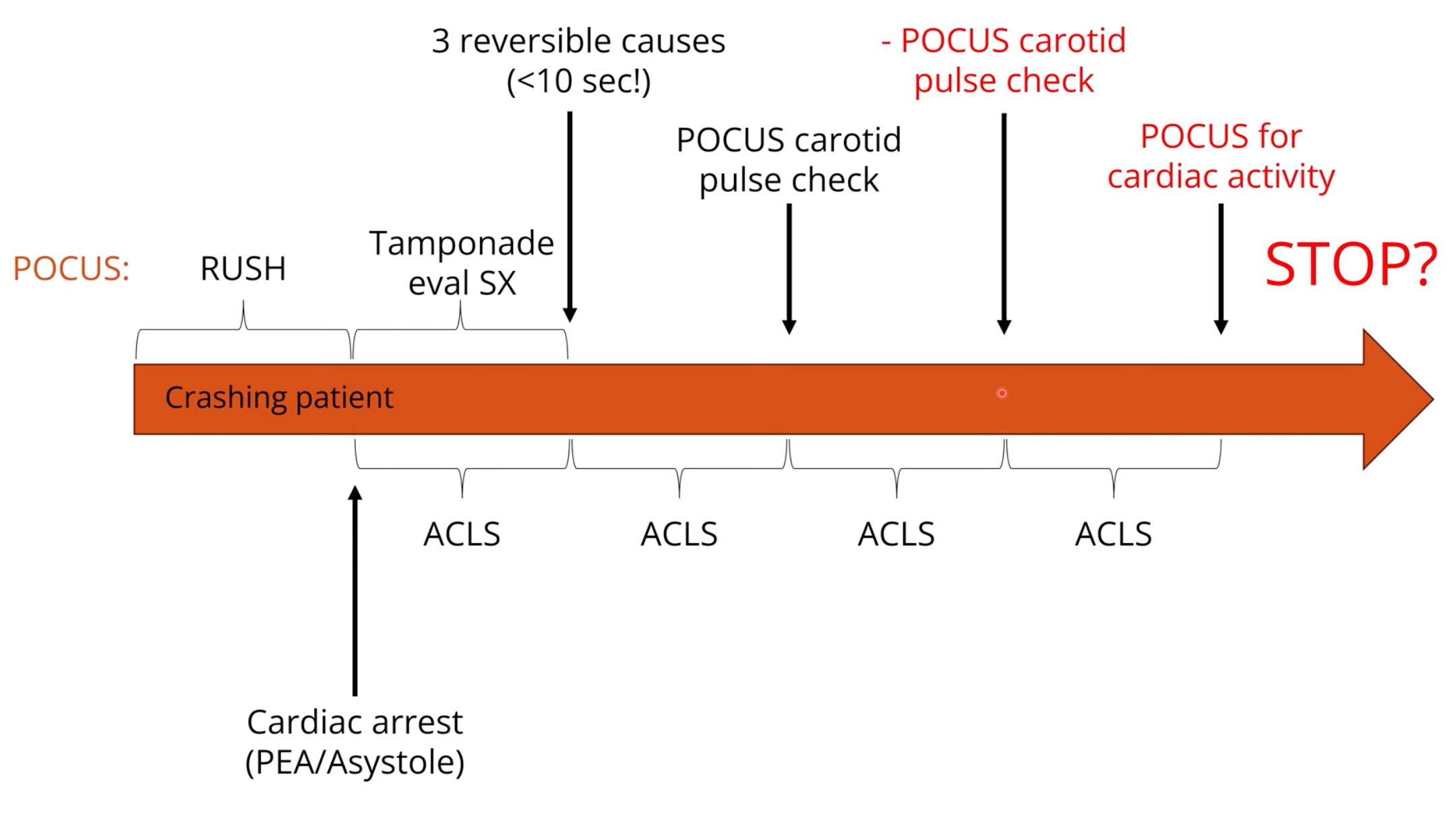
Pulse Checks
- Inferior to arterial line but better than manual palpation
- Perform pulse checks with ultrasound after reversible causes have been ruled
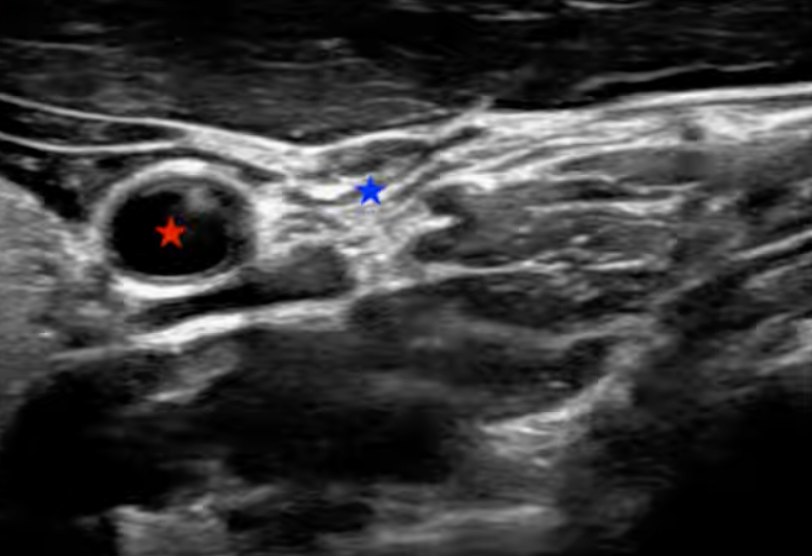
- Use a linear probe transversely in the mid neck
- Identify the carotid artery and use gentle compression until the IJV is compressed
- Look for pulsations indicating a sonographic pulse
Procedures
- For example central line insertion, pericardiocentesis etc.
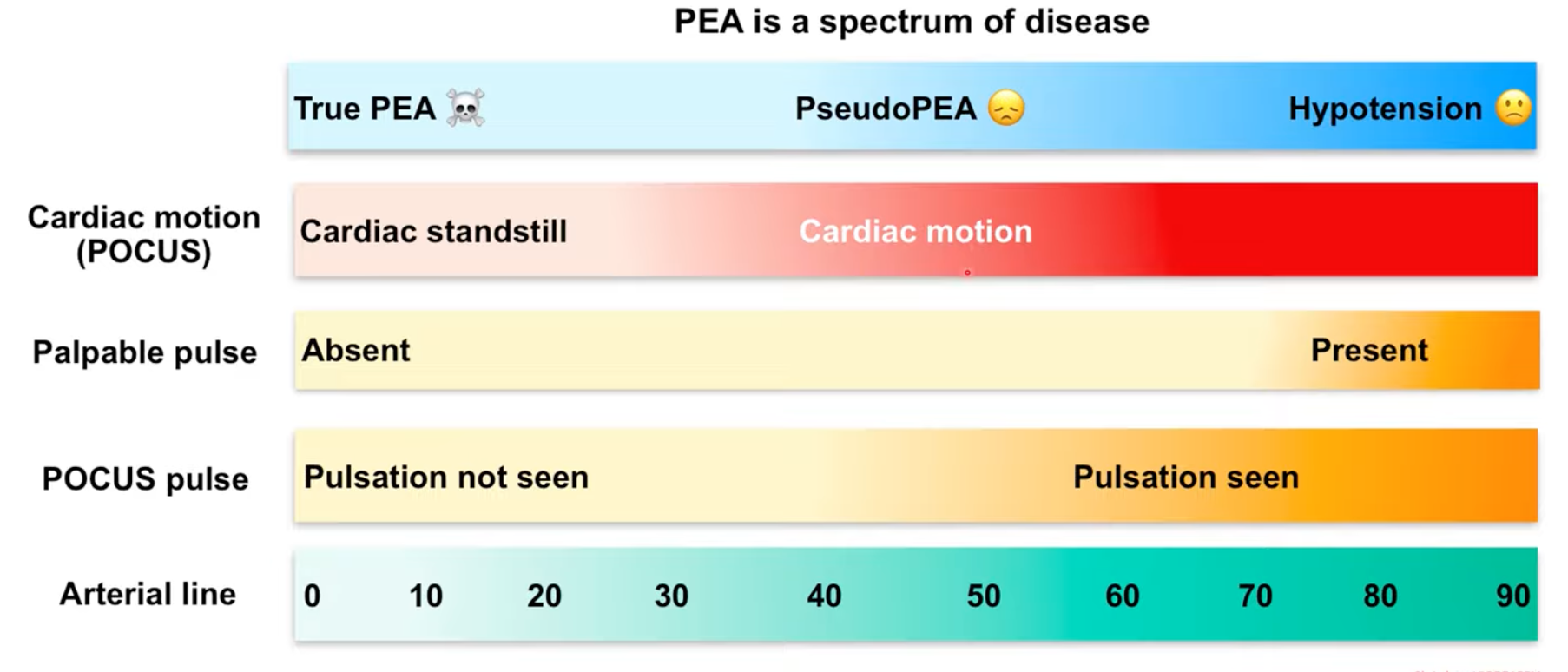
Prognostication
- Cardiac activity on 1st ultrasound suggested a 4% survival to discharge but no cardiac activity on 1st ultrasound suggests <1% survival to discharge
- Defining cardiac activty:
- Organised cardiac activity with a change in size of the ventricular cavity and synchronised movement of the ventricular wall
- Do not use valve movement
- Do not confuse bagging the patient with cardiac activity